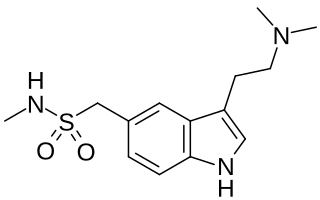
Sumatriptan, sold under the brand name Imitrex among others, is a medication used to treat migraine headaches and cluster headaches. It is taken orally, intranasally, or by subcutaneous injection. Therapeutic effects generally occur within three hours.

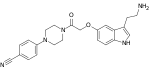
Frovatriptan, sold under the brand name Frova, is a triptan drug developed by Vernalis for the treatment of migraine headaches and for short term prevention of menstrual migraine. The product is licensed to Endo Pharmaceuticals in North America and Menarini in Europe.
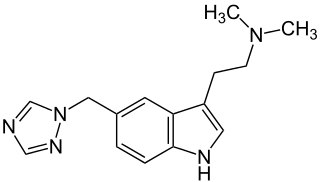
Rizatriptan, sold under the brand name Maxalt among others, is a medication used for the treatment of migraine headaches. It is taken by mouth. It can also be applied on the tongue. It is a serotonin (5-HT) 1B/1D receptor agonist (triptan).
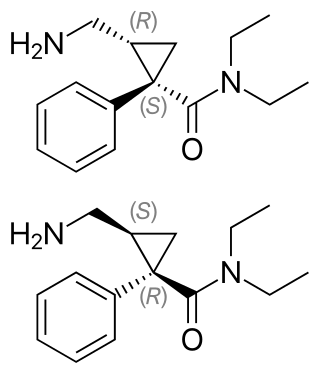
Milnacipran is a serotonin–norepinephrine reuptake inhibitor (SNRI) used in the clinical treatment of fibromyalgia. It is not approved for the clinical treatment of major depressive disorder in the US, but it is in other countries.

Dihydroergotamine (DHE), sold under the brand names D.H.E. 45 and Migranal among others, is an ergot alkaloid used to treat migraines. It is a derivative of ergotamine. It is administered as a nasal spray or injection and has an efficacy similar to that of sumatriptan. Nausea is a common side effect.
Methysergide, sold under the brand names Deseril and Sansert, is a monoaminergic medication of the ergoline and lysergamide groups which is used in the prophylaxis and treatment of migraine and cluster headaches. It has been withdrawn from the market in the United States and Canada due to adverse effects. It is taken by mouth.

Almotriptan is a triptan medication discovered and developed by Almirall for the treatment of heavy migraine headache.

A serotonin receptor agonist is an agonist of one or more serotonin receptors. They activate serotonin receptors in a manner similar to that of serotonin, a neurotransmitter and hormone and the endogenous ligand of the serotonin receptors.

Antimigraine drugs are medications intended to reduce the effects or intensity of migraine headache. They include drugs for the treatment of acute migraine symptoms as well as drugs for the prevention of migraine attacks.

Naratriptan (trade names include Amerge) is a triptan drug marketed by GlaxoSmithKline and is used for the treatment of migraine headaches. It is a selective 5-HT1 receptor subtype agonist.

5-hydroxytryptamine receptor 1B also known as the 5-HT1B receptor is a protein that in humans is encoded by the HTR1B gene. The 5-HT1B receptor is a 5-HT receptor subtype.

5-hydroxytryptamine (serotonin) receptor 1D, also known as HTR1D, is a 5-HT receptor, but also denotes the human gene encoding it. 5-HT1D acts on the central nervous system, and affects locomotion and anxiety. It also induces vasoconstriction in the brain.
Triptans are a family of tryptamine-based drugs used as abortive medication in the treatment of migraines and cluster headaches. They are selective 5-hydroxytryptamine/serotonin1B/1D (5-HT1B/1D) agonists. Migraine is a complex disease which affects about 15% of the population and can be highly disabling. Triptans have advantages over ergotamine and dihydroergotamine, such as selective pharmacology, well established safety record and evidence-based prescribing instructions. Triptans are therefore often preferred treatment in migraine.
Roxindole (EMD-49,980) is a dopaminergic and serotonergic drug which was originally developed by Merck KGaA for the treatment of schizophrenia. In clinical trials its antipsychotic efficacy was only modest but it was unexpectedly found to produce potent and rapid antidepressant and anxiolytic effects. As a result, roxindole was further researched for the treatment of depression instead. It has also been investigated as a therapy for Parkinson's disease and prolactinoma.

PNU-142633 is an experimental drug candidate for the treatment of migraine. It exerts its effect as a selective, high affinity 5-HT1D receptor antagonist. PNU-142633 is well tolerated after oral administration.

Donitriptan (INN) is a triptan drug which was investigated as an antimigraine agent but ultimately was never marketed. It acts as a high-affinity, high-efficacy/near-full agonist of the 5-HT1B and 5-HT1D receptors, and is among the most potent of the triptan series of drugs. Donitriptan was being developed in France by bioMérieux-Pierre Fabre and made it to phase II clinical trials in Europe before development was discontinued.

CP-122,288 is a drug which acts as a potent and selective agonist for the 5-HT1B, 5-HT1D and 5-HT1F serotonin receptor subtypes. It is a derivative of the migraine medication sumatriptan, but while CP-122,288 is 40,000 times more potent than sumatriptan as an inhibitor of neurogenic inflammation and plasma protein extravasation, it is only twice as potent as a constrictor of blood vessels. In human trials, CP-122,288 was not found to be effective as a treatment for migraine, but its selectivity for neurogenic anti-inflammatory action over vasoconstriction has made it useful for research into the underlying causes of migraine.
Ditans are a class of abortive medication for the treatment of migraines. The first ditan, Eli Lilly's lasmiditan, was approved by the FDA in 2019.
Professor Patrick Humphrey OBE DSc PhD HonFBPhS is a South African-born British pharmacologist. He was instrumental in the discovery of the triptans, a group of 5-HT1B and 5-HT1D agonists used to stop single instances of cluster headache or migraine.