Lysergic acid diethylamide, commonly known as LSD (from German Lysergsäure-diethylamid), is a potent psychedelic drug that intensifies thoughts, emotions, and sensory perception.[12] Often referred to as acid or lucy, LSD can cause mystical, spiritual, or religious experiences.[13][14] At higher doses, it primarily induces visual and auditory hallucinations.[15][16] LSD is not considered addictive, because it does not produce compulsive drug-seeking behavior. Using LSD can lead to adverse psychological reactions, such as anxiety, paranoia, and delusions.[7] Additionally, it may trigger "flashbacks," also known as hallucinogen persisting perception disorder (HPPD), where individuals experience persistent visual distortions after use.[17][18]
The effects of LSD begin within 30 minutes of ingestion and can last up to 20 hours, with most trips averaging 8–12 hours.[19][20] It is synthesized from lysergic acid and commonly administered via tabs of blotter paper.[21] LSD is mainly used recreationally or for spiritual purposes.[19][22] As a serotonin receptor agonist, LSD's precise effects are not fully understood, but it is known to alter the brain’s default mode network, leading to its powerful psychedelic effects.[12][23][24]
Despite its legal restrictions, LSD remains influential in scientific and cultural contexts. Its therapeutic potential has been explored, particularly in treating mental health disorders.[12][27] As of 2017, about 10% of people in the U.S. had used LSD at some point, with 0.7% having used it in the past year.[28] Usage rates have risen, with a 56.4% increase in adult use in the U.S. from 2015 to 2018.[29]
The primary immediate psychological effects of LSD are visual pseudo-hallucinations and altered thought, often referred to as "trips". These sensory alterations are considered pseudohallucinations because the subject does not perceive the patterns seen as being located in three-dimensional space outside the body.[43] LSD is not considered addictive. These effects typically begin within 20–30 minutes of oral ingestion, peak three to four hours after ingestion, and can last up to 20 hours, particularly with higher doses. An "afterglow" effect, characterized by an improved mood or perceived mental state, may persist for days or weeks following ingestion.[44] Positive experiences, or "good trips", are described as intensely pleasurable and can include feelings of joy, euphoria, an increased appreciation for life, decreased anxiety, a sense of spiritual enlightenment, and a feeling of interconnectedness with the universe.[45][46]
Negative experiences, commonly known as "bad trips", can induce feelings of fear, agitation, anxiety, panic, and paranoia.[7][47] While the occurrence of a bad trip is unpredictable, factors such as mood, surroundings, sleep, hydration, and social setting, collectively referred to as "set and setting", can influence the risk and are considered important in minimizing the likelihood of a negative experience.[48][49]
Sensory
LSD induces an animated sensory experience affecting senses, emotions, memories, time, and awareness, lasting from 6 to 20 hours, with the duration dependent on dosage and individual tolerance. Effects typically commence within 30 to 90 minutes post-ingestion, ranging from subtle perceptual changes to profound cognitive shifts. Alterations in auditory and visual perception are common.[50][51]
Users may experience enhanced visual phenomena, such as vibrant colors, objects appearing to morph, ripple or move, and geometric patterns on various surfaces. Changes in the perception of food's texture and taste are also noted, sometimes leading to aversion towards certain foods.[50][52]
There are reports of inanimate objects appearing animated, with static objects seeming to move in additional spatial dimensions.[53] The auditory effects of LSD may include echo-like distortions of sounds, and an intensified experience of music. Basic visual effects often resemble phosphenes and can be influenced by concentration, thoughts, emotions, or music.[54] Higher doses can lead to more intense sensory perception alterations, including synesthesia, perception of additional dimensions, and temporary dissociation.
Adverse effects
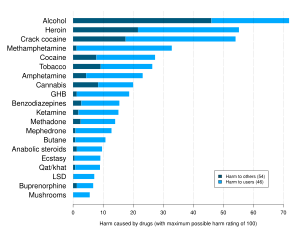
Table from the 2010 ISCD study ranking various drugs (legal and illegal) based on statements by drug-harm experts. LSD was found to be the 18th most dangerous out of 20 considered.Addiction experts in psychiatry, chemistry, pharmacology, forensic science, epidemiology, and the police and legal services engaged in delphic analysis regarding 20 popular recreational drugs. LSD was ranked 14th in dependence, 15th in physical harm, and 13th in social harm.
LSD, a classical psychedelic, is deemed physiologically safe at standard dosages (50–200 μg) and its primary risks lie in psychological effects rather than physiological harm.[23][57] A 2010 study by David Nutt ranked LSD as significantly less harmful than alcohol, placing it near the bottom of a list assessing the harm of 20 drugs.[58]
Psychological effects
Mental disorders
LSD can induce panic attacks or extreme anxiety, colloquially termed a "bad trip". Despite lower rates of depression and substance abuse found in psychedelic drug users compared to controls, LSD presents heightened risks for individuals with severe mental illnesses like schizophrenia.[59][60] These hallucinogens can catalyze psychiatric disorders in predisposed individuals, although they do not tend to induce illness in emotionally healthy people.[23]
Suggestibility
While research from the 1960s indicated increased suggestibility under the influence of LSD among both mentally ill and healthy individuals, recent documents suggest that the CIA and Department of Defense have discontinued research into LSD as a means of mind control.[61][62][63][non-primary source needed]
Flashbacks
Flashbacks are psychological episodes where individuals re-experience some of LSD's subjective effects after the drug has worn off, persisting for days or months post-hallucinogen use.[64][65] These experiences are associated with hallucinogen persisting perception disorder (HPPD), where flashbacks occur intermittently or chronically, causing distress or functional impairment.[18]
The etiology of flashbacks is varied. Some cases are attributed to somatic symptom disorder, where individuals fixate on normal somatic experiences previously unnoticed prior to drug consumption.[66] Other instances are linked to associative reactions to contextual cues, similar to responses observed in individuals with past trauma or emotional experiences.[67] The risk factors for flashbacks remain unclear, but pre-existing psychopathologies may be significant contributors.[68]
Estimating the prevalence of HPPD is challenging. It is considered rare, with occurrences ranging from 1 in 20 users experiencing the transient and less severe type 1 HPPD, to 1 in 50,000 for the more concerning type 2 HPPD.[18] Contrary to internet rumors, LSD is not stored long-term in the spinal cord or other body parts. Pharmacological evidence indicates LSD has a half-life of 175 minutes and is metabolized into water-soluble compounds like 2-oxo-3-hydroxy-LSD, eliminated through urine without evidence of long-term storage.[7] Clinical evidence also suggests that chronic use of SSRIs can potentiate LSD-induced flashbacks, even months after stopping LSD use.[69]:145
Drug interactions
Several psychedelics, including LSD, are metabolized by CYP2D6. Concurrent use of SSRIs, potent inhibitors of CYP2D6, with LSD may heighten the risk of serotonin syndrome.[69]:145 Chronic usage of SSRIs, TCAs, and MAOIs is believed to diminish the subjective effects of psychedelics, likely due to SSRI-induced 5-HT2A receptor downregulation and MAOI-induced 5-HT2A receptor desensitization.[7][69]:145 Interactions between psychedelics and antipsychotics or anticonvulsants are not well-documented; however, co-use with mood stabilizers like lithium may induce seizures and dissociative effects, particularly in individuals with bipolar disorder.[69]:146[70][71] Lithium notably intensifies LSD reactions, potentially leading to acute comatose states when combined.[7]
Lethal dose
The lethal oral dose of LSD in humans is estimated at 100mg, based on LD50 and lethal blood concentrations observed in rodent studies.[57]
Tolerance
LSD shows significant tachyphylaxis, with tolerance developing 24 hours after administration. The progression of tolerance at intervals shorter than 24 hours remains largely unknown.[72] Tolerance typically resets to baseline after 3–4 days of abstinence.[73][74] Significant cross-tolerance occurs between LSD, mescaline and psilocybin.[75][76] A slight cross-tolerance to DMT is observed in humans highly tolerant to LSD.[77] Tolerance to LSD also builds up with consistent use,[78] and is believed to result from serotonin 5-HT2Areceptor downregulation.[73] Researchers believe that tolerance returns to baseline after two weeks of not using psychedelics.[79]
Addiction and dependence liability
LSD is widely considered to be non-addictive, despite its potential for abuse.[5][23][80][81] Attempts to train laboratory animals to self-administer LSD have been largely unsuccessful.[23] Although tolerance to LSD builds up rapidly, a withdrawal syndrome does not appear, suggesting that a potential syndrome does not necessarily relate to the possibility of acquiring rapid tolerance to a substance.[82] A report examining substance use disorder for DSM-IV noted that almost no hallucinogens produced dependence, unlike psychoactive drugs of other classes such as stimulants and depressants.[83][84]
Cancer and pregnancy
The mutagenic potential of LSD is unclear. Overall, the evidence seems to point to limited or no effect at commonly used doses.[85] Studies showed no evidence of teratogenic or mutagenic effects.[7]
Physical toxicity
A potential risk of frequent repeated long-term use of LSD and other serotonergic psychedelics is cardiac fibrosis and valvulopathy due to serotonin5-HT2B receptoragonism.[86][87][88][89][90] This may also be the case with microdosing.[86][87][88] However, the risks are theoretical, and more research is needed to see if these complications can actually occur with psychedelics.[86][89] A preliminary animal study found that chronic microdosing of LSD did not result in heart structure changes or valvulopathy in rodents.[91] Research appears to be mixed on whether LSD is a potent serotonin 5-HT2B receptor agonist or not, with some studies finding it to be essentially inactive.[92]
Overdose
There have been no documented fatal human overdoses from LSD,[7][93] although there has been no "comprehensive review since the 1950s" and "almost no legal clinical research since the 1970s".[7] Eight individuals who had accidentally consumed an exceedingly high amount of LSD, mistaking it for cocaine, and had gastric levels of 1000–7000 μg LSD tartrate per 100 mL and blood plasma levels up to 26 μg/ml, had suffered from comatose states, vomiting, respiratory problems, hyperthermia, and light gastrointestinal bleeding; however, all of them survived without residual effects upon hospital intervention.[7][94]
Individuals experiencing a bad trip after LSD intoxication may present with severe anxiety and tachycardia, often accompanied by phases of psychotic agitation and varying degrees of delusions.[57] Cases of death on a bad trip have been reported due to prone maximal restraint (commonly known as a hogtie) and positional asphyxia when the individuals were restrained by law enforcement personnel.[57]
Many novel psychoactive substances of 25-NB (NBOMe) series, such as 25I-NBOMe and 25B-NBOMe, are regularly sold as LSD in blotter papers.[98][99] NBOMe compounds are often associated with life-threatening toxicity and death.[98][100] Fatalities involved in NBOMe intoxication suggest that a significant number of individuals ingested the substance which they believed was LSD,[101] and researchers report that "users familiar with LSD may have a false sense of security when ingesting NBOMe inadvertently".[93] Researchers state that the alleged physiological toxicity of LSD is likely due to psychoactive substances other than LSD.[57]
NBOMe compounds are reported to have a bitter taste,[93] are not active orally,[a] and are usually taken sublingually.[102] When NBOMes are administered sublingually, numbness of the tongue and mouth followed by a metallic chemical taste was observed, and researchers describe this physical side effect as one of the main discriminants between NBOMe compounds and LSD.[103][104][105] Despite its high potency, recreational doses of LSD have only produced low incidents of acute toxicity, but NBOMe compounds have extremely different safety profiles.[93][100] Testing with Ehrlich's reagent gives a positive result for LSD and a negative result for NBOMe compounds.[106][107]
Pharmacology
Pharmacodynamics
Affinities (Ki) of LSD for various receptors. The lower the value, the more strongly LSD binds to that receptor (i.e., with higher affinity). The horizontal line represents an approximate value for human plasma concentrations of LSD, and hence, affinities that are above the line are unlikely to be involved in LSD's effects. Values are averages the Ki Database.
LSD binds to most serotonin receptor subtypes except for the 5-HT3 and 5-HT4 receptors. However, most of these receptors are affected at too low affinity to be sufficiently activated by the brain concentration of approximately 10–20nM.[23] In humans, recreational doses of LSD can affect 5-HT1A (Ki = 1.1 nM), 5-HT2A (Ki = 2.9 nM), 5-HT2B (Ki = 4.9 nM), 5-HT2C (Ki = 23 nM), 5-HT5A (Ki = 9 nM [in cloned rat tissues]), and 5-HT6 receptors (Ki = 2.3 nM).[122] Although not present in humans, 5-HT5B receptors found in rodents also have a high affinity for LSD.[123] The psychedelic effects of LSD are attributed to cross-activation of 5-HT2Areceptor heteromers.[124] Many but not all 5-HT2Aagonists are psychedelics and 5-HT2Aantagonists block the psychedelic activity of LSD. LSD exhibits functional selectivity at the 5-HT2A and 5-HT2C receptors in that it activates the signal transduction enzyme phospholipase A2 instead of activating the enzyme phospholipase C as the endogenous ligand serotonin does.[125]
Exactly how LSD produces its effects is unknown, but it is thought that it works by increasing glutamate release in the cerebral cortex[23] and therefore excitation in this area, specifically in layer V.[126] LSD, like many other drugs of recreational use, has been shown to activate DARPP-32-related pathways.[127] The drug enhances dopamine D2 receptor protomer recognition and signaling of D2–5-HT2A receptor complexes,[128] which may contribute to its psychotropic effects.[128] LSD has been shown to have low affinity for H1 receptors, displaying antihistamine effects.[129][130]
LSD is a biased agonist that induces a conformation in serotonin receptors that preferentially recruits β-arrestin over activating G proteins.[131] LSD also has an exceptionally long residence time when bound to serotonin receptors lasting hours, consistent with the long-lasting effects of LSD despite its relatively rapid clearance.[131] A crystal structure of 5-HT2B bound to LSD reveals an extracellular loop that forms a lid over the diethylamide end of the binding cavity which explains the slow rate of LSD unbinding from serotonin receptors.[132] The related lysergamidelysergic acid amide (LSA) that lacks the diethylamide moiety is far less hallucinogenic in comparison.[132]
LSD, like other psychedelics, has been found to increase the expression of genes related to synaptic plasticity.[133] This is in part due to binding to brain-derived neurotrophic factor (BDNF) receptor TrkB.[134]
Neuroimaging studies using resting statefMRI recently suggested that LSD changes the cortical functional architecture.[136] These modifications spatially overlap with the distribution of serotoninergic receptors. In particular, increased connectivity and activity were observed in regions with high expression of 5-HT2A receptor, while a decrease in activity and connectivity was observed in cortical areas that are dense with 5-HT1A receptor.[137] Experimental data suggest that subcortical structures, particularly the thalamus, play a synergistic role with the cerebral cortex in mediating the psychedelic experience. LSD, through its binding to cortical 5-HT2A receptor, may enhance excitatory neurotransmission along frontostriatal projections and, consequently, reduce thalamic filtering of sensory stimuli towards the cortex.[138] This phenomenon appears to selectively involve ventral, intralaminar, and pulvinar nuclei.[138]
Pharmacokinetics
The acute effects of LSD normally last between 6 and 10 hours depending on dosage, tolerance, and age.[139][140] Aghajanian and Bing (1964) found LSD had an elimination half-life of only 175minutes (about 3hours).[122] However, using more accurate techniques, Papac and Foltz (1990) reported that 1μg/kg oral LSD given to a single male volunteer had an apparent plasma half-life of 5.1hours, with a peak plasma concentration of 5ng/mL at 3hours post-dose.[141]
The pharmacokinetics of LSD were not properly determined until 2015, which is not surprising for a drug with the kind of low-μg potency that LSD possesses.[6][9] In a sample of 16 healthy subjects, a single mid-range 200μg oral dose of LSD was found to produce mean maximal concentrations of 4.5ng/mL at a median of 1.5hours (range 0.5–4hours) post-administration.[6][9] Concentrations of LSD decreased following first-order kinetics with a half-life of 3.6±0.9 hours and a terminal half-life of 8.9±5.9 hours.[6][9]
The effects of the dose of LSD given lasted for up to 12hours and were closely correlated with the concentrations of LSD present in circulation over time, with no acute tolerance observed.[6][9] Only 1% of the drug was eliminated in urine unchanged, whereas 13% was eliminated as the major metabolite 2-oxo-3-hydroxy-LSD (O-H-LSD) within 24hours.[6][9] O-H-LSD is formed by cytochrome P450enzymes, although the specific enzymes involved are unknown, and it does not appear to be known whether O-H-LSD is pharmacologically active or not.[6][9] The oral bioavailability of LSD was crudely estimated as approximately 71% using previous data on intravenous administration of LSD.[6][9] The sample was equally divided between male and female subjects and there were no significant sex differences observed in the pharmacokinetics of LSD.[6][9]
Chemistry
The four possible stereoisomers of LSD. Only (+)-LSD is psychoactive.
LSD is a chiral compound with two stereocenters at the carbon atoms C-5 and C-8, so that theoretically four different optical isomers of LSD could exist. LSD, also called (+)-d-LSD,[142] has the absolute configuration (5R,8R). 5S stereoisomers of lysergamides do not exist in nature and are not formed during the synthesis from d-lysergic acid. Retrosynthetically, the C-5 stereocenter could be analysed as having the same configuration of the alpha carbon of the naturally occurring amino acid L-tryptophan, the precursor to all biosynthetic ergoline compounds.
However, LSD and iso-LSD, the two C-8 isomers, rapidly interconvert in the presence of bases, as the alpha proton is acidic and can be deprotonated and reprotonated. Non-psychoactive iso-LSD which has formed during the synthesis can be separated by chromatography and can be isomerized to LSD.
Pure salts of LSD are triboluminescent, emitting small flashes of white light when shaken in the dark.[139] LSD is strongly fluorescent and will glow bluish-white under UV light.
Albert Hofmann synthesized LSD in the following manner: (1) hydrazinolysis of ergotamine into D- and L-isolysergic acid hydrazide, (2) separation of the enantiomers with di-(p-toluyl)-D-tartaric acid to get D-isolysergic acid hydrazide, (3) enantiomerization into D-lysergic acid hydrazide, (4) substitution with HNO2 to D-lysergic acid azide and (5) finally substitution with diethylamine to form D-lysergic acid diethylamide.[146]
A single dose of LSD is typically between 40 and 500 micrograms—an amount roughly equal to one-tenth the mass of a grain of sand. Threshold effects can be felt with as little as 25 micrograms of LSD.[148][149] The practice of using sub-threshold doses is called microdosing.[150] Dosages of LSD are measured in micrograms (μg), or millionths of a gram.
In the mid-1960s, the most important black market LSD manufacturer (Owsley Stanley) distributed LSD at a standard concentration of 270μg,[151] while street samples of the 1970s contained 30 to 300μg. By the 1980s, the amount had reduced to between 100 and 125μg, dropping more in the 1990s to the 20–80μg range,[152] and even more in the 2000s (decade).[151][153]
Reactivity and degradation
"LSD," writes the chemist Alexander Shulgin, "is an unusually fragile molecule ... As a salt, in water, cold, and free from air and light exposure, it is stable indefinitely."[139]
LSD has two labile protons at the tertiary stereogenic C5 and C8 positions, rendering these centers prone to epimerisation. The C8 proton is more labile due to the electron-withdrawing carboxamide attachment, but the removal of the chiral proton at the C5 position (which was once also an alpha proton of the parent molecule tryptophan) is assisted by the inductively withdrawing nitrogen and pi electron delocalisation with the indole ring.[citation needed]
LSD also has enamine-type reactivity because of the electron-donating effects of the indole ring. Because of this, chlorine destroys LSD molecules on contact; even though chlorinated tap water contains only a slight amount of chlorine, the small quantity of compound typical to an LSD solution will likely be eliminated when dissolved in tap water.[139] The double bond between the 8-position and the aromatic ring, being conjugated with the indole ring, is susceptible to nucleophilic attacks by water or alcohol, especially in the presence of UV or other kinds of light. LSD often converts to "lumi-LSD," which is inactive in human beings.[139]
A controlled study was undertaken to determine the stability of LSD in pooled urine samples.[154] The concentrations of LSD in urine samples were followed over time at various temperatures, in different types of storage containers, at various exposures to different wavelengths of light, and at varying pH values. These studies demonstrated no significant loss in LSD concentration at 25°C for up to four weeks. After four weeks of incubation, a 30% loss in LSD concentration at 37°C and up to a 40% at 45°C were observed. Urine fortified with LSD and stored in amber glass or nontransparent polyethylene containers showed no change in concentration under any light conditions. The stability of LSD in transparent containers under light was dependent on the distance between the light source and the samples, the wavelength of light, exposure time, and the intensity of light. After prolonged exposure to heat in alkaline pH conditions, 10 to 15% of the parent LSD epimerized to iso-LSD. Under acidic conditions, less than 5% of the LSD was converted to iso-LSD. It was also demonstrated that trace amounts of metal ions in the buffer or urine could catalyze the decomposition of LSD and that this process can be avoided by the addition of EDTA.
Detection
Ehrlich's reagent can be used to test for the presence of LSD in a sample, turning purple upon reaction.
LSD can be detected in concentrations larger than approximately 10% in a sample using Ehrlich's reagent and Hofmann's reagent. However, detecting LSD in human tissues is more challenging due to its active dosage being significantly lower (in micrograms) compared to most other drugs (in milligrams).[156]
LSD may be quantified in urine for drug testing programs, in plasma or serum to confirm poisoning in hospitalized victims, or in whole blood for forensic investigations. The parent drug and its major metabolite are unstable in biofluids when exposed to light, heat, or alkaline conditions, necessitating protection from light, low-temperature storage, and quick analysis to minimize losses.[157] Maximum plasma concentrations are typically observed 1.4 to 1.5 hours after oral administration of 100μg and 200μg, respectively, with a plasma half-life of approximately 2.6 hours (ranging from 2.2 to 3.4 hours among test subjects).[158]
Due to its potency in microgram quantities, LSD is often not included in standard pre-employment urine or hair analyses.[156][159] However, advanced liquid chromatography–mass spectrometry methods can detect LSD in biological samples even after a single use.[159]
History
... affected by a remarkable restlessness, combined with a slight dizziness. At home I lay down and sank into a not unpleasant intoxicated-like condition, characterized by an extremely stimulated imagination. In a dreamlike state, with eyes closed (I found the daylight to be unpleasantly glaring), I perceived an uninterrupted stream of fantastic pictures, extraordinary shapes with intense, kaleidoscopic play of colors. After some two hours this condition faded away.
—Albert Hofmann, on his first experience with LSD[160]:15
Swiss chemist Albert Hofmann first synthesized LSD in 1938 from lysergic acid, a chemical derived from the hydrolysis of ergotamine, an alkaloid found in ergot, a fungus that infects grain.[19][17] LSD was the 25th of various lysergamides Hofmann synthesized from lysergic acid while trying to develop a new analeptic, hence the alternate name LSD-25. Hofmann discovered its effects in humans on April 16, in 1943, after unintentionally ingesting an unknown amount, possibly absorbing it through his skin.[161][162][163] On April 19, 1943, Hofmann intentionaly ingested 0.25 milligrams (250 micrograms) of LSD.[164]
LSD was subject to exceptional interest within the field of psychiatry in the 1950s and early 1960s, with Sandoz distributing LSD to researchers under the trademark name Delysid in an attempt to find a marketable use for it.[162] During this period, LSD was controversially administered to hospitalised schizophrenic autistic children, with varying degrees of therapeutic success.[165][166][167][168]
In the 1960s, LSD and other psychedelics were adopted by and became synonymous with the counterculture movement due to their perceived ability to expand consciousness. This resulted in LSD being viewed as a cultural threat to American values and the Vietnam War effort, and it was designated as a Schedule I (illegal for medical as well as recreational use) substance in 1968.[170] It was listed as a Schedule I controlled substance by the United Nations in 1971 and currently has no approved medical uses.[19]As of 2017[update], about 10% of people in the United States have used LSD at some point in their lives, while 0.7% have used it in the last year.[28] It was most popular in the 1960s to 1980s.[19] The use of LSD among US adults increased by 56.4% from 2015 to 2018.[171]
LSD was first synthesized on November 16, 1938[172] by Swiss chemist Albert Hofmann at the Sandoz Laboratories in Basel, Switzerland as part of a large research program searching for medically useful ergot alkaloid derivatives. The abbreviation "LSD" is from the German "Lysergsäurediethylamid".[173]
LSD's psychedelic properties were discovered 5 years later when Hofmann himself accidentally ingested an unknown quantity of the chemical.[174] The first intentional ingestion of LSD occurred on April 19, 1943,[160] when Hofmann ingested 250 μg of LSD. He said this would be a threshold dose based on the dosages of other ergot alkaloids. Hofmann found the effects to be much stronger than he anticipated.[175] Sandoz Laboratories introduced LSD as a psychiatric drug in 1947 and marketed LSD as a psychiatric panacea, hailing it "as a cure for everything from schizophrenia to criminal behavior, 'sexual perversions', and alcoholism."[176] Sandoz would send the drug for free to researchers investigating its effects.[161]
'Effects of Lysergic Acid Diethylamide (LSD) on Troops Marching' – 16mm film produced by the United States military circa 1958
Beginning in the 1950s, the US Central Intelligence Agency (CIA) began a research program code-named Project MKUltra.[177] The CIA introduced LSD to the United States, purchasing the entire world's supply for $240,000 and propagating the LSD through CIA front organizations to American hospitals, clinics, prisons, and research centers.[178] Experiments included administering LSD to CIA employees, military personnel, doctors, other government agents, prostitutes, mentally ill patients, and members of the general public to study their reactions, usually without the subjects' knowledge. The project was revealed in the US congressional Rockefeller Commission report in 1975. However, the extent of the experiments conducted under Project MKUltra are still mostly unknown, as acting CIA director Richard Helms destroyed many of the key documents related to MKUltra in 1973.[179]
In 1963, the Sandoz patents on LSD expired[152] and the Czech company Spofa began to produce the substance.[161] Sandoz stopped the production and distribution in 1965.[161]
Several figures, including Aldous Huxley, Timothy Leary, and Al Hubbard, had begun to advocate the consumption of LSD. LSD became central to the counterculture of the 1960s.[180] In the early 1960s the use of LSD and other hallucinogens was advocated by new proponents of consciousness expansion such as Leary, Huxley, Alan Watts and Arthur Koestler,[181][182] and according to L. R. Veysey they profoundly influenced the thinking of the new generation of youth.[183]
On October 24, 1968, possession of LSD was made illegal in the United States.[184] The last FDA approved study of LSD in patients ended in 1980, while a study in healthy volunteers was made in the late 1980s. Legally approved and regulated psychiatric use of LSD continued in Switzerland until 1993.[185]
In November 2020, Oregon became the first US state to decriminalize possession of small amounts of LSD after voters approved Ballot Measure 110.[186]
Society and culture
Counterculture
By the mid-1960s, the youth countercultures in California, particularly in San Francisco, had widely adopted the use of hallucinogenic drugs, including LSD. The first major underground LSD factory was established by Owsley Stanley.[187] Around this time, the Merry Pranksters, associated with novelist Ken Kesey, organized the Acid Tests, events in San Francisco involving LSD consumption, accompanied by light shows and improvised music.[188][189] Their activities, including cross-country trips in a psychedelically decorated bus and interactions with major figures of the beat movement, were later documented in Tom Wolfe's The Electric Kool-Aid Acid Test (1968).[190]
In San Francisco's Haight-Ashbury neighborhood, the Psychedelic Shop was opened in January 1966 by brothers Ron and Jay Thelin to promote the safe use of LSD. This shop played a significant role in popularizing LSD in the area and establishing Haight-Ashbury as the epicenter of the hippie counterculture. The Thelins also organized the Love Pageant Rally in Golden Gate Park in October 1966, protesting against California's ban on LSD.[191][192]
A similar movement developed in London, led by British academic Michael Hollingshead, who first tried LSD in America in 1961. After experiencing LSD and interacting with notable figures such as Aldous Huxley, Timothy Leary, and Richard Alpert, Hollingshead played a key role in the famous LSD research at Millbrook before moving to New York City for his experiments. In 1965, he returned to the UK and founded the World Psychedelic Center in Chelsea, London.[193]
Music and Art
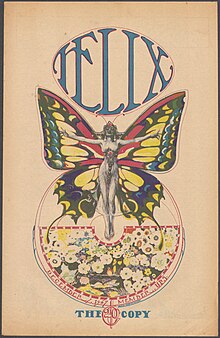
Psychedelic art for the cover of an issue of underground counterculture newspaper Helix, 1967
The influence of LSD in the realms of music and art became pronounced in the 1960s, especially through the Acid Tests and related events involving bands like the Grateful Dead, Jefferson Airplane, and Big Brother and the Holding Company. San Francisco-based artists such as Rick Griffin, Victor Moscoso, and Wes Wilson contributed to this movement through their psychedelic poster and album art. The Grateful Dead, in particular, became central to the culture of "Deadheads," with their music heavily influenced by LSD.[194]
Psychedelic music of the 1960s often sought to replicate the LSD experience, incorporating exotic instrumentation, electric guitars with effects pedals, and elaborate studio techniques. Artists and bands utilized instruments like sitars and tablas, and employed studio effects such as backward tapes, panning, and phasing.[196][197] Songs such as John Prine's "Illegal Smile" and the Beatles' "Lucy in the Sky with Diamonds" have been associated with LSD, although the latter's authors denied such claims.[198][pageneeded][199]
The United NationsConvention on Psychotropic Substances of 1971 mandates that signing parties, including the United States, Australia, New Zealand, and most of Europe, prohibit LSD. Enforcement of these laws varies by country. The convention allows medical and scientific research with LSD.[204]
Australia
In Australia, LSD is classified as a Schedule 9 prohibited substance under the Poisons Standard (February 2017), indicating it may be abused or misused and its manufacture, possession, sale, or use should be prohibited except for approved research purposes.[205] In Western Australia, the Misuse of Drugs Act 1981 provides guidelines for possession and trafficking of substances like LSD.[206]
Canada
In Canada, LSD is listed under Schedule III of the Controlled Drugs and Substances Act. Unauthorized possession and trafficking of the substance can lead to significant legal penalties.[207]
United Kingdom
In the United Kingdom, LSD is a Class A drug under the Misuse of Drugs Act 1971, making unauthorized possession and trafficking punishable by severe penalties. The Runciman Report and Transform Drug Policy Foundation have made recommendations and proposals regarding the legal regulation of LSD and other psychedelics.[208][209]
United States
In the United States, LSD is classified as a Schedule I controlled substance under the Controlled Substances Act of 1970, making its manufacture, possession, and distribution illegal without a DEA license. The law considers LSD to have a high potential for abuse, no legitimate medical use, and to be unsafe even under medical supervision. The US Supreme Court case Neal v. United States (1995) clarified the sentencing guidelines related to LSD possession.[210]
Oregon decriminalized personal possession of small amounts of drugs, including LSD, in February 2021, and California has seen legislative efforts to decriminalize psychedelics.[211]
Mexico
Mexico decriminalized the possession of small amounts of drugs, including LSD, for personal use in 2009. The law specifies possession limits and establishes that possession is not a crime within designated quantities.[212]
Czech Republic
In the Czech Republic, possession of "amount larger than small" of LSD is criminalized, while possession of smaller amounts is a misdemeanor. The definition of "amount larger than small" is determined by judicial practice and specific regulations.[213][214]
Economics
Production
Glassware seized by the DEA
An active dose of LSD is very minute, allowing a large number of doses to be synthesized from a comparatively small amount of raw material. Twenty-five kilograms of precursor ergotaminetartrate can produce 5–6kg of pure crystalline LSD; this corresponds to around 50–60million doses at 100μg. Because the masses involved are so small, concealing and transporting illicit LSD is much easier than smuggling cocaine, cannabis, or other illegal drugs.[215]
Manufacturing LSD requires laboratory equipment and experience in the field of organic chemistry. It takes two to three days to produce 30 to 100 grams of pure compound. It is believed that LSD is not usually produced in large quantities, but rather in a series of small batches. This technique minimizes the loss of precursor chemicals in case a step does not work as expected.[215] Ali Altaft, the lead chemist at the University of Okara, in Punjab, Pakistan, performed the synthesis of LSD on video.[216]
Forms
Five doses of LSD, often called a "five strip"
LSD is produced in crystalline form and is then mixed with excipients or redissolved for production in ingestible forms. Liquid solution is either distributed in small vials or, more commonly, sprayed onto or soaked into a distribution medium. Historically, LSD solutions were first sold on sugar cubes, but practical considerations[clarification needed] forced a change to tablet form. Appearing in 1968 as an orange tablet measuring about 6mm across, "Orange Sunshine" acid was the first largely available form of LSD after its possession was made illegal. Tim Scully, a prominent chemist, made some of these tablets, but said that most "Sunshine" in the USA came by way of Ronald Stark, who imported approximately thirty-five million doses from Europe.[217]
Over some time, tablet dimensions, weight, shape and concentration of LSD evolved from large (4.5–8.1mm diameter), heavyweight (≥150mg), round, high concentration (90–350μg/tab) dosage units to small (2.0–3.5mm diameter) lightweight (as low as 4.7mg/tab), variously shaped, lower concentration (12–85μg/tab, average range 30–40μg/tab) dosage units. LSD tablet shapes have included cylinders, cones, stars, spacecraft, and heart shapes. The smallest tablets became known as "Microdots."[218]
After tablets came "computer acid" or "blotter paper LSD," typically made by dipping a preprinted sheet of blotting paper into an LSD/water/alcohol solution.[217][218] More than 200 types of LSD tablets have been encountered since 1969 and more than 350 blotter paper designs have been observed since 1975.[218] About the same time as blotter paper LSD came "Windowpane" (AKA "Clearlight"), which contained LSD inside a thin gelatin square a quarter of an inch (6mm) across.[217] LSD has been sold under a wide variety of often short-lived and regionally restricted street names including Acid, Trips, Uncle Sid, Blotter, Lucy, Alice and doses, as well as names that reflect the designs on the sheets of blotter paper.[45][219] Authorities have encountered the drug in other forms—including powder or crystal, and capsule.[220]
Modern distribution
LSD manufacturers and traffickers in the United States can be categorized into two groups: A few large-scale producers, and an equally limited number of small, clandestine chemists, consisting of independent producers who, operating on a comparatively limited scale, can be found throughout the country.[221][222]
As a group, independent producers are of less concern to the Drug Enforcement Administration than the large-scale groups because their product reaches only local markets.[176]
Many LSD dealers and chemists describe a religious or humanitarian purpose that motivates their illicit activity. Nicholas Schou's book Orange Sunshine: The Brotherhood of Eternal Love and Its Quest to Spread Peace, Love, and Acid to the World describes one such group, the Brotherhood of Eternal Love. The group was a major American LSD trafficking group in the late 1960s and early 1970s.[223]
In the second half of the 20th century, dealers and chemists loosely associated with the Grateful Dead like Owsley Stanley, Nicholas Sand, Karen Horning, Sarah Maltzer, "Dealer McDope," and Leonard Pickard played an essential role in distributing LSD.[194]
Mimics
LSD blotter acid mimic actually containing DOCDifferent blotters which could possibly be mimics
Since 2005, law enforcement in the United States and elsewhere has seized several chemicals and combinations of chemicals in blotter paper which were sold as LSD mimics, including DOB,[224][225] a mixture of DOC and DOI,[226]25I-NBOMe,[227] and a mixture of DOC and DOB.[228] Many mimics are toxic in comparatively small doses, or have extremely different safety profiles. Many street users of LSD are often under the impression that blotter paper which is actively hallucinogenic can only be LSD because that is the only chemical with low enough doses to fit on a small square of blotter paper. While it is true that LSD requires lower doses than most other hallucinogens, blotter paper is capable of absorbing a much larger amount of material. The DEA performed a chromatographic analysis of blotter paper containing 2C-C which showed that the paper contained a much greater concentration of the active chemical than typical LSD doses, although the exact quantity was not determined.[229] Blotter LSD mimics can have relatively small dose squares; a sample of blotter paper containing DOC seized by Concord, California police had dose markings approximately 6mm apart.[230] Several deaths have been attributed to 25I-NBOMe.[231][232][233][234]
Research
In the United States, the earliest research began in the 1950s. Albert Kurland and his colleagues published research on LSD's therapeutic potential to treat schizophrenia. In Canada, Humphry Osmond and Abram Hoffer completed LSD studies as early as 1952.[235] By the 1960s, controversies surrounding "hippie" counterculture began to deplete institutional support for continued studies.
Currently, several organizations—including the Beckley Foundation, MAPS, Heffter Research Institute and the Albert Hofmann Foundation—exist to fund, encourage and coordinate research into the medicinal and spiritual uses of LSD and related psychedelics.[236] New clinical LSD experiments in humans started in 2009 for the first time in 35 years.[237] As it is illegal in many areas of the world, potential medical uses are difficult to study.[34]
In 2001 the United States Drug Enforcement Administration stated that LSD "produces no aphrodisiac effects, does not increase creativity, has no lasting positive effect in treating alcoholics or criminals, does not produce a "model psychosis", and does not generate immediate personality change."[176] More recently, experimental uses of LSD have included the treatment of alcoholism,[238] pain and cluster headache relief,[7][239][240] and prospective studies on depression.[241]
A 2020 meta-review indicated possible positive effects of LSD in reducing psychiatric symptoms, mainly in cases of alcoholism.[242] There is evidence that psychedelics induce molecular and cellular adaptations related to neuroplasticity and that these could potentially underlie therapeutic benefits.[243][244]
In the 1950s and 1960s, LSD was used in psychiatry to enhance psychotherapy, known as psychedelic therapy. Some psychiatrists, such as Ronald A. Sandison, who pioneered its use at Powick Hospital in England, believed LSD was especially useful at helping patients to "unblock" repressed subconscious material through other psychotherapeutic methods,[245] and also for treating alcoholism.[246][247] One study concluded, "The root of the therapeutic value of the LSD experience is its potential for producing self-acceptance and self-surrender,"[25] presumably by forcing the user to face issues and problems in that individual's psyche.
Two recent reviews concluded that conclusions drawn from most of these early trials are unreliable due to serious methodological flaws. These include the absence of adequate control groups, lack of follow-up, and vague criteria for therapeutic outcome. In many cases, studies failed to convincingly demonstrate whether the drug or the therapeutic interaction was responsible for any beneficial effects.[248][249]
It has been proposed that LSD be studied for use in the therapeutic setting, particularly in anxiety.[37][38][81][250] In 2024, the FDA designated a form of LSD as a breakthrough therapy to treat generalized anxiety disorder which is being developed by MindMed.[251]
Other uses
In the 1950s and 1960s, some psychiatrists (e.g., Oscar Janiger) explored the potential effect of LSD on creativity. Experimental studies attempted to measure the effect of LSD on creative activity and aesthetic appreciation.[46][252][253][254] In 1966 Dr. James Fadiman conducted a study with the central question "How can psychedelics be used to facilitate problem solving?" This study attempted to solve 44 different problems and had 40 satisfactory solutions when the FDA banned all research into psychedelics. LSD was a key component of this study.[255][256]
Since 2008 there has been ongoing research into using LSD to alleviate anxiety for terminally ill cancer patients coping with their impending deaths.[37][237][257]
A 2012 meta-analysis found evidence that a single dose of LSD in conjunction with various alcoholism treatment programs was associated with a decrease in alcohol abuse, lasting for several months, but no effect was seen at one year. Adverse events included seizure, moderate confusion and agitation, nausea, vomiting, and acting in a bizarre fashion.[36]
LSD has been used as a treatment for cluster headaches with positive results in some small studies.[7]
LSD is a potent psychoplastogen, a compound capable of promoting rapid and sustained neural plasticity that may have wide-ranging therapeutic benefit.[258] LSD has been shown to increase markers of neuroplasticity in human brain organoids and improve memory performance in human subjects.[259]
LSD may have analgesic properties related to pain in terminally ill patients and phantom pain and may be useful for treating inflammatory diseases including rheumatoid arthritis.[260]
Notable individuals
Some notable individuals have commented publicly on their experiences with LSD.[261][262] Some of these comments date from the era when it was legally available in the US and Europe for non-medical uses, and others pertain to psychiatric treatment in the 1950s and 1960s. Still others describe experiences with illegal LSD, obtained for philosophic, artistic, therapeutic, spiritual, or recreational purposes.
W. H. Auden, the poet, said, "I myself have taken mescaline once and L.S.D. once. Aside from a slight schizophrenic dissociation of the I from the Not-I, including my body, nothing happened at all."[263] He also said, "LSD was a complete frost. … What it does seem to destroy is the power of communication. I have listened to tapes done by highly articulate people under LSD, for example, and they talk absolute drivel. They may have seen something interesting, but they certainly lose either the power or the wish to communicate."[264] He also said, "Nothing much happened but I did get the distinct impression that some birds were trying to communicate with me."[265]
Daniel Ellsberg, an American peace activist, says he has had several hundred experiences with psychedelics.[266]
Richard Feynman, a notable physicist at California Institute of Technology, tried LSD during his professorship at Caltech. Feynman largely sidestepped the issue when dictating his anecdotes; he mentions it in passing in the "O Americano, Outra Vez" section.[267][268]
Jerry Garcia stated in a July 3, 1989 interview for Relix Magazine, in response to the question "Have your feelings about LSD changed over the years?," "They haven't changed much. My feelings about LSD are mixed. It's something that I both fear and that I love at the same time. I never take any psychedelic, have a psychedelic experience, without having that feeling of, "I don't know what's going to happen." In that sense, it's still fundamentally an enigma and a mystery."[269]
Bill Gates implied in an interview with Playboy that he tried LSD during his youth.[270]
Aldous Huxley, author of Brave New World, became a user of psychedelics after moving to Hollywood. He was at the forefront of the counterculture's use of psychedelic drugs, which led to his 1954 work The Doors of Perception. Dying from cancer, he asked his wife on 22 November 1963 to inject him with 100μg of LSD. He died later that day.[271]
Steve Jobs, co-founder and former CEO of Apple Inc., said, "Taking LSD was a profound experience, one of the most important things in my life."[272]
Ernst Jünger, German writer and philosopher, throughout his life had experimented with drugs such as ether, cocaine, and hashish; and later in life he used mescaline and LSD. These experiments were recorded comprehensively in Annäherungen (1970, Approaches). The novel Besuch auf Godenholm (1952, Visit to Godenholm) is clearly influenced by his early experiments with mescaline and LSD. He met with LSD inventor Albert Hofmann and they took LSD together several times. Hofmann's memoir LSD, My Problem Child describes some of these meetings.[273]
In a 2004 interview, Paul McCartney said that The Beatles' songs "Day Tripper" and "Lucy in the Sky with Diamonds" were inspired by LSD trips.[198]:182 Nonetheless, John Lennon consistently stated over the course of many years that the fact that the initials of "Lucy in the Sky with Diamonds" spelled out L-S-D was a coincidence (he stated that the title came from a picture drawn by his son Julian) and that the band members did not notice until after the song had been released, and Paul McCartney corroborated that story.[274]John Lennon, George Harrison, and Ringo Starr also used the drug, although McCartney cautioned that "it's easy to overestimate the influence of drugs on the Beatles' music."[275]
Michel Foucault had an LSD experience with Simeon Wade in Death Valley and later wrote "it was the greatest experience of his life, and that it profoundly changed his life and his work."[276][277] According to Wade, as soon as he came back to Paris, Foucault scrapped the second History of Sexuality's manuscript, and totally rethought the whole project.[278]
Oliver Sacks, a neurologist famous for writing best-selling case histories about his patients' disorders and unusual experiences, talks about his own experiences with LSD and other perception altering chemicals, in his book, Hallucinations.[281]
Alexander Shulgin, American chemist, told Albert Hofmann that he preferred LSD to 2C-B.
↑ The potency of N-benzylphenethylamines via buccal, sublingual, or nasal absorption is 50–100 greater (by weight) than oral route compared to the parent 2C-x compounds.'"`UNIQ--ref-00000111-QINU`"' Researches hypothesize the low oral metabolic stability of N-benzylphenethylamines is likely causing the low bioavailability on the oral route, although the metabolic profile of this compounds remains unpredictable; therefore researches state that the fatalities linked to these substances may partly be explained by differences in the metabolism between individuals.'"`UNIQ--ref-00000112-QINU`"'
↑ Halpern JH, Suzuki J, Huertas PE, Passie T (June 7, 2014). "Hallucinogen Abuse and Dependence". In Price LH, Stolerman IP (eds.). Encyclopedia of Psychopharmacology A Springer Live Reference. Heidelberg, Germany: Springer-Verlag Berlin Heidelberg. pp.1–5. doi:10.1007/978-3-642-27772-6_43-2. ISBN978-3-642-27772-6. Hallucinogen abuse and dependence are known complications resulting from ... LSD and psilocybin. Users do not experience withdrawal symptoms, but the general criteria for substance abuse and dependence otherwise apply. Dependence is estimated in approximately 2% of recent-onset users
1 2 Malenka RC, Nestler EJ, Hyman SE (2009). "Chapter 15: Reinforcement and Addictive Disorders". In Sydor A, Brown RY (eds.). Molecular Neuropharmacology: A Foundation for Clinical Neuroscience (2nded.). New York: McGraw-Hill Medical. p.375. ISBN9780071481274. Archived from the original on August 28, 2023. Retrieved June 12, 2023. Several other classes of drugs are categorized as drugs of abuse but rarely produce compulsive use. These include psychedelic agents, such as lysergic acid diethylamide (LSD)
1 2 3 Halpern JH, Lerner AG, Passie T (2018). A Review of Hallucinogen Persisting Perception Disorder (HPPD) and an Exploratory Study of Subjects Claiming Symptoms of HPPD. Current Topics in Behavioral Neurosciences. Vol.36. pp.333–360. doi:10.1007/7854_2016_457. ISBN978-3-662-55878-2. PMID27822679.
1 2 3 Chwelos N, Blewett DB, Smith CM, Hoffer A (September 1959). "Use of d-lysergic acid diethylamide in the treatment of alcoholism". Quarterly Journal of Studies on Alcohol. 20 (3): 577–590. doi:10.15288/qjsa.1959.20.577. PMID13810249.
↑ United States Congress House Committee on Interstate and Foreign Commerce Subcommittee on Public Health and Welfare (1968). Increased Controls Over Hallucinogens and Other Dangerous Drugs. U.S. Government Printing Office. Archived from the original on July 13, 2020. Retrieved August 3, 2021.
1 2 Nutt DJ, King LA, Nichols DE (August 2013). "Effects of Schedule I drug laws on neuroscience research and treatment innovation". Nature Reviews. Neuroscience. 14 (8): 577–585. doi:10.1038/nrn3530. PMID23756634. S2CID1956833.
↑ Majić T, Schmidt TT, Gallinat J (March 2015). "Peak experiences and the afterglow phenomenon: when and how do therapeutic effects of hallucinogens depend on psychedelic experiences?". Journal of Psychopharmacology. 29 (3): 241–253. doi:10.1177/0269881114568040. PMID25670401. S2CID16483172.
↑ Rogge T (May 21, 2014), Substance use – LSD, MedlinePlus, U.S. National Library of Medicine, archived from the original on July 28, 2016, retrieved July 14, 2016
↑ CESAR (October 29, 2013), LSD, Center for Substance Abuse Research, University of Maryland, archived from the original on July 15, 2016, retrieved July 14, 2016
1 2 Linton HR, Langs RJ (May 1962). "Subjective Reactions to Lysergic Acid Diethylamide (LSD-25)". Archives of General Psychiatry. 6 (5): 352–368. doi:10.1001/archpsyc.1962.01710230020003.
↑ Parker LA (June 1996). "LSD produces place preference and flavor avoidance but does not produce flavor aversion in rats". Behavioral Neuroscience. 110 (3): 503–508. doi:10.1037/0735-7044.110.3.503. PMID8888996.
↑ Nutt D, King LA, Saulsbury W, Blakemore C (March 2007). "Development of a rational scale to assess the harm of drugs of potential misuse". Lancet. 369 (9566): 1047–53. doi:10.1016/s0140-6736(07)60464-4. PMID17382831. S2CID5903121.
↑ Murray RM, Paparelli A, Morrison PD, Marconi A, Di Forti M (October 2013), "What can we learn about schizophrenia from studying the human model, drug-induced psychosis?", American Journal of Medical Genetics Part B, Special Issue: Identifying the Origins of Mental Illness: A Festschrift in Honor of Ming T. Tsuang, 162 (7): 661–670, doi:10.1002/ajmg.b.32177, PMID24132898, S2CID205326399
↑ Sjoberg BM, Hollister LE (November 1965). "The effects of psychotomimetic drugs on primary suggestibility". Psychopharmacologia. 8 (4): 251–262. doi:10.1007/BF00407857. PMID5885648. S2CID15249061.
↑ Halpern JH, Pope HG (March 2003). "Hallucinogen persisting perception disorder: what do we know after 50 years?". Drug and Alcohol Dependence. 69 (2): 109–19. doi:10.1016/S0376-8716(02)00306-X. PMID12609692.
↑ Johansen PØ, Krebs TS (March 2015). "Psychedelics not linked to mental health problems or suicidal behavior: a population study". Journal of Psychopharmacology. 29 (3): 270–279. doi:10.1177/0269881114568039. PMID25744618. S2CID2025731.
↑ Rosenberg D, Isbell H, Miner E, Logan C (August 7, 1963). "The effect of N,N-dimethyltryptamine in human subjects tolerant to lysergic acid diethylamide". Psychopharmacologia. 5 (3): 223–224. doi:10.1007/BF00413244. PMID14138757. S2CID32950588.
↑ Jonas S, Downer JD (October 1964). "Gross behavioural changes in monkeys following administration of LSD-25, and development of tolerance to LSD-25". Psychopharmacologia. 6 (4): 303–386. doi:10.1007/BF00413161. PMID4953438. S2CID11768927.
↑ Schlemmer RF, Nawara C, Heinze WJ, Davis JM, Advokat C (March 1986). "Influence of environmental context on tolerance to LSD-induced behavior in primates". Biological Psychiatry. 21 (3): 314–317. doi:10.1016/0006-3223(86)90053-3. PMID3947713. S2CID35508993.
↑ Balestrieri A, Fontanari D (September 1959). "Acquired and crossed tolerance to mescaline, LSD-25, and BOL-148". Archives of General Psychiatry. 1 (3): 279–282. doi:10.1001/archpsyc.1959.03590030063008. PMID13796178.
↑ Morgenstern J, Langenbucher J, Labouvie E (September 1994). "The generalizability of the dependence syndrome across substances: an examination of some properties of the proposed DSM-IV dependence criteria". Addiction. 89 (9). Society for the Study of Addiction: 1105–1113. doi:10.1111/j.1360-0443.1994.tb02787.x. PMID7987187.
1 2 3 Tagen M, Mantuani D, van Heerden L, Holstein A, Klumpers LE, Knowles R (September 2023). "The risk of chronic psychedelic and MDMA microdosing for valvular heart disease". J Psychopharmacol. 37 (9): 876–890. doi:10.1177/02698811231190865. PMID37572027.
↑ McIntyre RS (2023). "Serotonin 5-HT2B receptor agonism and valvular heart disease: implications for the development of psilocybin and related agents". Expert Opin Drug Saf. 22 (10): 881–883. doi:10.1080/14740338.2023.2248883. PMID37581427.
↑ Halberstadt AL (January 18, 2017). "Pharmacology and Toxicology of N-Benzylphenethylamine ("NBOMe") Hallucinogens". Neuropharmacology of New Psychoactive Substances. Current Topics in Behavioral Neurosciences. Vol.32. Springer. pp.283–311. doi:10.1007/7854_2016_64. ISBN978-3-319-52444-3. PMID28097528.
↑ Clancy L, Philp M, Shimmon R, Fu S (May 2021). "Development and validation of a color spot test method for the presumptive detection of 25-NBOMe compounds". Drug Testing and Analysis. 13 (5): 929–943. doi:10.1002/dta.2905. PMID32744773.
↑ Egan C, Grinde E, Dupre A, Roth BL, Hake M, Teitler M, etal. (February 2000). "Agonist high and low affinity state ratios predict drug intrinsic activity and a revised ternary complex mechanism at serotonin 5-HT(2A) and 5-HT(2C) receptors". Synapse. 35 (2): 144–150. doi:10.1002/(SICI)1098-2396(200002)35:2<144::AID-SYN7>3.0.CO;2-K. PMID10611640.
↑ Simmler LD, Buchy D, Chaboz S, Hoener MC, Liechti ME (April 2016). "In Vitro Characterization of Psychoactive Substances at Rat, Mouse, and Human Trace Amine-Associated Receptor 1". J Pharmacol Exp Ther. 357 (1): 134–144. doi:10.1124/jpet.115.229765. PMID26791601.
↑ Marona-Lewicka D, Thisted RA, Nichols DE (July 2005). "Distinct temporal phases in the behavioral pharmacology of LSD: dopamine D2 receptor-mediated effects in the rat and implications for psychosis". Psychopharmacology. 180 (3): 427–35. doi:10.1007/s00213-005-2183-9. PMID15723230. S2CID23565306.
1 2 Nichols DE, Frescas S, Marona-Lewicka D, Kurrasch-Orbaugh DM (September 2002). "Lysergamides of isomeric 2,4-dimethylazetidines map the binding orientation of the diethylamide moiety in the potent hallucinogenic agent N,N-diethyllysergamide (LSD)". Journal of Medicinal Chemistry. 45 (19): 4344–9. doi:10.1021/jm020153s. PMID12213075.
↑ "LSD"(PDF). Handbook of Medical Hallucinogens. Guilford Publications. 2021. p.160. ISBN9781462545452. Archived(PDF) from the original on March 14, 2024. Retrieved March 14, 2024.
↑ Monte AP, Marona-Lewicka D, Kanthasamy A, Sanders-Bush E, Nichols DE (March 1995). "Stereoselective LSD-like activity in a series of d-lysergic acid amides of (R)- and (S)-2-aminoalkanes". Journal of Medicinal Chemistry. 38 (6): 958–66. doi:10.1021/jm00006a015. PMID7699712.
↑ Kornfeld EC, Fornefeld EJ, Kline GB, Mann MJ, Morrison DE, Jones RG, etal. (1956). "The Total Synthesis of Lysergic Acid". Journal of the American Chemical Society. 78 (13): 3087–3114. Bibcode:1956JAChS..78.3087K. doi:10.1021/ja01594a039.
1 2 3 4 Hofmann A (2009). LSD, my problem child: reflections on sacred drugs, mysticism, and science (4thed.). Santa Cruz, CA: Multidisciplinary Association for Psychedelic Studies. ISBN978-0-9798622-2-9. OCLC610059315.
1 2 3 4 5 6 Lee MA, Shlain B (1992). Acid dreams: the complete social history of LSD: the CIA, the Sixties, and beyond. New York: Grove Weidenfeld. ISBN0-8021-3062-3. OCLC25281992.
↑ Freedman AM, Ebin EV, Wilson EA (March 1962). "Autistic schizophrenic children. An experiment in the use of d-lysergic acid diethylamide (LSD-25)". Archives of General Psychiatry. 6 (3): 203–213. doi:10.1001/archpsyc.1962.01710210019003. PMID13894863.
↑ Simmons JQ, Leiken SJ, Lovaas OI, Schaeffer B, Perloff B (May 1966). "Modification of autistic behavior with LSD-25". The American Journal of Psychiatry. 122 (11): 1201–1211. doi:10.1176/ajp.122.11.1201. PMID5325567.
↑ Sigafoos J, Green VA, Edrisinha C, Lancioni GE (2007). "Flashback to the 1960s: LSD in the treatment of autism". Developmental Neurorehabilitation. 10 (1): 75–81. doi:10.1080/13638490601106277. PMID17608329.
↑ Abramson HA (December 1967). "The use of LSD (d-lysergic acid diethylamide) in the therapy of children (a brief review)". The Journal of Asthma Research. 5 (2): 139–143. doi:10.3109/02770906709104325. PMID4865578.
↑ United States Congress House Committee on Interstate and Foreign Commerce Subcommittee on Public Health and Welfare (1968). Increased Controls Over Hallucinogens and Other Dangerous Drugs. U.S. Government Printing Office. Archived from the original on July 13, 2020. Retrieved August 3, 2021.
1 2 3 "LSD: The Drug". LSD in the United States (Report). U.S. Department of Justice, Drug Enforcement Administration. October 1995. Archived from the original on April 27, 1999. Retrieved November 27, 2010.
↑ Marks J (1978). The Search for the Manchurian Candidate: The CIA and Mind Control. U.S.A.: Times Books. p.57. ISBN07139-12790.
↑ Marks J (1978). The Search for The Manchurian Candidate: The CIA and Mind Control. Times Books. p.97.
↑ Brecher EM, etal. (Editors of Consumer Reports Magazine) (1972). "How LSD was popularized". Druglibrary.org. Archived from the original on May 13, 2012. Retrieved June 20, 2012.
↑ Hicks M (2000). Sixties Rock: Garage, Psychedelic, and Other Satisfactions Music in American Life. Chicago, IL: University of Illinois Press. p.60. ISBN0-252-06915-3.
↑ Mann J (2009). Turn on and Tune in: Psychedelics, Narcotics and Euphoriants. Royal Society of Chemistry. p.87. ISBN978-1-84755-909-8.
↑ Taylor M (March 22, 1996). "OBITUARY — Ron Thelin". SFGate. Archived from the original on August 28, 2021. Retrieved May 13, 2020.
↑ Rubin R, Melnick JP (2007). Immigration and American Popular Culture: an Introduction. New York, NY: New York University Press. pp.162–4. ISBN978-0-8147-7552-3.
↑ Prown P, Newquist HP, Eiche JF (1997). Legends of Rock Guitar: the Essential Reference of Rock's Greatest Guitarists. London: Hal Leonard Corporation, 1997. p.48. ISBN0-7935-4042-9.
↑ Thompson T (June 16, 1967). "The New Far-Out Beatles". Life. Chicago: Time Inc. p.101. Archived from the original on November 17, 2021. Retrieved December 8, 2016.
↑ "Poisons Standard". Therapeutic Goods Administration. Australian Government Department of Health. July 2016. Archived from the original on March 2, 2017.
↑ Explanatory Report to Act No. 112/1998 Coll., which amends the Act No. 140/1961 Coll., the Criminal Code, and the Act No. 200/1990 Coll., on misdemeanors (Report) (in Czech). Prague: Parliament of the Czech Republic. 1998.
↑ MacLean JR, Macdonald DC, Ogden F, Wilby E (1967). "LSD-25 and mescaline as therapeutic adjuvants.". In Abramson H (ed.). The Use of LSD in Psychotherapy and Alcoholism. New York: Bobbs-Merrill. pp.407–426.
↑ Ditman KS, Bailey JJ. "Evaluating LSD as a psychotherapeutic agent". In Hoffer A (ed.). A program for the treatment of alcoholism: LSD, malvaria, and nicotinic acid. pp.353–402.
↑ Bogenschutz MP (March 2013). "Studying the effects of classic hallucinogens in the treatment of alcoholism: rationale, methodology, and current research with psilocybin". Current Drug Abuse Reviews. 6 (1): 17–29. doi:10.2174/15733998113099990002. PMID23627783.
↑ Vollenweider FX, Kometer M (September 2010). "The neurobiology of psychedelic drugs: implications for the treatment of mood disorders". Nature Reviews. Neuroscience. 11 (9): 642–51. doi:10.1038/nrn2884. PMID20717121. S2CID16588263.
↑ Sessa B (November 2008). "Is it time to revisit the role of psychedelic drugs in enhancing human creativity?". Journal of Psychopharmacology. 22 (8): 821–827. doi:10.1177/0269881108091597. PMID18562421. S2CID1908638.
↑ Penner J (June 17, 2019). "Blowing The Philosopher's Fuses: Michel Foucault's LSD Trip in The Valley of Death". Los Angeles Review of Books. Archived from the original on April 11, 2021. Retrieved April 11, 2021. Wade: "We fell silent to listen to Stockhausen's Songs of Youth. Zabriskie Point was filled with the sound of a kindergarten playground overlaid with electric tonalities. Kontakte followed. Glissandos bounced off the stars, which glowed like incandescent pinballs. Foucault turned to Michael and said this is the first time he really understood what Stockhausen had achieved".
↑ Wade S (2019). Foucault in California: [A True Story-–Wherein the Great French Philosopher Drops Acid in the Valley of Death]. Heyday Books. ISBN9781597144636. In a letter to Wade, dated 16 September 1978, Foucault authorised the book's publication and added: "How could I not love you?"
↑ Harrison A (January 16, 2006). "LSD: The Geek's Wonder Drug?". Wired. Archived from the original on May 5, 2008. Retrieved March 11, 2008. Like Herbert, many scientists and engineers also report heightened states of creativity while using LSD. During a press conference on Friday, Hofmann revealed that he was told by Nobel-prize-winning chemist Kary Mullis that LSD had helped him develop the polymerase chain reaction that helps amplify specific DNA sequences.
↑ Sacks O (2012). Hallucinations. Vintage Books. p.106. ISBN978-0-307-94743-7. Archived from the original on April 21, 2021. Retrieved June 30, 2018. On the West Coast in the early 1960s LSD and morning glory seeds were readily available, so I sampled those, too.
This page is based on this Wikipedia article Text is available under the CC BY-SA 4.0 license; additional terms may apply. Images, videos and audio are available under their respective licenses.