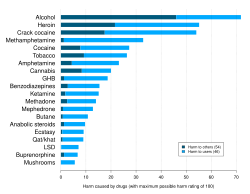
Coffee (containing caffeine) being consumed in a social environment; caffeine is widely legal virtually worldwide making it the most commonly used psychoactive drug.Depiction of alcohol and tobacco (containing nicotine) being used, both of which are commonly legal psychoactive drugs.Chart of relative harmfulness of some psychoactive substances
A psychoactive drug, psychopharmaceutical,[2]mind-altering drug, consciousness-altering drug, psychoactive substance,[3] or psychotropic substance[3] is a chemical substance that alters psychological functioning by modulating central nervous system (CNS) activity.[4][3] Psychoactive and psychotropicdrugs both affect the brain, with psychotropics sometimes referring to psychiatric drugs or high-abuse substances, while “drug” can have negative connotations. Novel psychoactive substances are designer drugs made to mimic illegal ones and bypass laws.
Psychoactive drug use dates back to prehistory for medicinal and consciousness-altering purposes, with evidence of widespread cultural use. Many animals intentionally consume psychoactive substances, and some traditional legends suggest animals first introduced humans to their use. Psychoactive substances are used across cultures for purposes ranging from medicinal and therapeutic treatment of mental disorders and pain, to performance enhancement. Their effects are influenced by the drug itself, the environment, and individual factors. Psychoactive drugs are categorized by their pharmacological effects into types such as anxiolytics (reduce anxiety), empathogen–entactogens (enhance empathy), stimulants (increase CNS activity), depressants (decrease CNS activity), and hallucinogens (alter perception and emotions). Psychoactive drugs are administered through various routes—including oral ingestion, injection, rectal use, and inhalation—with the method and efficiency differing by drug.
The legality of psychoactive drugs has long been controversial, shaped by international treaties like the 1961 Single Convention on Narcotic Drugs and national laws such as the United States Controlled Substances Act. Distinctions are made between recreational and medical use. Enforcement varies across countries. While the 20th century saw global criminalization, recent shifts favor harm reduction and regulation over prohibition. Widely used psychoactive drugs include legal substances like caffeine, alcohol, and nicotine; prescribed medications such as SSRIs, opioids, and benzodiazepines; and illegal recreational drugs like cocaine, LSD, and MDMA.
Psychoactive drug use can be traced to prehistory. Archaeological evidence of the use of psychoactive substances, mostly plants, dates back at least 10,000 years; historical evidence indicates cultural use 5,000 years ago.[5] There is evidence of the chewing of coca leaves, for example, in Peruvian society 8,000 years ago.[6][7]
Psychoactive substances have been used medicinally and to alter consciousness. Consciousness altering may be a primary drive, akin to the need to satiate thirst, hunger, or sexual desire.[8] This may be manifest in the long history of drug use, and even in children's desire for spinning, swinging, or sliding, suggesting that the drive to alter one's state of mind is universal.[9]
In The Hasheesh Eater (1857), American author Fitz Hugh Ludlow was one of the first to describe in modern terms the desire to change one's consciousness through drug use:
[D]rugs are able to bring humans into the neighborhood of divine experience and can thus carry us up from our personal fate and the everyday circumstances of our life into a higher form of reality. It is, however, necessary to understand precisely what is meant by the use of drugs. We do not mean the purely physical craving... That of which we speak is something much higher, namely the knowledge of the possibility of the soul to enter into a lighter being, and to catch a glimpse of deeper insights and more magnificent visions of the beauty, truth, and the divine than we are normally able to spy through the cracks in our prison cell. But there are not many drugs which have the power of stilling such craving. The entire catalog, at least to the extent that research has thus far written it, may include only opium, hashish, and in rarer cases alcohol, which has enlightening effects only upon very particular characters.[10]
During the 20th century, the majority of countries initially responded to the use of recreational drugs by prohibiting production, distribution, or use through criminalization. A notable example occurred with Prohibition in the United States, where early in the century alcohol was made illegal for 13 years. In recent decades, an emerging perspective among governments and law enforcement holds that illicit drug use cannot be stopped through prohibition. One organization holding that view, Law Enforcement Against Prohibition (LEAP), concluded that "[in] fighting a war on drugs the government has increased the problems of society and made them far worse. A system of regulation rather than prohibition is a less harmful, more ethical and a more effective public policy."[11][failed verification]
In some countries and localities, there has been a move away from prohibition and towards harm reduction, where the use of illicit drugs is neither condoned nor promoted, but services and support are provided to ensure users have adequate factual information readily available and to minimize, or eliminate, negative effects of their use. Such is the case with Portugal's drug policy of decriminalization and harm reduction, with a primary goal of reducing the adverse health effects of drug use.[12]
Terminology
Psychoactive and psychotropic are often used interchangeably in general and academic sources, to describe substances that act on the brain to alter cognition and perception; some sources make a distinction between the terms. One narrower definition of psychotropic refers to drugs used to treat mental disorders, such as anxiolytic sedatives, antidepressants, antimanic agents, and neuroleptics. Another usage of psychotropic refers to substances determined to pose "high abuse liability", including stimulants, hallucinogens, opioids, and sedatives/hypnotics including alcohol. In international drug control, psychotropic substances refers to the substances specified in the Convention on Psychotropic Substances, which does not include narcotics.[13]
The term "drug" has become a skunked term. "Drugs" can have a negative connotation, often associated with illegal substances like cocaine or heroin, despite the fact that the terms "drug" and "medicine" are sometimes used interchangeably.[14]
Novel psychoactive substances (NPS)[note 1], also known as "designer drugs" are a category of psychoactive drugs (substances) that are designed to mimic the effects of often illegal drugs, usually in efforts to circumvent existing drug laws.[15]
Types
Psychoactive drugs are divided according to their pharmacological effects. Common subtypes include:
Anxiolytics are medicinally used to reduce the symptoms of anxiety, and sometimes insomnia.
Stimulants increase activity, or arousal, of the central nervous system. They can enhance alertness, attention, cognition, mood and physical performance. Some stimulants are used medicinally to treat individuals with ADHD and narcolepsy.
Depressants reduce, or depress, activity and stimulation in the central nervous system. This category encompasses a spectrum of substances with sedative, soporific, and anesthetic properties, and include sedatives, hypnotics, and opioids.
Three key factors influence drug use: the drug (type, strength, availability, etc.), the individual (age, genetics, personality, etc.) and the environment (relatives, poverty, social norms, drug policy, etc.).
The ways in which psychoactive substances are used vary widely between cultures. Some substances may have controlled or illegal uses, others may have shamanic purposes, and others are used medicinally. Examples would be social drinking, nootropic supplements, and sleep aids. Caffeine is the world's most widely consumed psychoactive substance, and is legal and unregulated in nearly all jurisdictions; in North America, 90% of adults consume caffeine daily.[18]
Psychiatric medications are psychoactive drugs prescribed for the management of mental and emotional disorders, or to aid in overcoming challenging behavior.[19] There are six major classes of psychiatric medications:
Exposure to psychoactive drugs can cause changes to the brain that counteract or augment some of their effects; these changes may be beneficial or harmful. However, there is a significant amount of evidence that the relapse rate of mental disorders negatively corresponds with the length of properly followed treatment regimens (that is, relapse rate substantially declines over time), and to a much greater degree than placebo.[22]
Military
Drugs used by militaries
Two hip flasks, located in the left-center, are featured in the military equipment used as emergency sustenance by the Luftwaffe, which was the air force of Nazi Germany during World War II.
Militaries worldwide have used or are using various psychoactive drugs to treat pain and to improve performance of soldiers by suppressing hunger, increasing the ability to sustain effort without food, increasing and lengthening wakefulness and concentration, suppressing fear, reducing empathy, and improving reflexes and memory-recall among other things.[23][24]
Both military and civilian American intelligence officials are known to have used psychoactive drugs while interrogating captives apprehended in its "war on terror". In July 2012 Jason Leopold and Jeffrey Kaye, psychologists and human rights workers, had a Freedom of Information Act request fulfilled that confirmed that the use of psychoactive drugs during interrogation was a long-standing practice.[25][26] Captives and former captives had been reporting medical staff collaborating with interrogators to drug captives with powerful psychoactive drugs prior to interrogation since the very first captives release.[27][28] In May 2003 recently released Pakistani captiveSha Mohammed Alikhel described the routine use of psychoactive drugs. He said that Jihan Wali, a captive kept in a nearby cell, was rendered catatonic through the use of these drugs.[citation needed]
Alcohol has a long association of military use, and has been called "liquid courage" for its role in preparing troops for battle, anaesthetize injured soldiers, and celebrate military victories. It has also served as a coping mechanism for combat stress reactions and a means of decompression from combat to everyday life. However, this reliance on alcohol can have negative consequences for physical and mental health.[29]
Performance-enhancing substances, also known as performance-enhancing drugs (PEDs),[36] are substances that are used to improve any form of activity performance in humans. A well-known example of cheating in sports involves doping in sport, where banned physical performance-enhancing drugs are used by athletes and bodybuilders. Athletic performance-enhancing substances are sometimes referred as ergogenic aids.[37][38] Cognitive performance-enhancing drugs, commonly called nootropics,[39] are sometimes used by students to improve academic performance. Performance-enhancing substances are also used by military personnel to enhance combat performance.[40]
Global per capita alcohol consumption has shown a downward trajectory since the 20th century, suggesting a shift towards prioritizing health and well-being.
Many psychoactive substances are used for their mood and perception altering effects, including those with accepted uses in medicine and psychiatry. Examples of psychoactive substances include caffeine, alcohol, cocaine, LSD, nicotine, cannabis, and dextromethorphan.[41] Classes of drugs frequently used recreationally include:
Hypnotics, which depress the central nervous system.
Opioid analgesics, which also depress the central nervous system. These are used recreationally because of their euphoric effects.
Inhalants, in the forms of gas aerosols, or solvents, which are inhaled as a vapor because of their stupefying effects. Many inhalants also fall into the above categories (such as nitrous oxide which is also an analgesic).
In some modern and ancient cultures, drug usage is seen as a status symbol. Recreational drugs are seen as status symbols in settings such as at nightclubs and parties.[42] For example, in ancient Egypt, gods were commonly pictured holding hallucinogenic plants.[43]
Because there is controversy about regulation of recreational drugs, there is an ongoing debate about drug prohibition. Critics of prohibition believe that regulation of recreational drug use is a violation of personal autonomy and freedom.[44] In the United States, critics have noted that prohibition or regulation of recreational and spiritual drug use might be unconstitutional, and causing more harm than is prevented.[45]
Some people who take psychoactive drugs experience drug- or substance-induced psychosis. A 2019 systematic review and meta-analysis by Murrie et al. found that the pooled proportion of transition from substance-induced psychosis to schizophrenia was 25% (95% CI 18%–35%), compared with 36% (95% CI 30%–43%) for brief, atypical and not otherwise specified psychoses.[46] Type of substance was the primary predictor of transition from drug-induced psychosis to schizophrenia, with highest rates associated with cannabis (6 studies, 34%, CI 25%–46%), hallucinogens (3 studies, 26%, CI 14%–43%) and amphetamines (5 studies, 22%, CI 14%–34%). Lower rates were reported for opioid (12%), alcohol (10%) and sedative (9%) induced psychoses. Transition rates were slightly lower in older cohorts but were not affected by sex, country of the study, hospital or community location, urban or rural setting, diagnostic methods, or duration of follow-up.[46]
Ritual and spiritual
Offerings
Alcohol and tobacco (nicotine) have been and are used as offerings in various religions and spiritual practices.[citation needed]Coca leaves have been used as offerings in rituals.[47]
According to the Catholic Church, the sacramental wine used in the Eucharist must contain alcohol. Canon 924 of the present Code of Canon Law (1983) states:
§3 The wine must be natural, made from grapes of the vine, and not corrupt.[48]
Timothy Leary was a leading proponent of spiritual hallucinogen use.
Certain psychoactives, particularly hallucinogens, have been used for religious purposes since prehistoric times. Native Americans have used peyote cacti containing mescaline for religious ceremonies for as long as 5700 years.[49] The muscimol-containing Amanita muscaria mushroom was used for ritual purposes throughout prehistoric Europe.[50]
The use of entheogens for religious purposes resurfaced in the West during the counterculture movements of the 1960s and 70s. Under the leadership of Timothy Leary, new spiritual and intention-based movements began to use LSD and other hallucinogens as tools to access deeper inner exploration. In the United States, the use of peyote for ritual purposes is protected only for members of the Native American Church, which is allowed to cultivate and distribute peyote. However, the genuine religious use of peyote, regardless of one's personal ancestry, is protected in Colorado, Arizona, New Mexico, Nevada, and Oregon.[51]
The aims and methods of psychonautics, when state-altering substances are involved, is commonly distinguished from recreational drug use by research sources.[56] Psychonautics as a means of exploration need not involve drugs, and may take place in a religious context with an established history. Cohen considers psychonautics closer in association to wisdom traditions and other transpersonal and integral movements.[57]
Self-medication, sometime called do-it-yourself (DIY) medicine, is a human behavior in which an individual uses a substance or any exogenous influence to self-administer treatment for physical or psychological conditions, for example headaches or fatigue.
The substances most widely used in self-medication are over-the-counter drugs and dietary supplements, which are used to treat common health issues at home. These do not require a doctor'sprescription to obtain and, in some countries, are available in supermarkets and convenience stores.[58]
In the US, NORML (National Organization for the Reform of Marijuana Laws) has led since the 1970s a movement to legalize cannabis nationally.[59] The so-called "420 movement" is the global association of the number 420 with cannabis consumption: April 20th – fourth month, twentieth day – has become an international countercultureholiday based on the celebration and consumption of cannabis;[60][61][62] 4:20 pm on any day is a time to consume cannabis.[63][64]
Operation Overgrow
Operation Overgrow is the name, given by cannabis activists, of an "operation" to spread marijuana seeds wildly "so it grows like weed".[65] The thought behind the operation is to draw attention to the debate about legalization/decriminalization of marijuana.
A drug overdose involves taking a dose of a drug that exceeds safe levels. In the UK (England and Wales) until 2013, a drug overdose was the most common suicide method in females.[66] In 2019 in males the percentage is 16%. Self-poisoning accounts for the highest number of non-fatal suicide attempts. In the United States about 60% of suicide attempts and 14% of suicide deaths involve drug overdoses.[67] The case fatality rate of suicide attempts involving overdose is about 2%.[67]
Most people are under the influence of sedative-hypnotic drugs (such as alcohol or benzodiazepines) when they die by suicide,[68] with alcoholism present in between 15% and 61% of cases.[69] Countries that have higher rates of alcohol use and a greater density of bars generally also have higher rates of suicide.[70] About 2.2–3.4% of those who have been treated for alcoholism at some point in their life die by suicide.[70] Alcoholics who attempt suicide are usually male, older, and have tried to take their own lives in the past.[69] In adolescents who misuse alcohol, neurological and psychological dysfunctions may contribute to the increased risk of suicide.[71]
Overdose attempts using painkillers are among the most common, due to their easy availability over-the-counter.[72]
The theory of dosage, set, and setting is a useful model in dealing with the effects of psychoactive substances, especially in a controlled therapeutic setting as well as in recreational use. Dr. Timothy Leary, based on his own experiences and systematic observations on psychedelics, developed this theory along with his colleagues Ralph Metzner, and Richard Alpert (Ram Dass) in the 1960s.[74]
Dosage
The first factor, dosage, has been a truism since ancient times, or at least since Paracelsus who said, "Dose makes the poison." Some compounds are beneficial or pleasurable when consumed in small amounts, but harmful, deadly, or evoke discomfort in higher doses.
Set
The set is the internal attitudes and constitution of the person, including their expectations, wishes, fears, and sensitivity to the drug. This factor is especially important for the hallucinogens, which have the ability to make conscious experiences out of the unconscious. In traditional cultures, set is shaped primarily by the worldview, health and genetic characteristics that all the members of the culture share.
Setting
The third aspect is setting, which pertains to the surroundings, the place, and the time in which the experiences transpire.
This theory clearly states that the effects are equally the result of chemical, pharmacological, psychological, and physical influences. The model that Timothy Leary proposed applied to the psychedelics, although it also applies to other psychoactives.[75]
Illustration of the major elements of neurotransmission. Depending on its method of action, a psychoactive substance may block the receptors on the post-synaptic neuron (dendrite), or block reuptake or affect neurotransmitter synthesis in the pre-synaptic neuron (axon).
Psychoactive drugs operate by temporarily affecting a person's neurochemistry, which in turn causes changes in a person's mood, cognition, perception and behavior. There are many ways in which psychoactive drugs can affect the brain. Each drug has a specific action on one or more neurotransmitter or neuroreceptor in the brain.
Drugs that increase activity in particular neurotransmitter systems are called agonists. They act by increasing the synthesis of one or more neurotransmitters, by reducing its reuptake from the synapses, or by mimicking the action by binding directly to the postsynaptic receptor. Drugs that reduce neurotransmitter activity are called antagonists, and operate by interfering with synthesis or blocking postsynaptic receptors so that neurotransmitters cannot bind to them.[76]
Exposure to a psychoactive substance can cause changes in the structure and functioning of neurons, as the nervous system tries to re-establish the homeostasis disrupted by the presence of the drug (see also, neuroplasticity). Exposure to antagonists for a particular neurotransmitter can increase the number of receptors for that neurotransmitter or the receptors themselves may become more responsive to neurotransmitters; this is called sensitization. Conversely, overstimulation of receptors for a particular neurotransmitter may cause a decrease in both number and sensitivity of these receptors, a process called desensitization or tolerance. Sensitization and desensitization are more likely to occur with long-term exposure, although they may occur after only a single exposure. These processes are thought to play a role in drug dependence and addiction.[77]Physical dependence on antidepressants or anxiolytics may result in worse depression or anxiety, respectively, as withdrawal symptoms. Unfortunately, because clinical depression (also called major depressive disorder) is often referred to simply as depression, antidepressants are often requested by and prescribed for patients who are depressed, but not clinically depressed.
Affected neurotransmitter systems
The following is a brief table of notable drugs and their primary neurotransmitter, receptor or method of action. Many drugs act on more than one transmitter or receptor in the brain.[78]
addiction – a neuropsychological disorder characterized by a persistent and intense urge to use a drug or engage in a behavior that produces natural reward
addictive drug – psychoactive substances that with repeated use are associated with significantly higher rates of substance use disorders, due in large part to the drug's effect on brain reward systems
dependence – an adaptive state associated with a withdrawal syndrome upon cessation of repeated exposure to a stimulus (e.g., drug intake)
drug sensitization or reverse tolerance – the escalating effect of a drug resulting from repeated administration at a given dose
drug withdrawal – symptoms that occur upon cessation of repeated drug use
psychological dependence – dependence that is characterised by emotional-motivational withdrawal symptoms (e.g., anhedonia and anxiety) that affect cognitive functioning.
reinforcing stimuli – stimuli that increase the probability of repeating behaviors paired with them
rewarding stimuli – stimuli that the brain interprets as intrinsically positive and desirable or as something to approach
sensitization – an amplified response to a stimulus resulting from repeated exposure to it
substance use disorder – a condition in which the use of substances leads to clinically and functionally significant impairment or distress
drug tolerance – the diminishing effect of a drug resulting from repeated administration at a given dose
Comparison of the perceived harm for various psychoactive drugs from a poll among medical psychiatrists specialized in addiction treatment (David Nutt et al. 2007)
Psychoactive drugs are often associated with addiction or drug dependence. Dependence can be divided into two types: psychological dependence, by which a user experiences negative psychological or emotional withdrawal symptoms (e.g., depression) and physical dependence, by which a user must use a drug to avoid physically uncomfortable or even medically harmful physical withdrawal symptoms.[91] Drugs that are both rewarding and reinforcing are addictive; these properties of a drug are mediated through activation of the mesolimbic dopamine pathway, particularly the nucleus accumbens. Not all addictive drugs are associated with physical dependence, e.g., amphetamine, and not all drugs that produce physical dependence are addictive drugs, e.g., oxymetazoline.
Globally, as of 2016, alcohol use disorders were the most prevalent of all substance use disorders (SUD) worldwide; cannabis dependence and opioid dependence were the next most prevalent SUDs.[92]
Many professionals, self-help groups, and businesses specialize in drug rehabilitation, with varying degrees of success, and many parents attempt to influence the actions and choices of their children regarding psychoactives.[93]
The legality of psychoactive drugs has been controversial through most of recent history; the Second Opium War and Prohibition are two historical examples of legal controversy surrounding psychoactive drugs. However, in recent years, the most influential document regarding the legality of psychoactive drugs is the Single Convention on Narcotic Drugs, an international treaty signed in 1961 as an Act of the United Nations. Signed by 73 nations including the United States, the USSR, Pakistan, India, and the United Kingdom, the Single Convention on Narcotic Drugs established Schedules for the legality of each drug and laid out an international agreement to fight addiction to recreational drugs by combatting the sale, trafficking, and use of scheduled drugs.[96] All countries that signed the treaty passed laws to implement these rules within their borders. However, some countries that signed the Single Convention on Narcotic Drugs, such as the Netherlands, are more lenient with their enforcement of these laws.[97]
In the United States, the Food and Drug Administration (FDA) has authority over all drugs, including psychoactive drugs. The FDA regulates which psychoactive drugs are over the counter and which are only available with a prescription.[98] However, certain psychoactive drugs, like alcohol, tobacco, and drugs listed in the Single Convention on Narcotic Drugs are subject to criminal laws. The Controlled Substances Act of 1970 regulates the recreational drugs outlined in the Single Convention on Narcotic Drugs.[99] Alcohol is regulated by state governments, but the federal National Minimum Drinking Age Act penalizes states for not following a national drinking age.[100] Tobacco is also regulated by all fifty state governments.[101] Most people accept such restrictions and prohibitions of certain drugs, especially the "hard" drugs, which are illegal in most countries.[102][103][104]
In the medical context, psychoactive drugs as a treatment for illness is widespread and generally accepted. Little controversy exists concerning over the counter psychoactive medications in antiemetics and antitussives. Psychoactive drugs are commonly prescribed to patients with psychiatric disorders. However, certain critics [who?] believe that certain prescription psychoactives, such as antidepressants and stimulants, are overprescribed and threaten patients' judgement and autonomy.[105][106]
A number of animals consume different psychoactive plants, animals, berries and even fermented fruit, becoming intoxicated. An example of this is cats after consuming catnip. Traditional legends of sacred plants often contain references to animals that introduced humankind to their use.[107] Animals and psychoactive plants appear to have co-evolved, possibly explaining why these chemicals and their receptors exist within the nervous system.[108]
Widely used psychoactive drugs
This is a list of commonly used drugs that contain psychoactive ingredients. Please note that the following lists contains legal and illegal drugs (based on the country's laws).
Common legal drugs
The most widely consumed psychotropic drugs worldwide are:[109]
↑"New Psychoactive Substance", and "Novel Psychoactive Substance" (NPS) are often used interchangeably.
↑MDMA and Ketamine are not a classical psychedelics but are sometimes discussed alongside classical psychedelics due to similarities in their psychoactive and potentially therapeutic effects.[52]
References
↑Nehlig A, Daval JL, Debry G (1992). "Caffeine and the central nervous system: mechanisms of action, biochemical, metabolic and psychostimulant effects". Brain Research. Brain Research Reviews. 17 (2): 139–170. doi:10.1016/0165-0173(92)90012-B. PMID1356551. S2CID14277779.
↑Bersani FS, Corazza O, Simonato P, Mylokosta A, Levari E, Lovaste R, Schifano F (2013). "Drops of madness? Recreational misuse of tropicamide collyrium; early warning alerts from Russia and Italy". General Hospital Psychiatry. 35 (5): 571–3. doi:10.1016/j.genhosppsych.2013.04.013. PMID23706777.
↑Lovett R (24 September 2005). "Coffee: The demon drink?"(fee required). New Scientist (2518). Archived from the original on 24 October 2007. Retrieved 2007-11-19.
↑Matson JL, Neal D (2009). "Psychotropic medication use for challenging behaviors in persons with intellectual disabilities: An overview". Research in Developmental Disabilities. 30 (3): 572–86. doi:10.1016/j.ridd.2008.08.007. PMID18845418.
↑Schatzberg AF (2000). "New indications for antidepressants". The Journal of Clinical Psychiatry. 61 (11): 9–17. PMID10926050.
↑Robert Beckhusen (2012-07-11). "U.S. Injected Gitmo Detainees With 'Mind Altering' Drugs". Wired magazine. Archived from the original on 2012-07-13. Retrieved 2012-07-14. That's according to a recently declassified report (.pdf) from the Pentagon's inspector general, obtained by Truthout's Jeffrey Kaye and Jason Leopold after a Freedom of Information Act Request. In it, the inspector general concludes that 'certain detainees, diagnosed as having serious mental health conditions being treated with psychoactive medications on a continuing basis, were interrogated.' The report does not conclude, though, that anti-psychotic drugs were used specifically for interrogation purposes.
↑Haroon Rashid (2003-05-23). "Pakistani relives Guantanamo ordeal". BBC News. Archived from the original on 2012-10-31. Retrieved 2009-01-09. Mr Shah alleged that the Americans had given him injections and tablets prior to interrogations. "They used to tell me I was mad," the 23-year-old told the BBC in his native village in Dir district near the Afghan border. I was given injections at least four or five times as well as different tablets. I don't know what they were meant for."
↑"People the law forgot". The Guardian. 2003-12-03. Archived from the original on 2013-08-27. Retrieved 2012-07-14. The biggest damage is to my brain. My physical and mental state isn't right. I'm a changed person. I don't laugh or enjoy myself much.
↑Jones E, Fear NT (April 2011). "Alcohol use and misuse within the military: a review". International Review of Psychiatry. 23 (2): 166–172. doi:10.3109/09540261.2010.550868. PMID21521086.
↑"Aimo Allan Koivunen". www.sotapolku.fi (in Finnish). 2016. Retrieved January 17, 2022.
↑Quiding H, Lundqvist G, Boréus LO, Bondesson U, Ohrvik J (1993). "Analgesic effect and plasma concentrations of codeine and morphine after two dose levels of codeine following oral surgery". European Journal of Clinical Pharmacology. 44 (4): 319–23. doi:10.1007/BF00316466. PMID8513842. S2CID37268044.
↑Medline Plus. Anesthesia. Accessed on July 16, 2007.
↑Liddle DG, Connor DJ (June 2013). "Nutritional supplements and ergogenic AIDS". Primary Care. 40 (2): 487–505. doi:10.1016/j.pop.2013.02.009. PMID23668655. Amphetamines and caffeine are stimulants that increase alertness, improve focus, decrease reaction time, and delay fatigue, allowing for an increased intensity and duration of training... Physiologic and performance effects [of amphetamines] •Amphetamines increase dopamine/norepinephrine release and inhibit their reuptake, leading to central nervous system (CNS) stimulation •Amphetamines seem to enhance athletic performance in anaerobic conditions 39 40 •Improved reaction time •Increased muscle strength and delayed muscle fatigue •Increased acceleration •Increased alertness and attention to task
↑Frati P, Kyriakou C, Del Rio A, Marinelli E, Vergallo GM, Zaami S, Busardò FP (January 2015). "Smart drugs and synthetic androgens for cognitive and physical enhancement: revolving doors of cosmetic neurology". Current Neuropharmacology. 13 (1): 5–11. doi:10.2174/1570159X13666141210221750. PMC4462043. PMID26074739. Cognitive enhancement can be defined as the use of drugs and/or other means with the aim to improve the cognitive functions of healthy subjects in particular memory, attention, creativity and intelligence in the absence of any medical indication.... The first aim of this paper was to review current trends in the misuse of smart drugs (also known as Nootropics) presently available on the market focusing in detail on methylphenidate, trying to evaluate the potential risk in healthy individuals, especially teenagers and young adults.
↑El-Seedi HR, De Smet PA, Beck O, Possnert G, Bruhn JG (2005). "Prehistoric peyote use: alkaloid analysis and radiocarbon dating of archaeological specimens of Lophophora from Texas". Journal of Ethnopharmacology. 101 (1–3): 238–42. doi:10.1016/j.jep.2005.04.022. PMID15990261.
↑Vetulani J (2001). "Drug addiction. Part I. Psychoactive substances in the past and presence". Polish Journal of Pharmacology. 53 (3): 201–14. PMID11785921.
↑Bullis RK (1990). "Swallowing the scroll: legal implications of the recent Supreme Court peyote cases". Journal of Psychoactive Drugs. 22 (3): 325–32. doi:10.1080/02791072.1990.10472556. PMID2286866.
12Conner A, Azrael D, Miller M (3 December 2019). "Suicide Case-Fatality Rates in the United States, 2007 to 2014"(PDF). Annals of Internal Medicine. 171 (12): 885–895. doi:10.7326/M19-1324. PMID31791066. S2CID208611916. Archived from the original(PDF) on 28 January 2021. Table 1. Suicide Deaths, Nonfatal Suicide Attempts, and Total Suicidal Acts, Overall and by [...] Method [(Table contents' transcription:) Out of 3,657,886 recorded suicide attempts, 309,377 (8.46%) resulted in deaths; 2,171,482 of these suicidal acts are based on drug poisoning, 41,758 (1.92%) of which resulted in deaths.]
↑Youssef NA, Rich CL (2008). "Does acute treatment with sedatives/hypnotics for anxiety in depressed patients affect suicide risk? A literature review". Annals of Clinical Psychiatry. 20 (3): 157–169. doi:10.1080/10401230802177698. PMID18633742.
↑Sher L (2007). "Functional magnetic resonance imaging in studies of the neurobiology of suicidal behavior in adolescents with alcohol use disorders". International Journal of Adolescent Medicine and Health. 19 (1): 11–18. doi:10.1515/ijamh.2007.19.1.11. PMID17458319. S2CID42672912.
↑Di Carlo G, Borrelli F, Ernst E, Izzo AA (2001). "St John's wort: Prozac from the plant kingdom". Trends in Pharmacological Sciences. 22 (6): 292–7. doi:10.1016/S0165-6147(00)01716-8. PMID11395157.
↑Herraiz T, Chaparro C (2006). "Human monoamine oxidase enzyme inhibition by coffee and β-carbolines norharman and harman isolated from coffee". Life Sciences. 78 (8): 795–802. doi:10.1016/j.lfs.2005.05.074. PMID16139309.
↑Malenka RC, Nestler EJ, Hyman SE (2009). "Chapter 15: Reinforcement and Addictive Disorders". In Sydor A, Brown RY (eds.). Molecular Neuropharmacology: A Foundation for Clinical Neuroscience (2nded.). New York: McGraw-Hill Medical. pp.364–375. ISBN9780071481274.
↑Nestler EJ (December 2013). "Cellular basis of memory for addiction". Dialogues in Clinical Neuroscience. 15 (4): 431–443. PMC3898681. PMID24459410. Despite the importance of numerous psychosocial factors, at its core, drug addiction involves a biological process: the ability of repeated exposure to a drug of abuse to induce changes in a vulnerable brain that drive the compulsive seeking and taking of drugs, and loss of control over drug use, that define a state of addiction.... A large body of literature has demonstrated that such ΔFosB induction in D1-type [nucleus accumbens] neurons increases an animal's sensitivity to drug as well as natural rewards and promotes drug self-administration, presumably through a process of positive reinforcement... Another ΔFosB target is cFos: as ΔFosB accumulates with repeated drug exposure it represses c-Fos and contributes to the molecular switch whereby ΔFosB is selectively induced in the chronic drug-treated state.41.... Moreover, there is increasing evidence that, despite a range of genetic risks for addiction across the population, exposure to sufficiently high doses of a drug for long periods of time can transform someone who has relatively lower genetic loading into an addict.
↑Volkow ND, Koob GF, McLellan AT (January 2016). "Neurobiologic Advances from the Brain Disease Model of Addiction". New England Journal of Medicine. 374 (4): 363–371. doi:10.1056/NEJMra1511480. PMC6135257. PMID26816013. Substance-use disorder: A diagnostic term in the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) referring to recurrent use of alcohol or other drugs that causes clinically and functionally significant impairment, such as health problems, disability, and failure to meet major responsibilities at work, school, or home. Depending on the level of severity, this disorder is classified as mild, moderate, or severe. Addiction: A term used to indicate the most severe, chronic stage of substance-use disorder, in which there is a substantial loss of self-control, as indicated by compulsive drug taking despite the desire to stop taking the drug. In the DSM-5, the term addiction is synonymous with the classification of severe substance-use disorder.
↑Johnson B (2003). "Psychological Addiction, Physical Addiction, Addictive Character, and Addictive Personality Disorder: A Nosology of Addictive Disorders". Canadian Journal of Psychoanalysis. 11 (1): 135–60. OCLC208052223.
↑Hops H, Tildesley E, Lichtenstein E, Ary D, Sherman L (2009). "Parent-Adolescent Problem-Solving Interactions and Drug Use". The American Journal of Drug and Alcohol Abuse. 16 (3–4): 239–58. doi:10.3109/00952999009001586. PMID2288323.
This page is based on this Wikipedia article Text is available under the CC BY-SA 4.0 license; additional terms may apply. Images, videos and audio are available under their respective licenses.