Both racemic methamphetamine and dextromethamphetamine are illicitly trafficked and sold owing to their potential for recreational use and ease of manufacture. The highest prevalence of illegal methamphetamine use occurs in parts of Asia and Oceania, and in the United States, where racemic methamphetamine and dextromethamphetamine are classified as Schedule II controlled substances. Levomethamphetamine is available as an over-the-counter (OTC) drug for use as an inhaled nasal decongestant in the United States and is seldom abused.[28][note 4] Internationally, the production, distribution, sale, and possession of methamphetamine is restricted or banned in many countries, owing to its placement in schedule II of the United Nations Convention on Psychotropic Substances treaty. While dextromethamphetamine is a more potent drug, racemic methamphetamine is illicitly produced more often, owing to the relative ease of synthesis and regulatory limits of chemical precursor availability.
In the United States, methamphetamine hydrochloride, sold under the brand name Desoxyn, is FDA-approved for the treatment of attention deficit hyperactivity disorder (ADHD);[27][35] however, the FDA notes that the limited therapeutic usefulness of methamphetamine should be weighed against the risks associated with its use.[27] To avoid toxicity and risk of side effects, FDA guidelines recommend an initial dose of methamphetamine at doses 5–10mg/day for ADHD in adults and children over six years of age, and may be increased at weekly intervals of 5mg, up to 25mg/day, until optimum clinical response is found; the usual effective dose is around 20–25mg/day.[25][7][27] Methamphetamine is sometimes prescribed off-label for obesity, narcolepsy, and idiopathic hypersomnia.[25][36][37] In the United States, methamphetamine's levorotary form is available in some over-the-counter (OTC) nasal decongestant products.[25][note 4]
Although the pharmaceutical name "methamphetamine hydrochloride" may suggest a racemic mixture, Desoxyn contains enantiopure dextromethamphetamine, which is a more potent stimulant than both levomethamphetamine and racemic methamphetamine.[25][note 3] This naming convention deviates from the standard practice observed with other stimulants, such as Adderall and dextroamphetamine, where the dextrorotary enantiomer is explicitly identified as an active ingredient in both generic and brand-name pharmaceuticals.[38][39][40]
As methamphetamine is associated with a high potential for misuse, the drug is regulated under the Controlled Substances Act and is listed under Schedule II in the United States.[3] Methamphetamine hydrochloride dispensed in the United States is required to include a boxed warning regarding its potential for recreational misuse and addiction liability.[27]
Desoxyn Gradumet was an extended-release form of the drug. It is no longer produced.[41]
Methamphetamine is often used recreationally for its effects as a potent euphoriant and stimulant as well as aphrodisiac qualities.[42]
According to a National Geographic TV documentary on methamphetamine, an entire subculture known as party and play is based around sexual activity and methamphetamine use.[42] Participants in this subculture, which consists almost entirely of homosexual male methamphetamine users, will typically meet up through internet dating sites and have sex.[42] Because of its strong stimulant and aphrodisiac effects and inhibitory effect on ejaculation, with repeated use, these sexual encounters will sometimes occur continuously for several days on end.[42] The crash following the use of methamphetamine in this manner is very often severe, with marked hypersomnia (excessive daytime sleepiness).[42] The party and play subculture is prevalent in major US cities such as San Francisco and New York City.[42][43]
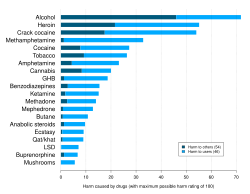
A 2010 study ranking various illegal and legal drugs based on statements by drug-harm experts. Methamphetamine was found to be the fourth most damaging to users. However, Nutt's concept and methodology were criticised sharply from a scientific perspective.Main short and long term adverse physical and mental effects that may appear in methamphetamine use
Methamphetamine users, particularly heavy users, may lose their teeth abnormally quickly, regardless of the route of administration, from a condition informally known as meth mouth.[53] The condition is generally most severe in users who inject the drug, rather than swallow, smoke, or inhale it.[53] According to the American Dental Association, meth mouth "is probably caused by a combination of drug-induced psychological and physiological changes resulting in xerostomia (dry mouth), extended periods of poor oral hygiene, frequent consumption of high-calorie, carbonated beverages and bruxism (teeth grinding and clenching)".[53][54] As dry mouth is also a common side effect of other stimulants, which are not known to contribute severe tooth decay, many researchers suggest that methamphetamine-associated tooth decay is more due to users' other choices. They suggest the side effect has been exaggerated and stylized to create a stereotype of current users as a deterrence for new ones.[35]
Sexually transmitted infection
Methamphetamine use was found to be related to higher frequencies of unprotected sexual intercourse in both HIV-positive and unknown casual partners, an association more pronounced in HIV-positive participants.[55] These findings suggest that methamphetamine use and engagement in unprotected anal intercourse are co-occurring risk behaviors, behaviors that potentially heighten the risk of HIV transmission among gay and bisexual men.[55] Methamphetamine use allows users of both sexes to engage in prolonged sexual activity, which may cause genital sores and abrasions as well as priapism in men.[27][56] Methamphetamine may also cause sores and abrasions in the mouth via bruxism, increasing the risk of sexually transmitted infection.[27][56]
Besides the sexual transmission of HIV, it may also be transmitted between users who share a common needle.[57] The level of needle sharing among methamphetamine users is similar to that among other drug injection users.[57]
Methamphetamine is neurotoxic to dopaminergic systems in lab animals and is associated with dopaminergic toxicity in humans.[33][34]Excitotoxicity, oxidative stress, metabolic compromise, UPS dysfunction, protein nitration, endoplasmic reticulum stress, p53 expression and other processes contributed to this neurotoxicity.[33][65][4] In line with its dopaminergic neurotoxicity, methamphetamine use is associated with a higher risk of Parkinson's disease.[66] In addition to its dopaminergic neurotoxicity, a review of human studies indicated that chronic methamphetamine use is associated with serotonergic neurotoxicity.[34] It has been demonstrated that a high core temperature is correlated with an increase in the neurotoxic effects of methamphetamine.[67] Withdrawal of methamphetamine in dependent persons may lead to post-acute withdrawal which persists months beyond the typical withdrawal period.[4]
Methamphetamine has been shown to activate TAAR1 in human astrocytes and generate cAMP as a result.[66] Activation of astrocyte-localized TAAR1 appears to function as a mechanism by which methamphetamine attenuates membrane-bound EAAT2 (SLC1A2) levels and function in these cells.[66]
Methamphetamine binds to and activates both sigma receptor subtypes, σ1 and σ2, with micromolar affinity.[64][68] Sigma receptor activation may promote methamphetamine-induced neurotoxicity by facilitating hyperthermia, increasing dopamine synthesis and release, influencing microglial activation, and modulating apoptotic signaling cascades and the formation of reactive oxygen species.[64][68]
addiction – a neuropsychological disorder characterized by a persistent and intense urge to use a drug or engage in a behavior that produces natural reward
addictive drug – psychoactive substances that with repeated use are associated with significantly higher rates of substance use disorders, due in large part to the drug's effect on brain reward systems
dependence – an adaptive state associated with a withdrawal syndrome upon cessation of repeated exposure to a stimulus (e.g., drug intake)
drug sensitization or reverse tolerance – the escalating effect of a drug resulting from repeated administration at a given dose
drug withdrawal – symptoms that occur upon cessation of repeated drug use
psychological dependence – dependence that is characterised by emotional-motivational withdrawal symptoms (e.g., anhedonia and anxiety) that affect cognitive functioning.
reinforcing stimuli – stimuli that increase the probability of repeating behaviors paired with them
rewarding stimuli – stimuli that the brain interprets as intrinsically positive and desirable or as something to approach
sensitization – an amplified response to a stimulus resulting from repeated exposure to it
substance use disorder – a condition in which the use of substances leads to clinically and functionally significant impairment or distress
drug tolerance – the diminishing effect of a drug resulting from repeated administration at a given dose
This diagram depicts the signaling events in the brain's reward center that are induced by chronic high-dose exposure to psychostimulants that increase the concentration of synaptic dopamine, like amphetamine, methamphetamine, and phenethylamine. Following presynaptic dopamine and glutamateco-release by such psychostimulants,[72][73]postsynaptic receptors for these neurotransmitters trigger internal signaling events through a cAMP-dependent pathway and a calcium-dependent pathway that ultimately result in increased CREB phosphorylation.[72][74][75] Phosphorylated CREB increases levels of ΔFosB, which in turn represses the c-Fos gene with the help of corepressors;[72][76][77]c-Fosrepression acts as a molecular switch that enables the accumulation of ΔFosB in the neuron.[78] A highly stable (phosphorylated) form of ΔFosB, one that persists in neurons for 1–2months, slowly accumulates following repeated high-dose exposure to stimulants through this process.[76][77] ΔFosB functions as "one of the master control proteins" that produces addiction-related structural changes in the brain, and upon sufficient accumulation, with the help of its downstream targets (e.g., nuclear factor kappa B), it induces an addictive state.[76][77]
ΔJunD, a transcription factor, and G9a, a histone methyltransferase enzyme, both directly oppose the induction of ΔFosB in the nucleus accumbens (i.e., they oppose increases in its expression).[70][80][86] Sufficiently overexpressing ΔJunD in the nucleus accumbens with viral vectors can completely block many of the neural and behavioral alterations seen in chronic drug use (i.e., the alterations mediated by ΔFosB).[80] ΔFosB also plays an important role in regulating behavioral responses to natural rewards, such as palatable food, sex, and exercise.[80][83][87] Since both natural rewards and addictive drugs induce expression of ΔFosB (i.e., they cause the brain to produce more of it), chronic acquisition of these rewards can result in a similar pathological state of addiction.[80][83] ΔFosB is the most significant factor involved in both amphetamine addiction and amphetamine-induced sex addictions, which are compulsive sexual behaviors that result from excessive sexual activity and amphetamine use.[note 7][83][88] These sex addictions (i.e., drug-induced compulsive sexual behaviors) are associated with a dopamine dysregulation syndrome which occurs in some patients taking dopaminergic drugs, such as amphetamine or methamphetamine.[83][87][88]
Epigenetic factors
Methamphetamine addiction is persistent for many individuals, with 61% of individuals treated for addiction relapsing within one year.[89] About half of those with methamphetamine addiction continue with use over a ten-year period, while the other half reduce use starting at about one to four years after initial use.[90]
The frequent persistence of addiction suggests that long-lasting changes in gene expression may occur in particular regions of the brain, and may contribute importantly to the addiction phenotype. In 2014, a crucial role was found for epigenetic mechanisms in driving lasting changes in gene expression in the brain.[86]
In methamphetamine addicted rats, epigenetic regulation through reduced acetylation of histones, in brain striatal neurons, caused reduced transcription of glutamate receptors.[93] Glutamate receptors play an important role in regulating the reinforcing effects of addictive drugs.[94]
Administration of methamphetamine to rodents causes DNA damage in their brain, particularly in the nucleus accumbens region.[95][96] During repair of such DNA damages, persistent chromatin alterations may occur such as in the methylation of DNA or the acetylation or methylation of histones at the sites of repair.[97] These alterations can be epigenetic scars in the chromatin that contribute to the persistent epigenetic changes found in methamphetamine addiction.
Medication-Assisted Treatment (MAT) combines FDA-approved medications with behavioral therapies to address substance use disorders. This approach aims to reduce cravings and withdrawal symptoms, supporting individuals in their recovery process.[103]
Dependence and withdrawal
Tolerance is expected to develop with regular methamphetamine use and, when used recreationally, this tolerance develops rapidly.[104][105] In dependent users, withdrawal symptoms are positively correlated with the level of drug tolerance.[106]Depression from methamphetamine withdrawal lasts longer and is more severe than that of cocaine withdrawal.[107]
According to the current Cochrane review on drug dependence and withdrawal in recreational users of methamphetamine, "when chronic heavy users abruptly discontinue [methamphetamine] use, many report a time-limited withdrawal syndrome that occurs within 24hours of their last dose".[106] Withdrawal symptoms in chronic, high-dose users are frequent, occurring in up to 87.6% of cases, and persist for three to four weeks with a marked "crash" phase occurring during the first week.[106] Methamphetamine withdrawal symptoms can include anxiety, drug craving, dysphoric mood, fatigue, increased appetite, increased movement or decreased movement, lack of motivation, sleeplessness or sleepiness, and vivid or lucid dreams.[106]
Methamphetamine that is present in a mother's bloodstream can pass through the placenta to a fetus and be secreted into breast milk.[107] Infants born to methamphetamine-abusing mothers may experience a neonatal withdrawal syndrome, with symptoms involving of abnormal sleep patterns, poor feeding, tremors, and hypertonia.[107] This withdrawal syndrome is relatively mild and only requires medical intervention in approximately4% of cases.[107]
Unlike other drugs, babies with prenatal exposure to methamphetamine do not show immediate signs of withdrawal. Instead, cognitive and behavioral problems start emerging when the children reach school age.[108]
A prospective cohort study of 330 children showed that at the age of 3, children with methamphetamine exposure showed increased emotional reactivity, as well as more signs of anxiety and depression; and at the age of 5, children showed higher rates of externalizing disorders and attention deficit hyperactivity disorder (ADHD).[109]
Use of methamphetamine can result in a stimulant psychosis which may present with a variety of symptoms (e.g., paranoia, hallucinations, delirium, and delusions).[5][114] A Cochrane Collaboration review on treatment for amphetamine, dextroamphetamine, and methamphetamine use-induced psychosis states that about5–15% of users fail to recover completely.[114][115] The same review asserts that, based upon at least one trial, antipsychotic medications effectively resolve the symptoms of acute amphetamine psychosis.[114] Amphetamine psychosis may also develop occasionally as a treatment-emergent side effect.[116]
Death from overdose
The CDC reported that the number of deaths in the United States involving psychostimulants with abuse potential to be 23,837 in 2020 and 32,537 in 2021.[117] This category code (ICD–10 of T43.6) includes primarily methamphetamine but also other stimulants such as amphetamine, and methylphenidate. The mechanism of death in these cases is not reported in these statistics and is difficult to know.[118] Unlike fentanyl which causes respiratory depression, methamphetamine is not a respiratory depressant. Some deaths are as a result of intracranial hemorrhage[119] and some deaths are cardiovascular in nature including flash pulmonary edema[120] and ventricular fibrillation.[121][122]
Emergency treatment
Acute methamphetamine intoxication is largely managed by treating the symptoms and treatments may initially include administration of activated charcoal and sedation.[5] There is not enough evidence on hemodialysis or peritoneal dialysis in cases of methamphetamine intoxication to determine their usefulness.[27]Forced acid diuresis (e.g., with vitamin C) will increase methamphetamine excretion but is not recommended as it may increase the risk of aggravating acidosis, or cause seizures or rhabdomyolysis.[5] Hypertension presents a risk for intracranial hemorrhage (i.e., bleeding in the brain) and, if severe, is typically treated with intravenous phentolamine or nitroprusside.[5] Blood pressure often drops gradually following sufficient sedation with a benzodiazepine and providing a calming environment.[5]
Antipsychotics such as haloperidol are useful in treating agitation and psychosis from methamphetamine overdose.[123][124]Beta blockers with lipophilic properties and CNS penetration such as metoprolol and labetalol may be useful for treating CNS and cardiovascular toxicity.[125][126] The mixed alpha- and beta-blocker labetalol is especially useful for treatment of concomitant tachycardia and hypertension induced by methamphetamine.[123] The phenomenon of "unopposed alpha stimulation" has not been reported with the use of beta-blockers for treatment of methamphetamine toxicity.[123]
Interactions
Methamphetamine is metabolized by the liver enzyme CYP2D6, so CYP2D6 inhibitors will prolong the elimination half-life of methamphetamine.[27][127] Methamphetamine also interacts with monoamine oxidase inhibitors (MAOIs), since both MAOIs and methamphetamine increase plasma catecholamines; therefore, concurrent use of both is dangerous.[27] Methamphetamine may decrease the effects of sedatives and depressants and increase the effects of antidepressants and other stimulants as well.[27] Methamphetamine may counteract the effects of antihypertensives and antipsychotics owing to its effects on the cardiovascular system and cognition respectively.[27] The pH of gastrointestinal content and urine affects the absorption and excretion of methamphetamine.[27] Specifically, acidic substances will reduce the absorption of methamphetamine and increase urinary excretion, while alkaline substances do the opposite.[27] Owing to the effect pH has on absorption, proton pump inhibitors, which reduce gastric acid, are known to interact with methamphetamine.[27]Norepinephrine reuptake inhibitors (NRIs) like atomoxetine prevent norepinephrine release induced by amphetamines and have been found to reduce the stimulant, euphoriant, and sympathomimetic effects of dextroamphetamine in humans.[128][129][130] Similarly, norepinephrine–dopamine reuptake inhibitors (NRIs) like methylphenidate and bupropion prevent norepinephrine and dopamine release induced by amphetamines and bupropion has been found to reduce the subjective and sympathomimetic effects of methamphetamine in humans.[131][129][132][133]
Pharmacology
Pharmacodynamics
Monoamine release of methamphetamine and related agents (EC50Tooltip Half maximal effective concentration, nM)
This illustration depicts the normal operation of the dopaminergic terminal to the left, and the dopaminergic terminal in the presence of methamphetamine to the right. Methamphetamine reverses the action of the dopamine transporter (DAT) by activating TAAR1 (not shown). TAAR1 activation also causes some of the dopamine transporters to move into the presynaptic neuron and cease transport (not shown). At VMAT2 (labeled VMAT), methamphetamine causes dopamine efflux (release).
In addition to its effect on the plasma membrane monoamine transporters, methamphetamine inhibits synaptic vesicle function by inhibiting VMAT2, which prevents monoamine uptake into the vesicles and promotes their release.[154] Methamphetamine binds to VMAT2 via the resperine site, in contrast to amphetamine, which appears to bind at the tetrabenazine site.[155] This results in the outflow of monoamines from synaptic vesicles into the cytosol (intracellular fluid) of the presynaptic neuron, and their subsequent release into the synaptic cleft by the phosphorylated transporters.[156] Other transporters that methamphetamine is known to inhibit are SLC22A3 and SLC22A5.[154] SLC22A3 is an extraneuronal monoamine transporter that is present in astrocytes, and SLC22A5 is a high-affinity carnitine transporter.[145][157]
The bioavailability of methamphetamine is 67% orally, 79% intranasally, 67 to 90% via inhalation (smoking), and 100% intravenously.[4][5][6] Following oral administration, methamphetamine is well-absorbed into the bloodstream, with peak plasma methamphetamine concentrations achieved in approximately 3.13–6.3hours post ingestion.[161] Methamphetamine is also well absorbed following inhalation and following intranasal administration.[5] Because of the high lipophilicity of methamphetamine due to its methyl group, it can readily move through the blood–brain barrier faster than other stimulants, where it is more resistant to degradation by monoamine oxidase.[5][161][162] The amphetamine metabolite peaks at 10–24hours.[5] Methamphetamine is excreted by the kidneys, with the rate of excretion into the urine heavily influenced by urinary pH.[27][161] When taken orally, 30–54% of the dose is excreted in urine as methamphetamine and 10–23% as amphetamine.[161] Following IV doses, about45% is excreted as methamphetamine and 7% as amphetamine.[161] The elimination half-life of methamphetamine varies with a range of 5–30hours, but it is on average 9 to 12hours in most studies.[5][4] The elimination half-life of methamphetamine does not vary by route of administration, but is subject to substantial interindividual variability.[4]
The main metabolic pathways involve aromatic para-hydroxylation, aliphatic alpha- and beta-hydroxylation, N-oxidation, N-dealkylation, and deamination.[10][161][172] The known metabolic pathways include:
Metabolic pathways of methamphetamine in humans[sources 2]
The primary metabolites of methamphetamine are amphetamine and 4-hydroxymethamphetamine.[161]Human microbiota, particularly Lactobacillus, Enterococcus, and Clostridium species, contribute to the metabolism of methamphetamine via an enzyme which N-demethylates methamphetamine and 4-hydroxymethamphetamine into amphetamine and 4-hydroxyamphetamine respectively.[173][174]
Detection in biological fluids
Methamphetamine and amphetamine are often measured in urine or blood as part of a drug test for sports, employment, poisoning diagnostics, and forensics.[175][176][177][178] Chiral techniques may be employed to help distinguish the source of the drug to determine whether it was obtained illicitly or legally via prescription or prodrug.[179] Chiral separation is needed to assess the possible contribution of levomethamphetamine, which is an active ingredients in some OTC nasal decongestants,[note 4] toward a positive test result.[179][180][181] Dietary zinc supplements can mask the presence of methamphetamine and other drugs in urine.[182]
Chemistry
Shards of pure methamphetamine hydrochloride, also known as crystal meth
In contrast, the methamphetamine hydrochloride salt is odorless with a bitter taste.[14] It has a melting point between 170 and 175°C (338 and 347°F) and, at room temperature, occurs as white crystals or a white crystalline powder.[14] The hydrochloride salt is also freely soluble in ethanol and water.[14] The crystal structure of either enantiomer is monoclinic with P21space group; at 90K (−183.2°C; −297.7°F), it has lattice parametersa = 7.10Å, b = 7.29Å, c = 10.81Å, and β = 97.29°.[183]
Degradation
A 2011 study into the destruction of methamphetamine using bleach showed that effectiveness is correlated with exposure time and concentration.[184] A year-long study (also from 2011) showed that methamphetamine in soils is a persistent pollutant.[185] In a 2013 study of bioreactors in wastewater, methamphetamine was found to be largely degraded within 30days under exposure to light.[186]
Racemic methamphetamine may be prepared starting from phenylacetone by either the Leuckart[187] or reductive amination methods.[188] In the Leuckart reaction, one equivalent of phenylacetone is reacted with two equivalents of N-methylformamide to produce the formyl amide of methamphetamine plus carbon dioxide and methylamine as side products.[188] In this reaction, an iminium cation is formed as an intermediate which is reduced by the second equivalent of N-methylformamide.[188] The intermediate formyl amide is then hydrolyzed under acidic aqueous conditions to yield methamphetamine as the final product.[188] Alternatively, phenylacetone can be reacted with methylamine under reducing conditions to yield methamphetamine.[188]
Methamphetamine synthesis
Method of methamphetamine synthesis of methamphetamine via reductive amination
Pervitin, a methamphetamine brand used by German soldiers during World War II, was dispensed in various forms, including tablet containers.U.S. drug overdose related fatalities in 2017 were 70,200, including 10,333 of those related to psychostimulants (including methamphetamine).
Amphetamine, discovered before methamphetamine, was first synthesized in 1887 in Germany by Romanian chemist Lazăr Edeleanu who named it phenylisopropylamine.[191][192] Shortly after, methamphetamine was synthesized from ephedrine in 1893 by Japanese chemistNagai Nagayoshi.[193] Three decades later, in 1919, methamphetamine hydrochloride was synthesized by pharmacologist Akira Ogata via reduction of ephedrine using red phosphorus and iodine.[194]
From 1938, methamphetamine was marketed on a large scale in Germany as a nonprescription drug under the brand name Pervitin, produced by the Berlin-based Temmler pharmaceutical company.[195][196] It was used by all branches of the combined armed forces of the Third Reich, for its stimulant effects and to induce extended wakefulness.[197][198] Pervitin became colloquially known among the German troops as "Stuka-Tablets" (Stuka-Tabletten) and "Herman-Göring-Pills" (Hermann-Göring-Pillen), as a snide allusion to Göring's widely-known addiction to drugs. However, the side effects, particularly the withdrawal symptoms, were so serious that the army sharply cut back its usage in 1940.[199] By 1941, usage was restricted to a doctor's prescription, and the military tightly controlled its distribution. Soldiers would only receive a couple of tablets at a time, and were discouraged from using them in combat. Historian Łukasz Kamieński says,
A soldier going to battle on Pervitin usually found himself unable to perform effectively for the next day or two. Suffering from a drug hangover and looking more like a zombie than a great warrior, he had to recover from the side effects.
Some soldiers turned violent, committing war crimes against civilians; others attacked their own officers.[199] At the end of the war, it was used as part of a new drug: D-IX.
Obetrol, patented by Obetrol Pharmaceuticals in the 1950s and indicated for treatment of obesity, was one of the first brands of pharmaceutical methamphetamine products.[200] Because of the psychological and stimulant effects of methamphetamine, Obetrol became a popular diet pill in the United States in the 1950s and 1960s.[200] Eventually, as the addictive properties of the drug became known, governments began to strictly regulate the production and distribution of methamphetamine.[192] For example, during the early 1970s in the United States, methamphetamine became a schedule II controlled substance under the Controlled Substances Act.[3] As of January 2013, the Desoxyn trademark had been sold to Italian pharmaceutical company Recordati.[201]
Trafficking
The Golden Triangle (Southeast Asia), specifically Shan State, Myanmar, is the world's leading producer of methamphetamine as production has shifted to ya ba and crystalline methamphetamine, including for export to the United States and across East and Southeast Asia and the Pacific.[202]
Concerning the accelerating synthetic drug production in the region, the Cantonese Chinese syndicate Sam Gor, also known as The Company, is understood to be the main international crime syndicate responsible for this shift.[203] It is made up of members of five different triads. Sam Gor is primarily involved in drug trafficking, earning at least $8 billion per year.[204] Sam Gor is alleged to control 40% of the Asia-Pacific methamphetamine market, while also trafficking heroin and ketamine. The organization is active in a variety of countries, including Myanmar, Thailand, New Zealand, Australia, Japan, China, and Taiwan. Sam Gor previously produced meth in Southern China and is now believed to manufacture mainly in the Golden Triangle, specifically Shan State, Myanmar, responsible for much of the massive surge of crystal meth in circa 2019.[205] The group is understood to be headed by Tse Chi Lop, a gangster born in Guangzhou, China who also holds a Canadian passport.
Liu Zhaohua was another individual involved in the production and trafficking of methamphetamine until his arrest in 2005.[206] It was estimated over 18 tonnes of methamphetamine were produced under his watch.[206]
The production, distribution, sale, and possession of methamphetamine is restricted or illegal in many jurisdictions.[207][208] In some jurisdictions, it is legally available as a prescription medication. Methamphetamine has been placed in schedule II of the United NationsConvention on Psychotropic Substances treaty, indicating that it has limited medical use.[208]
Research
Animal models have shown that low-dose methamphetamine improves cognitive and behavioural functioning following TBI (traumatic brain injury).[7] This is in contrast to high, repeated doses which cause neurotoxicity. These models demonstrate that low-dose methamphetamine increases neurogenesis and reduces apoptosis in the dentate gyrus of the hippocampus following TBI.[209] It has also been found that TBI patients testing positive for methamphetamine at the time of emergency department admission have lower rates of mortality.[210]
It has been suggested, based on animal research, that calcitriol, the active metabolite of vitamin D, can provide significant protection against the DA- and 5-HT-depleting effects of neurotoxic doses of methamphetamine.[211] Protection against methamphetamine-induced neurotoxicity has also been observed following administration of ascorbic acid (vitamin C),[212] cobalamin (vitamin B12),[213] and vitamin E.[214]
↑Methamphetamine is contracted from N-methylamphetamine. Synonyms and alternate spellings include: N-methylamphetamine, desoxyephedrine, Syndrox, Methedrine, and Desoxyn.[15][16][17] Common slang names for methamphetamine include: meth, speed, crank, and shabu (also sabu and shabu-shabu) in Indonesia and the Philippines,[18][19][20][21] and for the hydrochloride crystal, crystal meth, glass, shards, and ice,[22]Tina,[23] and, in New Zealand, P.[24]
↑Enantiomers are molecules that are mirror images of one another; they are structurally identical, but of the opposite orientation. Levomethamphetamine and dextromethamphetamine are also known as L-methamphetamine, (R)-methamphetamine, or levmetamfetamine (International Nonproprietary Name [INN]) and D-methamphetamine, (S)-methamphetamine, or metamfetamine (INN), respectively.[15][26]
12The medication package insert for Desoxyn lists the chemical name (S)-N,α-dimethylbenzeneethanamine hydrochloride, which explicitly identifies the compound as dextromethamphetamine (the S-enantiomer) with no stereochemical ambiguity.[27]
123The active ingredient in some OTC inhalers in the United States is listed as levmetamfetamine, the INN and USAN of levomethamphetamine.[29][30]
↑Transcription factors are proteins that increase or decrease the expression of specific genes.[81]
↑In simpler terms, this necessary and sufficient relationship means that ΔFosB overexpression in the nucleus accumbens and addiction-related behavioral and neural adaptations always occur together and never occur alone.
↑The associated research only involved amphetamine, not methamphetamine; however, this statement is included here due to the similarity between the pharmacodynamics and aphrodisiac effects of amphetamine and methamphetamine.
↑"Methamphetamine: Toxicity". PubChem Compound. National Center for Biotechnology Information. Archived from the original on 4 January 2015. Retrieved 4 January 2015.
12Sellers EM, Tyndale RF (2000). "Mimicking gene defects to treat drug dependence". Ann. N. Y. Acad. Sci. 909 (1): 233–246. Bibcode:2000NYASA.909..233S. doi:10.1111/j.1749-6632.2000.tb06685.x. PMID10911933. Methamphetamine, a central nervous system stimulant drug, is p-hydroxylated by CYP2D6 to less active p-OH-methamphetamine.
1234"Adderall XR Prescribing Information"(PDF). United States Food and Drug Administration. Shire US Inc. December 2013. pp.12–13. Archived(PDF) from the original on 30 December 2013. Retrieved 30 December 2013.
12Cashman JR, Xiong YN, Xu L, Janowsky A (March 1999). "N-oxygenation of amphetamine and methamphetamine by the human flavin-containing monooxygenase (form 3): role in bioactivation and detoxication". J. Pharmacol. Exp. Ther. 288 (3): 1251–1260. doi:10.1016/S0022-3565(24)38081-4. PMID10027866.
12"Methamphetamine". Drug profiles. European Monitoring Centre for Drugs and Drug Addiction (EMCDDA). 8 January 2015. Archived from the original on 15 April 2016. Retrieved 27 November 2018. The term metamfetamine (the International Non-Proprietary Name: INN) strictly relates to the specific enantiomer (S)-N,α-dimethylbenzeneethanamine.
12345678Moszczynska A, Callan SP (September 2017). "Molecular, Behavioral, and Physiological Consequences of Methamphetamine Neurotoxicity: Implications for Treatment". The Journal of Pharmacology and Experimental Therapeutics. 362 (3): 474–488. doi:10.1124/jpet.116.238501. PMC11047030. PMID28630283. METH is a schedule II drug, which can only be prescribed for attention deficit hyperactivity disorder (ADHD), extreme obesity, or narcolepsy (as Desoxyn; Recordati Rare Diseases LLC, Lebanon, NJ), with amphetamine being prescribed more often for these conditions due to amphetamine having lower reinforcing potential than METH (Lile et al., 2013).... As discussed earlier, the d-enantiomer has stronger CNS effects but is metabolized more quickly than the l-enantiomer, which is longer lasting due to the slower breakdown.... l-METH, a vasoconstrictor, is the active constituent of the Vicks Inhaler decongestant (Procter & Gamble, Cincinnati, OH), an over-the-counter product containing about 50 mg of the drug (Smith et al., 2014). Desoxyn, which is d-METH, is rarely medically prescribed due to its strong reinforcing properties. Therapeutic doses of Desoxyn are 20–25 mg daily, taken every 12 hours, with dosing not exceeding 60 mg/day
↑"Levomethamphetamine". Pubchem Compound. National Center for Biotechnology Information. Archived from the original on 6 October 2014. Retrieved 27 November 2018.
12Hart CL, Marvin CB, Silver R, Smith EE (February 2012). "Is cognitive functioning impaired in methamphetamine users? A critical review". Neuropsychopharmacology. 37 (3): 586–608. doi:10.1038/npp.2011.276. PMC3260986. PMID22089317. There are several amphetamines used recreationally, including d-amphetamine, methamphetamine, 3,4-methylenedioxyamphetamine, and 3,4-methylenedioxymethamphetamine. Of these compounds, methamphetamine has generated the greatest amount of concern. Indeed, periodically there are statements in the scientific and popular literature attesting to methamphetamine's greater potency and 'addictive' potential, relative to other amphetamines. Such statements, however, are inconsistent with data collected in humans, which show that d-amphetamine and methamphetamine produce nearly identical physiological and behavioral effects (eg, Martin et al, 1971; Sevak et al, 2009; Kirkpatrick et al, in press a).
12345678Krasnova IN, Cadet JL (May 2009). "Methamphetamine toxicity and messengers of death". Brain Res. Rev. 60 (2): 379–407. doi:10.1016/j.brainresrev.2009.03.002. PMC2731235. PMID19328213. Neuroimaging studies have revealed that METH can indeed cause neurodegenerative changes in the brains of human addicts (Aron and Paulus, 2007; Chang et al., 2007). These abnormalities include persistent decreases in the levels of dopamine transporters (DAT) in the orbitofrontal cortex, dorsolateral prefrontal cortex, and the caudate-putamen (McCann et al., 1998, 2008; Sekine et al., 2003; Volkow et al., 2001a, 2001c). The density of serotonin transporters (5-HTT) is also decreased in the midbrain, caudate, putamen, hypothalamus, thalamus, the orbitofrontal, temporal, and cingulate cortices of METH-dependent individuals (Sekine et al., 2006)... Neuropsychological studies have detected deficits in attention, working memory, and decision-making in chronic METH addicts... There is compelling evidence that the negative neuropsychiatric consequences of METH abuse are due, at least in part, to drug-induced neuropathological changes in the brains of these METH-exposed individuals... Structural magnetic resonance imaging (MRI) studies in METH addicts have revealed substantial morphological changes in their brains. These include loss of gray matter in the cingulate, limbic and paralimbic cortices, significant shrinkage of hippocampi, and hypertrophy of white matter (Thompson et al., 2004). In addition, the brains of METH abusers show evidence of hyperintensities in white matter (Bae et al., 2006; Ernst et al., 2000), decreases in the neuronal marker, N-acetylaspartate (Ernst et al., 2000; Sung et al., 2007), reductions in a marker of metabolic integrity, creatine (Sekine et al., 2002) and increases in a marker of glial activation, myoinositol (Chang et al., 2002; Ernst et al., 2000; Sung et al., 2007; Yen et al., 1994). Elevated choline levels, which are indicative of increased cellular membrane synthesis and turnover are also evident in the frontal gray matter of METH abusers (Ernst et al., 2000; Salo et al., 2007; Taylor et al., 2007).
↑Rolles S, Measham F (July 2011). "Questioning the method and utility of ranking drug harms in drug policy". The International Journal on Drug Policy. 22 (4): 243–246. doi:10.1016/j.drugpo.2011.04.004. PMID21652195.
↑Caulkins JP, Reuter P, Coulson C (November 2011). "Basing drug scheduling decisions on scientific ranking of harmfulness: false promise from false premises". Addiction. 106 (11): 1886–1890. doi:10.1111/j.1360-0443.2011.03461.x. PMID21895823.
1234Westfall DP, Westfall TC (2010). "Miscellaneous Sympathomimetic Agonists". In Brunton LL, Chabner BA, Knollmann BC (eds.). Goodman & Gilman's Pharmacological Basis of Therapeutics (12thed.). New York: McGraw-Hill. ISBN978-0-07-162442-8. Archived from the original on 10 November 2013. Retrieved 1 January 2014.
12Elkins C (27 February 2020). "Meth Sores". DrugRehab.com. Advanced Recovery Systems. Archived from the original on 14 August 2020. Retrieved 15 March 2020.
↑National Institute on Drug Abuse (29 January 2021). "Overdose Death Rates". National Institute on Drug Abuse. Archived from the original on 25 January 2018. Retrieved 8 October 2020.
123Hussain F, Frare RW, Py Berrios KL (2012). "Drug abuse identification and pain management in dental patients: a case study and literature review". Gen. Dent. 60 (4): 334–345. PMID22782046.
12O'Connor PG (February 2012). "Amphetamines". Merck Manual for Health Care Professionals. Merck. Archived from the original on 6 May 2012. Retrieved 8 May 2012.
12Beardsley PM, Hauser KF (2014). "Glial Modulators as Potential Treatments of Psychostimulant Abuse". Emerging Targets & Therapeutics in the Treatment of Psychostimulant Abuse. Advances in Pharmacology. Vol.69. Academic Press. pp.1–69. doi:10.1016/B978-0-12-420118-7.00001-9. ISBN978-0-12-420118-7. PMC4103010. PMID24484974. Glia (including astrocytes, microglia, and oligodendrocytes), which constitute the majority of cells in the brain, have many of the same receptors as neurons, secrete neurotransmitters and neurotrophic and neuroinflammatory factors, control clearance of neurotransmitters from synaptic clefts, and are intimately involved in synaptic plasticity. Despite their prevalence and spectrum of functions, appreciation of their potential general importance has been elusive since their identification in the mid-1800s, and only relatively recently have they been gaining their due respect. This development of appreciation has been nurtured by the growing awareness that drugs of abuse, including the psychostimulants, affect glial activity, and glial activity, in turn, has been found to modulate the effects of the psychostimulants
↑>See Fig. 7.1 in Loftis JM, Janowsky A (2014). "Neuroimmune basis of methamphetamine toxicity". Neuroimmune Signaling in Drug Actions and Addictions. International Review of Neurobiology. Vol.118. Academic Press. pp.165–197. doi:10.1016/B978-0-12-801284-0.00007-5. ISBN978-0-12-801284-0. PMC4418472. PMID25175865. Collectively, these pathological processes contribute to neurotoxicity (e.g., increased BBB permeability, inflammation, neuronal degeneration, cell death) and neuropsychiatric impairments (e.g., cognitive eficits, mood disorders)
12345Kaushal N, Matsumoto RR (March 2011). "Role of sigma receptors in methamphetamine-induced neurotoxicity". Curr Neuropharmacol. 9 (1): 54–57. doi:10.2174/157015911795016930. PMC3137201. PMID21886562. σ Receptors seem to play an important role in many of the effects of METH. They are present in the organs that mediate the actions of METH (e.g. brain, heart, lungs) [5]. In the brain, METH acts primarily on the dopaminergic system to cause acute locomotor stimulant, subchronic sensitized, and neurotoxic effects. σ Receptors are present on dopaminergic neurons and their activation stimulates dopamine synthesis and release [11–13]. σ-2 Receptors modulate DAT and the release of dopamine via protein kinase C (PKC) and Ca2+-calmodulin systems [14]. σ-1 Receptor antisense and antagonists have been shown to block the acute locomotor stimulant effects of METH [4]. Repeated administration or self administration of METH has been shown to upregulate σ-1 receptor protein and mRNA in various brain regions including the substantia nigra, frontal cortex, cerebellum, midbrain, and hippocampus [15, 16]. Additionally, σ receptor antagonists... prevent the development of behavioral sensitization to METH [17, 18].... σ Receptor agonists have been shown to facilitate dopamine release, through both σ-1 and σ-2 receptors [11–14].
↑Yuan J, Hatzidimitriou G, Suthar P, Mueller M, McCann U, Ricaurte G (March 2006). "Relationship between temperature, dopaminergic neurotoxicity, and plasma drug concentrations in methamphetamine-treated squirrel monkeys". The Journal of Pharmacology and Experimental Therapeutics. 316 (3): 1210–1218. doi:10.1124/jpet.105.096503. PMID16293712.
1234Rodvelt KR, Miller DK (September 2010). "Could sigma receptor ligands be a treatment for methamphetamine addiction?". Curr Drug Abuse Rev. 3 (3): 156–162. doi:10.2174/1874473711003030156. PMID21054260.
↑Malenka RC, Nestler EJ, Hyman SE (2009). "Chapter 15: Reinforcement and Addictive Disorders". In Sydor A, Brown RY (eds.). Molecular Neuropharmacology: A Foundation for Clinical Neuroscience (2nded.). New York: McGraw-Hill Medical. pp.364–375. ISBN9780071481274.
1234Nestler EJ (December 2013). "Cellular basis of memory for addiction". Dialogues in Clinical Neuroscience. 15 (4): 431–443. PMC3898681. PMID24459410. Despite the importance of numerous psychosocial factors, at its core, drug addiction involves a biological process: the ability of repeated exposure to a drug of abuse to induce changes in a vulnerable brain that drive the compulsive seeking and taking of drugs, and loss of control over drug use, that define a state of addiction.... A large body of literature has demonstrated that such ΔFosB induction in D1-type [nucleus accumbens] neurons increases an animal's sensitivity to drug as well as natural rewards and promotes drug self-administration, presumably through a process of positive reinforcement... Another ΔFosB target is cFos: as ΔFosB accumulates with repeated drug exposure it represses c-Fos and contributes to the molecular switch whereby ΔFosB is selectively induced in the chronic drug-treated state.41.... Moreover, there is increasing evidence that, despite a range of genetic risks for addiction across the population, exposure to sufficiently high doses of a drug for long periods of time can transform someone who has relatively lower genetic loading into an addict.
↑Volkow ND, Koob GF, McLellan AT (January 2016). "Neurobiologic Advances from the Brain Disease Model of Addiction". New England Journal of Medicine. 374 (4): 363–371. doi:10.1056/NEJMra1511480. PMC6135257. PMID26816013. Substance-use disorder: A diagnostic term in the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) referring to recurrent use of alcohol or other drugs that causes clinically and functionally significant impairment, such as health problems, disability, and failure to meet major responsibilities at work, school, or home. Depending on the level of severity, this disorder is classified as mild, moderate, or severe. Addiction: A term used to indicate the most severe, chronic stage of substance-use disorder, in which there is a substantial loss of self-control, as indicated by compulsive drug taking despite the desire to stop taking the drug. In the DSM-5, the term addiction is synonymous with the classification of severe substance-use disorder.
123Renthal W, Nestler EJ (September 2009). "Chromatin regulation in drug addiction and depression". Dialogues in Clinical Neuroscience. 11 (3): 257–268. doi:10.31887/DCNS.2009.11.3/wrenthal. PMC2834246. PMID19877494. [Psychostimulants] increase cAMP levels in striatum, which activates protein kinase A (PKA) and leads to phosphorylation of its targets. This includes the cAMP response element binding protein (CREB), the phosphorylation of which induces its association with the histone acetyltransferase, CREB binding protein (CBP) to acetylate histones and facilitate gene activation. This is known to occur on many genes including fosB and c-fos in response to psychostimulant exposure. ΔFosB is also upregulated by chronic psychostimulant treatments, and is known to activate certain genes (eg, cdk5) and repress others (eg, c-fos) where it recruits HDAC1 as a corepressor.... Chronic exposure to psychostimulants increases glutamatergic [signaling] from the prefrontal cortex to the NAc. Glutamatergic signaling elevates Ca2+ levels in NAc postsynaptic elements where it activates CaMK (calcium/calmodulin protein kinases) signaling, which, in addition to phosphorylating CREB, also phosphorylates HDAC5. Figure 2: Psychostimulant-induced signaling events
↑Broussard JI (January 2012). "Co-transmission of dopamine and glutamate". The Journal of General Physiology. 139 (1): 93–96. doi:10.1085/jgp.201110659. PMC3250102. PMID22200950. Coincident and convergent input often induces plasticity on a postsynaptic neuron. The NAc integrates processed information about the environment from basolateral amygdala, hippocampus, and prefrontal cortex (PFC), as well as projections from midbrain dopamine neurons. Previous studies have demonstrated how dopamine modulates this integrative process. For example, high frequency stimulation potentiates hippocampal inputs to the NAc while simultaneously depressing PFC synapses (Goto and Grace, 2005). The converse was also shown to be true; stimulation at PFC potentiates PFC–NAc synapses but depresses hippocampal–NAc synapses. In light of the new functional evidence of midbrain dopamine/glutamate co-transmission (references above), new experiments of NAc function will have to test whether midbrain glutamatergic inputs bias or filter either limbic or cortical inputs to guide goal-directed behavior.
↑Kanehisa Laboratories (10 October 2014). "Amphetamine – Homo sapiens (human)". KEGG Pathway. Retrieved 31 October 2014. Most addictive drugs increase extracellular concentrations of dopamine (DA) in nucleus accumbens (NAc) and medial prefrontal cortex (mPFC), projection areas of mesocorticolimbic DA neurons and key components of the "brain reward circuit". Amphetamine achieves this elevation in extracellular levels of DA by promoting efflux from synaptic terminals.... Chronic exposure to amphetamine induces a unique transcription factor delta FosB, which plays an essential role in long-term adaptive changes in the brain.
123Robison AJ, Nestler EJ (November 2011). "Transcriptional and epigenetic mechanisms of addiction". Nature Reviews Neuroscience. 12 (11): 623–637. doi:10.1038/nrn3111. PMC3272277. PMID21989194. ΔFosB serves as one of the master control proteins governing this structural plasticity.... ΔFosB also represses G9a expression, leading to reduced repressive histone methylation at the cdk5 gene. The net result is gene activation and increased CDK5 expression.... In contrast, ΔFosB binds to the c-fos gene and recruits several co-repressors, including HDAC1 (histone deacetylase 1) and SIRT 1 (sirtuin 1).... The net result is c-fos gene repression. Figure 4: Epigenetic basis of drug regulation of gene expression
123Nestler EJ (December 2012). "Transcriptional mechanisms of drug addiction". Clinical Psychopharmacology and Neuroscience. 10 (3): 136–143. doi:10.9758/cpn.2012.10.3.136. PMC3569166. PMID23430970. The 35-37 kD ΔFosB isoforms accumulate with chronic drug exposure due to their extraordinarily long half-lives.... As a result of its stability, the ΔFosB protein persists in neurons for at least several weeks after cessation of drug exposure.... ΔFosB overexpression in nucleus accumbens induces NFκB... In contrast, the ability of ΔFosB to repress the c-Fos gene occurs in concert with the recruitment of a histone deacetylase and presumably several other repressive proteins such as a repressive histone methyltransferase
↑Nestler EJ (October 2008). "Transcriptional mechanisms of addiction: Role of ΔFosB". Philosophical Transactions of the Royal Society B: Biological Sciences. 363 (1507): 3245–3255. doi:10.1098/rstb.2008.0067. PMC2607320. PMID18640924. Recent evidence has shown that ΔFosB also represses the c-fos gene that helps create the molecular switch—from the induction of several short-lived Fos family proteins after acute drug exposure to the predominant accumulation of ΔFosB after chronic drug exposure
↑Hyman SE, Malenka RC, Nestler EJ (July 2006). "Neural mechanisms of addiction: the role of reward-related learning and memory". Annu. Rev. Neurosci. 29: 565–598. doi:10.1146/annurev.neuro.29.051605.113009. PMID16776597.
12345678Robison AJ, Nestler EJ (November 2011). "Transcriptional and epigenetic mechanisms of addiction". Nat. Rev. Neurosci. 12 (11): 623–637. doi:10.1038/nrn3111. PMC3272277. PMID21989194. ΔFosB has been linked directly to several addiction-related behaviors... Importantly, genetic or viral overexpression of ΔJunD, a dominant-negative mutant of JunD which antagonizes ΔFosB- and other AP-1-mediated transcriptional activity, in the NAc or OFC blocks these key effects of drug exposure14,22–24. This indicates that ΔFosB is both necessary and sufficient for many of the changes wrought in the brain by chronic drug exposure. ΔFosB is also induced in D1-type NAc MSNs by chronic consumption of several natural rewards, including sucrose, high-fat food, sex, wheel running, where it promotes that consumption14,26–30. This implicates ΔFosB in the regulation of natural rewards under normal conditions and perhaps during pathological addictive-like states.
↑Malenka RC, Nestler EJ, Hyman SE (2009). "Chapter 4: Signal Transduction in the Brain". In Sydor A, Brown RY (eds.). Molecular Neuropharmacology: A Foundation for Clinical Neuroscience (2nded.). New York, USA: McGraw-Hill Medical. p.94. ISBN978-0-07-148127-4.
123Ruffle JK (November 2014). "Molecular neurobiology of addiction: what's all the (Δ)FosB about?". Am. J. Drug Alcohol Abuse. 40 (6): 428–437. doi:10.3109/00952990.2014.933840. PMID25083822. ΔFosB is an essential transcription factor implicated in the molecular and behavioral pathways of addiction following repeated drug exposure.
123456789101112131415161718Olsen CM (December 2011). "Natural rewards, neuroplasticity, and non-drug addictions". Neuropharmacology. 61 (7): 1109–1122. doi:10.1016/j.neuropharm.2011.03.010. PMC3139704. PMID21459101. Similar to environmental enrichment, studies have found that exercise reduces self-administration and relapse to drugs of abuse (Cosgrove et al., 2002; Zlebnik et al., 2010). There is also some evidence that these preclinical findings translate to human populations, as exercise reduces withdrawal symptoms and relapse in abstinent smokers (Daniel et al., 2006; Prochaska et al., 2008), and one drug recovery program has seen success in participants that train for and compete in a marathon as part of the program (Butler, 2005).... In humans, the role of dopamine signaling in incentive-sensitization processes has recently been highlighted by the observation of a dopamine dysregulation syndrome in some patients taking dopaminergic drugs. This syndrome is characterized by a medication-induced increase in (or compulsive) engagement in non-drug rewards such as gambling, shopping, or sex (Evans et al., 2006; Aiken, 2007; Lader, 2008).
12Blum K, Werner T, Carnes S, Carnes P, Bowirrat A, Giordano J, etal. (March 2012). "Sex, drugs, and rock 'n' roll: hypothesizing common mesolimbic activation as a function of reward gene polymorphisms". Journal of Psychoactive Drugs. 44 (1): 38–55. doi:10.1080/02791072.2012.662112. PMC4040958. PMID22641964. It has been found that deltaFosB gene in the NAc is critical for reinforcing effects of sexual reward. Pitchers and colleagues (2010) reported that sexual experience was shown to cause DeltaFosB accumulation in several limbic brain regions including the NAc, medial pre-frontal cortex, VTA, caudate, and putamen, but not the medial preoptic nucleus.... these findings support a critical role for DeltaFosB expression in the NAc in the reinforcing effects of sexual behavior and sexual experience-induced facilitation of sexual performance.... both drug addiction and sexual addiction represent pathological forms of neuroplasticity along with the emergence of aberrant behaviors involving a cascade of neurochemical changes mainly in the brain's rewarding circuitry.
12Pitchers KK, Vialou V, Nestler EJ, Laviolette SR, Lehman MN, Coolen LM (February 2013). "Natural and drug rewards act on common neural plasticity mechanisms with ΔFosB as a key mediator". J. Neurosci. 33 (8): 3434–3442. doi:10.1523/JNEUROSCI.4881-12.2013. PMC3865508. PMID23426671. Drugs of abuse induce neuroplasticity in the natural reward pathway, specifically the nucleus accumbens (NAc), thereby causing development and expression of addictive behavior.... Together, these findings demonstrate that drugs of abuse and natural reward behaviors act on common molecular and cellular mechanisms of plasticity that control vulnerability to drug addiction, and that this increased vulnerability is mediated by ΔFosB and its downstream transcriptional targets.... Sexual behavior is highly rewarding (Tenk et al., 2009), and sexual experience causes sensitized drug-related behaviors, including cross-sensitization to amphetamine (Amph)-induced locomotor activity (Bradley and Meisel, 2001; Pitchers et al., 2010a) and enhanced Amph reward (Pitchers et al., 2010a). Moreover, sexual experience induces neural plasticity in the NAc similar to that induced by psychostimulant exposure, including increased dendritic spine density (Meisel and Mullins, 2006; Pitchers et al., 2010a), altered glutamate receptor trafficking, and decreased synaptic strength in prefrontal cortex-responding NAc shell neurons (Pitchers et al., 2012). Finally, periods of abstinence from sexual experience were found to be critical for enhanced Amph reward, NAc spinogenesis (Pitchers et al., 2010a), and glutamate receptor trafficking (Pitchers et al., 2012). These findings suggest that natural and drug reward experiences share common mechanisms of neural plasticity
↑Kenny PJ, Markou A (May 2004). "The ups and downs of addiction: role of metabotropic glutamate receptors". Trends Pharmacol. Sci. 25 (5): 265–72. doi:10.1016/j.tips.2004.03.009. PMID15120493.
↑Johnson Z, Venters J, Guarraci FA, Zewail-Foote M (June 2015). "Methamphetamine induces DNA damage in specific regions of the female rat brain". Clinical and Experimental Pharmacology & Physiology. 42 (6): 570–575. doi:10.1111/1440-1681.12404. PMID25867833.
1234Shoptaw SJ, Kao U, Heinzerling K, Ling W (2009). Shoptaw SJ (ed.). "Treatment for amphetamine withdrawal". Cochrane Database Syst. Rev. 2009 (2) CD003021. doi:10.1002/14651858.CD003021.pub2. PMC7138250. PMID19370579. The prevalence of this withdrawal syndrome is extremely common (Cantwell 1998; Gossop 1982) with 87.6% of 647 individuals with amphetamine dependence reporting six or more signs of amphetamine withdrawal listed in the DSM when the drug is not available (Schuckit 1999)... Withdrawal symptoms typically present within 24hours of the last use of amphetamine, with a withdrawal syndrome involving two general phases that can last 3 weeks or more. The first phase of this syndrome is the initial "crash" that resolves within about a week (Gossop 1982;McGregor 2005)
1234Winslow BT, Voorhees KI, Pehl KA (2007). "Methamphetamine abuse". American Family Physician. 76 (8): 1169–1174. PMID17990840.
↑Albertson TE (2011). "Amphetamines". In Olson KR, Anderson IB, Benowitz NL, Blanc PD, Kearney TE, Kim-Katz SY, Wu AH (eds.). Poisoning & Drug Overdose (6thed.). New York: McGraw-Hill Medical. pp.77–79. ISBN978-0-07-166833-0.
↑Oskie SM, Rhee JW (11 February 2011). "Amphetamine Poisoning". Emergency Central. Unbound Medicine. Archived from the original on 26 September 2013. Retrieved 11 June 2013.
↑Isbister GK, Buckley NA, Whyte IM (September 2007). "Serotonin toxicity: a practical approach to diagnosis and treatment". Med. J. Aust. 187 (6): 361–365. doi:10.5694/j.1326-5377.2007.tb01282.x. PMID17874986.
↑Malenka RC, Nestler EJ, Hyman SE, Holtzman DM (2015). "Chapter 16: Reinforcement and Addictive Disorders". Molecular Neuropharmacology: A Foundation for Clinical Neuroscience (3rded.). New York: McGraw-Hill Medical. ISBN978-0-07-182770-6. Unlike cocaine and amphetamine, methamphetamine is directly toxic at higher doses to midbrain dopamine neurons
123Shoptaw SJ, Kao U, Ling W (2009). Shoptaw SJ, Ali R (eds.). "Treatment for amphetamine psychosis". Cochrane Database Syst. Rev. 2009 (1) CD003026. doi:10.1002/14651858.CD003026.pub3. PMC7004251. PMID19160215. A minority of individuals who use amphetamines develop full-blown psychosis requiring care at emergency departments or psychiatric hospitals. In such cases, symptoms of amphetamine psychosis commonly include paranoid and persecutory delusions as well as auditory and visual hallucinations in the presence of extreme agitation. More common (about 18%) is for frequent amphetamine users to report psychotic symptoms that are sub-clinical and that do not require high-intensity intervention... About5–15% of the users who develop an amphetamine psychosis fail to recover completely (Hofmann 1983)... Findings from one trial indicate use of antipsychotic medications effectively resolves symptoms of acute amphetamine psychosis.
↑Paone S, Clarkson L, Sin B, Punnapuzha S (August 2018). "Recognition of Sympathetic Crashing Acute Pulmonary Edema (SCAPE) and use of high-dose nitroglycerin infusion". The American Journal of Emergency Medicine. 36 (8): 1526.e5–1526.e7. doi:10.1016/j.ajem.2018.05.013. PMID29776826.
↑De Letter EA, Piette MH, Lambert WE, Cordonnier JA (January 2006). "Amphetamines as potential inducers of fatalities: a review in the district of Ghent from 1976-2004". Medicine, Science, and the Law. 46 (1): 37–65. doi:10.1258/rsmmsl.46.1.37. PMID16454462.
123Richards JR, Albertson TE, Derlet RW, Lange RA, Olson KR, Horowitz BZ (May 2015). "Treatment of toxicity from amphetamines, related derivatives, and analogues: a systematic clinical review". Drug Alcohol Depend. 150: 1–13. doi:10.1016/j.drugalcdep.2015.01.040. PMID25724076.
↑Richards JR, Derlet RW, Duncan DR (September 1997). "Methamphetamine toxicity: treatment with a benzodiazepine versus a butyrophenone". Eur. J. Emerg. Med. 4 (3): 130–135. doi:10.1097/00063110-199709000-00003. PMID9426992.
↑Farzam K, Jan A (2025), "Beta Blockers", StatPearls, Treasure Island (FL): StatPearls Publishing, PMID30422501, retrieved 22 March 2025
12"Methamphetamine: Enzymes". DrugBank. University of Alberta. 8 February 2013. Archived from the original on 28 December 2015. Retrieved 2 January 2014.
12Heal DJ, Smith SL, Findling RL (2012). "ADHD: current and future therapeutics". Behavioral Neuroscience of Attention Deficit Hyperactivity Disorder and Its Treatment. Current Topics in Behavioral Neurosciences. Vol.9. pp.361–390. doi:10.1007/7854_2011_125. ISBN978-3-642-24611-1. PMID21487953. Adjunctive therapy with DL-methylphenidate in atomoxetine partial responders has been successful (Wilens et al. 2009), but this also increases the rates of insomnia, irritability and loss of appetite (Hammerness et al. 2009). This combination therapy has not included amphetamine because blockade of NET by atomoxetine prevents entry of amphetamine into presynaptic noradrenergic terminals (Sofuoglu et al. 2009).
↑Fitzgerald LR, Gannon BM, Walther D, Landavazo A, Hiranita T, Blough BE, etal. (March 2024). "Structure-activity relationships for locomotor stimulant effects and monoamine transporter interactions of substituted amphetamines and cathinones". Neuropharmacology. 245 109827. doi:10.1016/j.neuropharm.2023.109827. PMC10842458. PMID38154512. Although the number of amphetamine analogues with different amine substituents is relatively low in recreational drug markets (Cho and Segal, 1994), N-methyl and N-ethyl substitutions are sometimes found. Pharmacological activity of amphetamine-type drugs is decreased substantially if the N-alkyl chain is lengthened beyond ethyl, as previous studies show that N-propylamphetamine and N-butylamphetamine are ~4-fold and ~6-fold less potent than amphetamine in rats (Woolverton et al., 1980).
↑Nicole L (2022). In vivo Structure-Activity Relationships of Substituted Amphetamines and Substituted Cathinones (Ph.D. thesis). University of Arkansas for Medical Sciences. ProQuest2711781450. FIGURE 2-6: Release: Effects of the specified test drug on monoamine release by DAT (red circles), NET (blue squares), and SERT (black triangles) in rat brain tissue. [...] EC50 values determined for the drug indicated within the panel. [...]
123"Methamphetamine: Targets". DrugBank. University of Alberta. 8 February 2013. Archived from the original on 28 December 2015. Retrieved 4 January 2014.
↑Maguire JJ, Davenport AP (2 December 2014). "TA1 receptor". IUPHAR database. International Union of Basic and Clinical Pharmacology. Archived from the original on 29 June 2015. Retrieved 8 December 2014.
↑Vaughan RA, Foster JD (September 2013). "Mechanisms of dopamine transporter regulation in normal and disease states". Trends Pharmacol. Sci. 34 (9): 489–496. doi:10.1016/j.tips.2013.07.005. PMC3831354. PMID23968642. AMPH and METH also stimulate DA efflux, which is thought to be a crucial element in their addictive properties [80], although the mechanisms do not appear to be identical for each drug [81]. These processes are PKCβ– and CaMK–dependent [72, 82], and PKCβ knock-out mice display decreased AMPH-induced efflux that correlates with reduced AMPH-induced locomotion [72].
↑Ledonne A, Berretta N, Davoli A, Rizzo GR, Bernardi G, Mercuri NB (July 2011). "Electrophysiological effects of trace amines on mesencephalic dopaminergic neurons". Front. Syst. Neurosci. 5: 56. doi:10.3389/fnsys.2011.00056. PMC3131148. PMID21772817. inhibition of firing due to increased release of dopamine; (b) reduction of D2 and GABAB receptor-mediated inhibitory responses (excitatory effects due to disinhibition); and (c) a direct TA1 receptor-mediated activation of GIRK channels which produce cell membrane hyperpolarization.
↑mct (28 January 2012). "TAAR1". GenAtlas. University of Paris. Archived from the original on 29 May 2014. Retrieved 29 May 2014. • tonically activates inwardly rectifying K(+) channels, which reduces the basal firing frequency of dopamine (DA) neurons of the ventral tegmental area (VTA)
↑Sulzer D, Sonders MS, Poulsen NW, Galli A (April 2005). "Mechanisms of neurotransmitter release by amphetamines: a review". Progress in Neurobiology. 75 (6): 406–433. doi:10.1016/j.pneurobio.2005.04.003. PMID15955613. They also demonstrated competition for binding between METH and reserpine, suggesting they might bind to the same site on VMAT. George Uhl's laboratory similarly reported that AMPH displaced the VMAT2 blocker tetrabenazine (Gonzalez et al., 1994). Tetrabenazine and reserpine are thought to bind to different sites on VMAT (Schuldiner et al., 1993a)
↑Inazu M, Takeda H, Matsumiya T (August 2003). "[The role of glial monoamine transporters in the central nervous system]". Nihon Shinkei Seishin Yakurigaku Zasshi (in Japanese). 23 (4): 171–178. PMID13677912.
↑Melega WP, Cho AK, Schmitz D, Kuczenski R, Segal DS (February 1999). "l-methamphetamine pharmacokinetics and pharmacodynamics for assessment of in vivo deprenyl-derived l-methamphetamine". J. Pharmacol. Exp. Ther. 288 (2): 752–758. doi:10.1016/S0022-3565(24)38016-4. PMID9918585.
12Mendelson J, Uemura N, Harris D, Nath RP, Fernandez E, Jacob P, etal. (October 2006). "Human pharmacology of the methamphetamine stereoisomers". Clin. Pharmacol. Ther. 80 (4): 403–420. doi:10.1016/j.clpt.2006.06.013. PMID17015058.
1234567891011"Methamphetamine: Pharmacology". DrugBank. University of Alberta. 2 October 2017. Archived from the original on 6 October 2017. Retrieved 5 October 2017. Methamphetamine is rapidly absorbed from the gastrointestinal tract with peak methamphetamine concentrations occurring in 3.13 to 6.3 hours post ingestion. Methamphetamine is also well absorbed following inhalation and following intranasal administration. It is distributed to most parts of the body. Because methamphetamine has a high lipophilicity it is distributed across the blood brain barrier and crosses the placenta.... The primary site of metabolism is in the liver by aromatic hydroxylation, N-dealkylation and deamination. At least seven metabolites have been identified in the urine, with the main metabolites being amphetamine (active) and 4-hydroxymethamphetamine. Other minor metabolites include 4-hydroxyamphetamine, norephedrine, and 4-hydroxynorephedrine.
↑Xu J, Zhang Z, Liu R, Sun Y, Liu H, Nie Z, etal. (May 2019). "Function of complement factor H and imaging of small molecules by MALDI-MSI in a methamphetamine behavioral sensitization model". Behavioural Brain Research. 364: 233–244. doi:10.1016/j.bbr.2019.02.002. PMID30731099. Methamphetamine (METH) is a potent amphetamine-type stimulant that has high abuse potential and can be smoked, snorted, injected, or taken orally. The drug is high in lipid solubility and can cross the blood-brain barrier more readily than amphetamine due to the addition of an extra methyl group.
12Santagati NA, Ferrara G, Marrazzo A, Ronsisvalle G (September 2002). "Simultaneous determination of amphetamine and one of its metabolites by HPLC with electrochemical detection". J. Pharm. Biomed. Anal. 30 (2): 247–255. doi:10.1016/S0731-7085(02)00330-8. PMID12191709.
↑Glennon RA (2013). "Phenylisopropylamine stimulants: amphetamine-related agents". In Lemke TL, Williams DA, Roche VF, Zito W (eds.). Foye's principles of medicinal chemistry (7thed.). Philadelphia, USA: Wolters Kluwer Health/Lippincott Williams & Wilkins. pp.646–648. ISBN978-1-60913-345-0. Archived from the original on 13 January 2023. Retrieved 5 October 2017. The simplest unsubstituted phenylisopropylamine, 1-phenyl-2-aminopropane, or amphetamine, serves as a common structural template for hallucinogens and psychostimulants. Amphetamine produces central stimulant, anorectic, and sympathomimetic actions, and it is the prototype member of this class (39).... The phase 1 metabolism of amphetamine analogs is catalyzed by two systems: cytochrome P450 and flavin monooxygenase.... Amphetamine can also undergo aromatic hydroxylation to p-hydroxyamphetamine.... Subsequent oxidation at the benzylic position by DA β-hydroxylase affords p-hydroxynorephedrine. Alternatively, direct oxidation of amphetamine by DA β-hydroxylase can afford norephedrine.
↑Sjoerdsma A, von Studnitz W (April 1963). "Dopamine-beta-oxidase activity in man, using hydroxyamphetamine as substrate". Br. J. Pharmacol. Chemother. 20 (2): 278–284. doi:10.1111/j.1476-5381.1963.tb01467.x. PMC1703637. PMID13977820. Hydroxyamphetamine was administered orally to five human subjects... Since conversion of hydroxyamphetamine to hydroxynorephedrine occurs in vitro by the action of dopamine-β-oxidase, a simple method is suggested for measuring the activity of this enzyme and the effect of its inhibitors in man.... The lack of effect of administration of neomycin to one patient indicates that the hydroxylation occurs in body tissues.... a major portion of the β-hydroxylation of hydroxyamphetamine occurs in non-adrenal tissue. Unfortunately, at the present time one cannot be completely certain that the hydroxylation of hydroxyamphetamine in vivo is accomplished by the same enzyme which converts dopamine to noradrenaline.
↑"Amphetamine". Pubchem Compound. National Center for Biotechnology Information. Archived from the original on 13 October 2013. Retrieved 12 October 2013.
↑Caldwell J, Hawksworth GM (May 1973). "The demethylation of methamphetamine by intestinal microflora". The Journal of Pharmacy and Pharmacology. 25 (5): 422–424. doi:10.1111/j.2042-7158.1973.tb10043.x. PMID4146404.
↑Kraemer T, Maurer HH (August 1998). "Determination of amphetamine, methamphetamine and amphetamine-derived designer drugs or medicaments in blood and urine". J. Chromatogr. B. 713 (1): 163–187. doi:10.1016/S0378-4347(97)00515-X. PMID9700558.
↑Kraemer T, Paul LD (August 2007). "Bioanalytical procedures for determination of drugs of abuse in blood". Anal. Bioanal. Chem. 388 (7): 1415–1435. doi:10.1007/s00216-007-1271-6. PMID17468860.
↑Goldberger BA, Cone EJ (July 1994). "Confirmatory tests for drugs in the workplace by gas chromatography-mass spectrometry". J. Chromatogr. A. 674 (1–2): 73–86. doi:10.1016/0021-9673(94)85218-9. PMID8075776.
↑de la Torre R, Farré M, Navarro M, Pacifici R, Zuccaro P, Pichini S (2004). "Clinical pharmacokinetics of amfetamine and related substances: monitoring in conventional and non-conventional matrices". Clin Pharmacokinet. 43 (3): 157–185. doi:10.2165/00003088-200443030-00002. PMID14871155.
↑Baselt RC (2020). Disposition of toxic drugs and chemicals in man. Seal Beach, Ca.: Biomedical Publications. pp.1277–1280. ISBN978-0-578-57749-4.
↑Venkatratnam A, Lents NH (July 2011). "Zinc reduces the detection of cocaine, methamphetamine, and THC by ELISA urine testing". J. Anal. Toxicol. 35 (6): 333–340. doi:10.1093/anatox/35.6.333. PMID21740689.
↑Pervitin (in German), Berlin: CHEMIE.DE Information Service GmbH, archived from the original on 18 December 2019, retrieved 16 September 2015
↑Freye E (2009). Pharmacology and Abuse of Cocaine, Amphetamines, Ecstasy and Related Designer Drugs. University Düsseldorf, Germany: Springer. p.110. ISBN978-90-481-2447-3.
↑Rau TF, Kothiwal AS, Rova AR, Brooks DM, Poulsen DJ (August 2012). "Treatment with low-dose methamphetamine improves behavioral and cognitive function after severe traumatic brain injury". The Journal of Trauma and Acute Care Surgery. 73 (2 Suppl 1): S165–S172. doi:10.1097/TA.0b013e318260896a. PMID22847088.
↑O'Phelan K, McArthur DL, Chang CW, Green D, Hovda DA (September 2008). "The impact of substance abuse on mortality in patients with severe traumatic brain injury". The Journal of Trauma. 65 (3): 674–677. doi:10.1097/TA.0b013e31817db0a5. PMID18784583.
↑Cass WA, Smith MP, Peters LE (August 2006). "Calcitriol protects against the dopamine- and serotonin-depleting effects of neurotoxic doses of methamphetamine". Annals of the New York Academy of Sciences. 1074 (1): 261–271. Bibcode:2006NYASA1074..261C. doi:10.1196/annals.1369.023. PMID17105922.
↑Huang YN, Yang LY, Wang JY, Lai CC, Chiu CT, Wang JY (January 2017). "L-Ascorbate Protects Against Methamphetamine-Induced Neurotoxicity of Cortical Cells via Inhibiting Oxidative Stress, Autophagy, and Apoptosis". Molecular Neurobiology. 54 (1): 125–136. doi:10.1007/s12035-015-9561-z. PMID26732595.
Notes: (1) TAAR1 activity of ligands varies significantly between species. Some agents that are TAAR1 ligands in some species are not in other species. This navbox includes all TAAR1 ligands regardless of species. (2) See the individual pages for references, as well as the List of trace amines, TAAR, and TAAR1 pages. See also:Receptor/signaling modulators
This page is based on this Wikipedia article Text is available under the CC BY-SA 4.0 license; additional terms may apply. Images, videos and audio are available under their respective licenses.