
The short-termeffects of cannabis are caused by many chemical compounds in the cannabis plant, including 113 different cannabinoids, such as tetrahydrocannabinol (THC), and 120 terpenes, which allow its drug to have various psychological and physiological effects on the human body. Different plants of the genus Cannabis contain different and often unpredictable concentrations of THC and other cannabinoids and hundreds of other molecules that have a pharmacological effect, so the final net effect cannot reliably be foreseen. Acute effects while under the influence can sometimes include euphoria or anxiety. Although some assert that cannabidiol (CBD), another cannabinoid found in cannabis in varying amounts, may alleviate the adverse effects of THC that some users experience, little is known about CBD's effects on humans. Cannabinoid receptor antagonists have previously been tested as antidotes for cannabis intoxication with success, reducing or eliminating the physiological and psychological effects of intoxication. Some of these products are currently in development as cannabis antidotes.

Medical cannabis, medicinal cannabis or medical marijuana (MMJ) refers to cannabis products and cannabinoid molecules that are prescribed by physicians for their patients. The use of cannabis as medicine has a long history, but has not been as rigorously tested as other medicinal plants due to legal and governmental restrictions, resulting in limited clinical research to define the safety and efficacy of using cannabis to treat diseases.
In the United States, the removal of cannabis from Schedule I of the Controlled Substances Act, the category reserved for drugs that have "no currently accepted medical use", is a proposed legal and administrative change in cannabis-related law at the federal level. After being proposed repeatedly since 1972, the U.S. Department of Justice initiated 2024 rulemaking to reschedule cannabis to Schedule III of the Controlled Substances Act. The majority of 2024 public comments supported descheduling, decriminalizing, or legalizing marijuana at the federal level.

Cannabis, commonly known as marijuana, weed, and pot, among other names, is a non-chemically uniform drug from the cannabis plant. Native to Central or South Asia, the cannabis plant has been used as a drug for both recreational and entheogenic purposes and in various traditional medicines for centuries. Tetrahydrocannabinol (THC) is the main psychoactive component of cannabis, which is one of the 483 known compounds in the plant, including at least 65 other cannabinoids, such as cannabidiol (CBD). Cannabis can be used by smoking, vaporizing, within food, or as an extract.
The National Institute on Drug Abuse (NIDA) is a United States federal government research institute whose mission is to "advance science on the causes and consequences of drug use and addiction and to apply that knowledge to improve individual and public health."
Lester Grinspoon was an American psychiatrist and longstanding associate professor of psychiatry at Harvard University who is best known for his groundbreaking work on the science and social policy of cannabis, psychedelics and other drugs, prompting his ensuing commitment to the reformation of harmful drug policies. He concurrently served as a senior psychiatrist at the Massachusetts Mental Health Center for 40 years. Grinspoon was a fellow of the American Association for the Advancement of Science and the American Psychiatric Association. He was founding editor of The American Psychiatric Association Annual Review and Harvard Mental Health Letter. Grinspoon was editor of Harvard Mental Health Letter for fifteen years.

Different religions have varying stances on the use of cannabis, historically and presently. In ancient history some religions used cannabis as an entheogen, particularly in the Indian subcontinent where the tradition continues on a more limited basis.

Cannabis tea is a cannabis-infused drink prepared by steeping various parts of the cannabis plant in hot or cold water. Cannabis tea is commonly recognized as an alternative form of preparation and consumption of the cannabis plant, more popularly known as marijuana, pot, or weed. This plant has long been recognized as an herbal medicine employed by health professionals worldwide to ease symptoms of disease, as well as a psychoactive drug used recreationally and in spiritual traditions. Though less commonly practiced than popular methods like smoking or consuming edibles, drinking cannabis tea can produce comparable physical and mental therapeutic effects. Such effects are largely attributed to the THC and CBD content of the tea, levels of which are drastically dependent on individual preparation techniques involving volume, amount of cannabis, and boiling time. Also in common with these administration forms of cannabis is the heating component performed before usage. Due to the rather uncommon nature of this particular practice of cannabis consumption in modern times as well as the legality of cannabis throughout the world, the research available on the composition of cannabis tea is limited and based broadly around what is known of cannabis as it exists botanically.
In the United States, the non-medical use of cannabis is legalized in 24 states and decriminalized in 7 states, as of November 2023. Decriminalization refers to a policy of reduced penalties for cannabis offenses, typically involving a civil penalty for possessing small amounts, instead of criminal prosecution or the threat of arrest. In jurisdictions without penalty the policy is referred to as legalization, although the term decriminalization is sometimes used for this purpose as well.
In the United States, increased restrictions and labeling of cannabis as a poison began in many states from 1906 onward, and outright prohibitions began in the 1920s. By the mid-1930s cannabis was regulated as a drug in every state, including 35 states that adopted the Uniform State Narcotic Drug Act. The first national regulation was the Marihuana Tax Act of 1937.
Many urban legends and misconceptions about drugs have been created and circulated among young people and the general public, with varying degrees of veracity. These are commonly repeated by organizations which oppose all classified drug use, often causing the true effects and dangers of drugs to be misunderstood and less scrutinized. The most common subjects of such false beliefs are LSD, cannabis, and PCP. These misconceptions include misinformation about adulterants or other black market issues, as well as alleged effects of the pure substances.
Cannabis consumption refers to the variety of ways cannabis is consumed, among which inhalation and ingestion are most common. All consumption methods involve heating the plant's THCA to decarboxylate it into THC, either at the time of consumption or during preparation. Salves and absorption through the skin (transdermal) are increasingly common in medical uses, both of CBD, THC, and other cannabinoids. Each method leads to subtly different psychoactive effects due to the THC and other chemicals being activated, and then consumed through different administration routes. It is generally considered that smoking, which includes combustion toxins, comes on quickly but lasts for a short period of time, while eating delays the onset of effect but the duration of effect is typically longer. In a 2007 ScienceDaily report of research conducted at the University of California–San Francisco, researchers reported that vaporizer users experience the same biological effect, but without the toxins associated with smoking. Δ9-THC is the primary component when inhaled, but when eaten the liver converts this to the more psychoactive 11-hydroxy-THC form.
The use, sale, and possession of cannabis containing over 0.3% THC by dry weight in the United States, despite laws in many states permitting it under various circumstances, is illegal under federal law. As a Schedule I drug under the federal Controlled Substances Act (CSA) of 1970, cannabis containing over 0.3% THC by dry weight is considered to have "no accepted medical use" and a high potential for abuse and physical or psychological dependence. Cannabis use is illegal for any reason, with the exception of FDA-approved research programs. However, individual states have enacted legislation permitting exemptions for various uses, including medical, industrial, and recreational use.
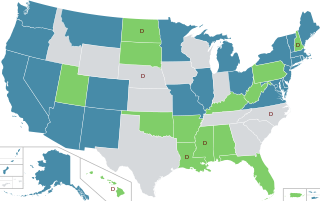
In the United States, the use of cannabis for medical purposes is legal in 38 states, four out of five permanently inhabited U.S. territories, and the District of Columbia, as of March 2023. Ten other states have more restrictive laws limiting THC content, for the purpose of allowing access to products that are rich in cannabidiol (CBD), a non-psychoactive component of cannabis. There is significant variation in medical cannabis laws from state to state, including how it is produced and distributed, how it can be consumed, and what medical conditions it can be used for.

A psychoactive drug, mind-altering drug, or consciousness-altering drug is a chemical substance that changes brain function and results in alterations in perception, mood, consciousness, cognition, or behavior. The term psychotropic drug is often used interchangeably, while some sources present narrower definitions. These substances may be used medically; recreationally; to purposefully improve performance or alter consciousness; as entheogens for ritual, spiritual, or shamanic purposes; or for research, including psychedelic therapy. Physicians and other healthcare practitioners prescribe psychoactive drugs from several categories for therapeutic purposes. These include anesthetics, analgesics, anticonvulsant and antiparkinsonian drugs as well as medications used to treat neuropsychiatric disorders, such as antidepressants, anxiolytics, antipsychotics, and stimulants. Some psychoactive substances may be used in detoxification and rehabilitation programs for persons dependent on or addicted to other psychoactive drugs.
In Judaism, there is debate that cannabis may have been used ritually in ancient Judaism, and the use of cannabis continues to be a controversial topic in modern Judaism.

Terms related to cannabis include:
Two main questions arise in the law surrounding driving after having ingested cannabis: (1) whether cannabis actually impairs driving ability, and (2) whether the common practice of testing for THC is a reliable means to measure impairment. On the first question, studies are mixed. Several recent, extensive studies–including one conducted by the National Highway Traffic Safety Administration and one conducted by the American Automobile Association (AAA)–show that drivers with detectable THC in their blood are no more likely to cause car crashes than drivers with no amount of THC in their blood. Others show that cannabis can impair certain abilities important to safe driving –but no studies have been able to show that this increases the actual risk of crashing, or that drivers with THC in their blood cause a disproportionate number of crashes. On the second question, the studies that have been conducted so far have consistently found that THC blood levels and degree of impairment are not closely related. No known relationship between blood levels of THC and increased relative crash risk, or THC blood levels and level of driving impairment, has been shown by single-crash or classic-control studies. Thus, even though it is possible that cannabis impairs driving ability to some extent, there are currently no reliable means to test or measure whether a driver was actually impaired.
Occupational health concerns over the use of cannabis among workers are becoming increasingly important as cannabis becomes legal in more areas of the US. Of note, employers have concerns of workers either coming to work acutely impaired or recent use of cannabis still being detected in the body. Employment issues such as ADA law as it relates to accommodations for cannabis, paying unemployment benefits or paying out workers compensation benefits and disability claims are all important issues. While federal law still prohibits use, employers in different states have taken different stances based on whether they are federal contractors, perform safety sensitive work or whether the cannabis use is acutely impairing the employee.
