Recreational drug use is the use of one or more psychoactive drugs to induce an altered state of consciousness, either for pleasure or for some other casual purpose or pastime. When a psychoactive drug enters the user's body, it induces an intoxicating effect. Recreational drugs are commonly divided into three categories: depressants, stimulants, and hallucinogens.

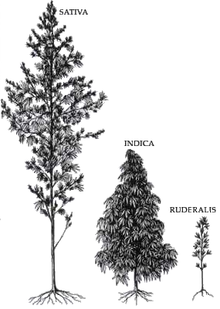
Cannabis is a genus of flowering plants in the family Cannabaceae. The number of species within the genus is disputed. Three species may be recognized: Cannabis sativa, C. indica, and C. ruderalis. Alternatively, C. ruderalis may be included within C. sativa, all three may be treated as subspecies of C. sativa, or C. sativa may be accepted as a single undivided species. The genus is widely accepted as being indigenous to and originating from Asia.
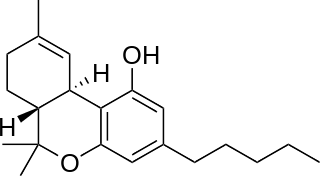
Tetrahydrocannabinol (THC) is a cannabinoid found in cannabis. It is the principal psychoactive constituent of cannabis and one of at least 113 total cannabinoids identified on the plant. Its chemical formula C21H30O2 includes compounds, the term THC usually refers to the delta-9-THC isomer with chemical name (−)-trans-Δ9-tetrahydrocannabinol. It is a colorless oil.

A cannabis edible, also known as a cannabis-infused food or simply an edible, is a food item that contains decarboxylated cannabinoids from cannabis extract as an active ingredient. Although edible may refer to either a food or a drink, a cannabis-infused drink may be referred to more specifically as a liquid edible or drinkable. Edibles are a way to consume cannabis. Unlike smoking, in which cannabinoids are inhaled into the lungs and pass rapidly into the bloodstream, peaking in about ten minutes and wearing off in a couple of hours, cannabis edibles may take hours to digest, and their effects may peak two to three hours after consumption and persist for around six hours. The food or drink used may affect both the timing and potency of the dose ingested.

The effects of cannabis are caused by chemical compounds in the cannabis plant, including 113 different cannabinoids such as tetrahydrocannabinol (THC) and 120 terpenes, which allow its drug to have various psychological and physiological effects on the human body. Different plants of the genus Cannabis contain different and often unpredictable concentrations of THC and other cannabinoids and hundreds of other molecules that have a pharmacological effect, so the final net effect cannot reliably be foreseen.

Medical cannabis, or medical marijuana (MMJ), is cannabis and cannabinoids that are prescribed by physicians for their patients. The use of cannabis as medicine has not been rigorously tested due to production and governmental restrictions, resulting in limited clinical research to define the safety and efficacy of using cannabis to treat diseases.
Cannabinoids are several structural classes of compounds found in the cannabis plant primarily and most animal organisms or as synthetic compounds. The most notable cannabinoid is the phytocannabinoid tetrahydrocannabinol (THC) (delta-9-THC), the primary psychoactive compound in cannabis. Cannabidiol (CBD) is also a major constituent of temperate cannabis plants and a minor constituent in tropical varieties. At least 113 distinct phytocannabinoids have been isolated from cannabis, although only four have been demonstrated to have a biogenetic origin. It was reported in 2020 that phytocannabinoids can be found in other plants such as rhododendron, licorice and liverwort, and earlier in Echinacea.

A vaporizer or vaporiser, colloquially known as a vape, is a device used to vaporize substances for inhalation. Plant substances can be used, commonly cannabis, tobacco, or other herbs or blends of essential oil. However, they are most commonly filled with a combination propylene glycol, glycerin, and drugs such as nicotine or tetrahydrocannabinol as a liquid solution.
The gateway drug effect is a comprehensive catchphrase for the often observed effect that the use of a psychoactive substance is coupled to an increased probability of the use of further substances. Possible reasons for the connection include environmental influence, impulsive people seeking both soft and hard drugs, alterations in the brain due to earlier substance exposure, as well as similar attitudes of people who use different substances, and therefore experience a "common liability to addiction". In 2020, the National Institute on Drug Abuse released a research report which supported allegations that marijuana is a "gateway" to more dangerous substance use; one of the peer-reviewed papers cited in the report claims that while "some studies have found that use of legal drugs or cannabis are not a requirement for the progression to other illicit drugs [...] most studies have supported the "gateway sequence"." However, a 2018 literature review conducted by the National Institute of Justice, which analyzed 23 peer-reviewed research studies, concluded "that existing statistical research and analysis relevant to the "gateway" hypothesis has produced mixed results", and that "no causal link between cannabis use and the use of other illicit drugs can be claimed at this time."

Cannabis tea is a cannabis-infused drink prepared by steeping various parts of the cannabis plant in hot or cold water. Cannabis tea is commonly recognized as an alternative form of preparation and consumption of the cannabis plant, more popularly known as marijuana, pot, or weed. This plant has long been recognized as an herbal medicine employed by health professionals worldwide to ease symptoms of disease, as well as a psychoactive drug used recreationally and in spiritual traditions. Though less commonly practiced than popular methods like smoking or consuming edibles, drinking cannabis tea can produce comparable physical and mental therapeutic effects. Such effects are largely attributed to the THC and CBD content of the tea, levels of which are drastically dependent on individual preparation techniques involving volume, amount of cannabis, and boiling time. Also in common with these administration forms of cannabis is the heating component performed before usage. Due to the rather uncommon nature of this particular practice of cannabis consumption in modern times as well as the legality of cannabis throughout the World, the research available on the composition of cannabis tea is limited and based broadly around what is known of cannabis as it exists botanically.

Cannabis smoking is the inhalation of smoke or vapor released by heating the flowers, leaves, or extracts of cannabis and releasing the main psychoactive chemical, Δ9-tetrahydrocannabinol (THC), which is absorbed into the bloodstream via the lungs. Archaeological evidence indicates cannabis with high levels of THC was being smoked at least 2,500 years ago. As of 2021, cannabis is the most commonly consumed federally illegal drug in the United States, with 36.4 million people consuming it monthly.
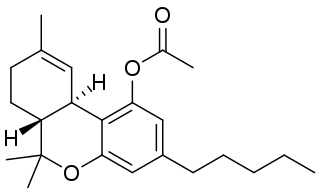
THC-O-acetate is the acetate ester of THC. The term THC-O-acetate and its variations are commonly used for two types of the substance, dependent on which cannabinoid it is synthesized from. The difference between Δ8-THC and Δ9-THC is bond placement on the cyclohexene ring.
Cannabis consumption refers to the variety of ways cannabis is consumed, among which inhalation and ingestion are most common. All consumption methods involve heating the plant's THCA to decarboxylate it into THC, either at the time of consumption or during preparation. Salves and absorption through the skin (transdermal) are increasingly common in medical uses, both of CBD, THC, and other cannabinoids. Each method leads to subtly different psychoactive effects due to the THC and other chemicals being activated, and then consumed through different administration routes. It is generally considered that smoking, which includes combustion toxins, comes on quickly but lasts for a short period of time, while eating delays the onset of effect but the duration of effect is typically longer. In a 2007 ScienceDaily report of research conducted at the University of California–San Francisco, researchers reported that vaporizer users experience the same biological effect, but without the toxins associated with smoking. Δ9-THC is the primary component when inhaled, but when eaten the liver converts this to the more psychoactive 11-hydroxy-THC form.
Cannabis strains are either pure or hybrid varieties of the plant genus Cannabis, which encompasses the species C. sativa, C. indica, and C. ruderalis.

Synthetic cannabinoids are a class of designer drug molecules that bind to the same receptors to which cannabinoids in cannabis plants attach. These novel psychoactive substances should not be confused with synthetic phytocannabinoids or synthetic endocannabinoids from which they are in many aspects distinct.
Dronabinol (INN), also known under the trade names Marinol and Syndros, is a generic name for the molecule of delta-9-tetrahydrocannabinol in the pharmaceutical context. It has indications as an appetite stimulant, antiemetic, and sleep apnea reliever and is approved by the FDA as safe and effective for HIV/AIDS-induced anorexia and chemotherapy-induced nausea and vomiting only.
The long-term effects of cannabis have been the subject of ongoing debate. Given that the use of cannabis is illegal in most countries, clinical research presents a challenge and there is limited evidence from which to draw conclusions. In 2017, the U.S. National Academies of Sciences, Engineering, and Medicine issued a report summarizing much of the published literature on health effects of cannabis, into categories regarded as conclusive, substantial, moderate, limited and of no or insufficient evidence to support an association with a particular outcome.

Cannabis use disorder (CUD), also known as cannabis addiction or marijuana addiction, is a psychiatric disorder defined in the fifth revision of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) and ICD-10 as the continued use of cannabis despite clinically significant impairment.
Two main questions arise in the law surrounding driving after having ingested cannabis: (1) whether cannabis actually impairs driving ability, and (2) whether the common practice of testing for THC is a reliable means to measure impairment. On the first question, studies are mixed. Several recent, extensive studies–including one conducted by the National Highway Traffic Safety Administration and one conducted by the American Automobile Association (AAA)–show that drivers with detectable THC in their blood are no more likely to cause car crashes than drivers with no amount of THC in their blood. Others show that cannabis can impair certain abilities important to safe driving –but no studies have been able to show that this increases the actual risk of crashing, or that drivers with THC in their blood cause a disproportionate number of crashes. On the second question, the studies that have been conducted so far have consistently found that THC blood levels and degree of impairment are not closely related. No known relationship between blood levels of THC and increased relative crash risk, or THC blood levels and level of driving impairment, has been shown by single-crash or classic-control studies. Thus, even though it is possible that cannabis impairs driving ability to some extent, there are currently no reliable means to test or measure whether a driver was actually impaired.
Cannabis use and trauma is the contribution that trauma plays in promoting the use and potential abuse of cannabis. Conversely, cannabis use has been associated with the intensity of trauma and PTSD symptoms. While evidence of efficacious use of cannabis is growing in novelty, it is not currently recommended.





 Dried flower buds (marijuana)
Dried flower buds (marijuana) A gram of kief
A gram of kief Hashish
Hashish Hash oil
Hash oil Infusion (dairy butter)
Infusion (dairy butter)