Creatine was first identified in 1832 when Michel Eugène Chevreul isolated it from the basified water-extract of skeletal muscle. He later named the crystallized precipitate after the Greek word for meat, κρέας (kreas). In 1928, creatine was shown to exist in equilibrium with creatinine.[3] Studies in the 1920s showed that consumption of large amounts of creatine did not result in its excretion. This result pointed to the ability of the body to store creatine, which in turn suggested its use as a dietary supplement.[4]
In the 1960s, the enzyme creatine kinase (CK) was shown to phosphorylate ADP using phosphocreatine (PCr) to generate ATP. It follows that ATP - not PCr - is directly consumed in muscle contraction. CK uses creatine to buffer the ATP/ADP ratio.[9]
While creatine's influence on physical performance has been well documented since the early twentieth century, it came into public view following the 1992 Olympics in Barcelona. An 7 August 1992 article in The Times reported that Linford Christie, the gold medal winner at 100 meters, had used creatine before the Olympics (however, it should also be noted that Christie was found guilty of doping later in his career).[10] An article in Bodybuilding Monthly named Sally Gunnell, who was the gold medalist in the 400-meter hurdles, as another creatine user. In addition, The Times also noted that 100 meter hurdler Colin Jackson began taking creatine before the Olympics.[11][12]
At the time, low-potency creatine supplements were available in Britain, but creatine supplements designed for strength enhancement were not commercially available until 1993 when a company called Experimental and Applied Sciences (EAS) introduced the compound to the sports nutrition market under the name Phosphagen.[13] In 1996, researchers found that carbohydrate consumption augments the effects of creatine supplementation on skeletal muscle creatine accumulation.[14]
The cyclic derivative creatinine exists in equilibrium with its tautomer and with creatine.
Metabolic role
Creatine is a naturally occurring non-protein compound and the primary constituent of phosphocreatine, which is used to regenerate ATP within the cell. 95% of the human body's total creatine and phosphocreatine stores are found in skeletal muscle, while the remainder is distributed in the blood, brain, testes, and other tissues.[15][16] The typical creatine content of skeletal muscle (as both creatine and phosphocreatine) is 120mmol per kilogram of dry muscle mass, but can reach up to 160mmol/kg through supplementation.[17] Approximately 1–2% of intramuscular creatine is degraded per day and an individual would need about 1–3 grams of creatine per day to maintain average (unsupplemented) creatine storage.[17][18][19] An omnivorous diet provides roughly half of this value, with the remainder synthesized in the liver and kidneys.[15][16][20]
Creatine is transported through the blood and taken up by tissues with high energy demands, such as the brain and skeletal muscle, through an active transport system. The concentration of ATP in skeletal muscle is usually 2–5mM, which would result in a muscle contraction of only a few seconds.[22] During times of increased energy demands, the phosphagen (or ATP/PCr) system rapidly resynthesizes ATP from ADP with the use of phosphocreatine (PCr) through a reversible reaction catalysed by the enzyme creatine kinase (CK). The phosphate group is attached to an NH center of the creatine. In skeletal muscle, PCr concentrations may reach 20–35mM or more. Additionally, in most muscles, the ATP regeneration capacity of CK is very high and is therefore not a limiting factor. Although the cellular concentrations of ATP are small, changes are difficult to detect because ATP is continuously and efficiently replenished from the large pools of PCr and CK.[22] Creatine has the ability to increase muscle stores of PCr, potentially increasing the muscle's ability to resynthesize ATP from ADP to meet increased energy demands.[23][24][25]
Creatine supplementation, when combined with strength training, has been reported in humans to augment training-induced increases in satellite cell content and myonuclei number per muscle fiber, changes that may support increases in muscle fiber size.[26] In a separate study of rehabilitative strength training following immobilization, creatine supplementation was associated with increased muscle MRF4 protein expression; however, whether changes in MRF4 directly mediate myonuclear accretion or hypertrophy remains uncertain.[27]
Vegan and vegetarian diets are associated with lower levels of muscle creatine, and athletes on these diets may benefit from creatine supplementation.[30]
Pharmacokinetics
Most of the research to-date on creatine has predominantly focused on the pharmacological properties of creatine, yet there is a lack of research into the pharmacokinetics of creatine. Studies have not established pharmacokinetic parameters for clinical usage of creatine such as volume of distribution, clearance, bioavailability, mean residence time, absorption rate, and half life. A clear pharmacokinetic profile would need to be established prior to optimal clinical dosing.[31]
Dosing
Loading phase
Approximate muscle total creatine levels in mmol/kg dry weight muscle reported in the literature for vegetarians, individuals following a normal diet, and in response to creatine loading with or without carbohydrate (CHO) or CHO and protein (PRO). Dietary supplementation of creatine serves to increase muscle creatine and PCr by 20–40%.
An approximation of 0.3 g/kg/day divided into 4 equal spaced intervals has been suggested since creatine needs may vary based on body weight.[32][17] It has also been shown that taking a lower dose of 3 grams a day for 28 days can also increase total muscle creatine storage to the same amount as the rapid loading dose of 20 g/day for 6 days.[17] However, a 28-day loading phase does not allow for ergogenic benefits of creatine supplementation to be realized until fully saturated muscle storage.
This elevation in muscle creatine storage has been correlated with ergogenic benefits discussed in the research section. However, higher doses for longer periods of time are being studied to offset creatine synthesis deficiencies and mitigating diseases.[33][34][29]
Maintenance phase
After the 5–7 day loading phase, muscle creatine stores are fully saturated and supplementation only needs to cover the amount of creatine broken down per day. This maintenance dose was originally reported to be around 2–3 g/day (or 0.03 g/kg/day),[17] however, some studies have suggested 3–5 g/day maintenance dose to maintain saturated muscle creatine.[14][19][35][36]
Absorption
This graph shows the mean plasma creatine concentration (measured in μmol/L) over an 8-hour period following ingestion of 4.4grams of creatine in the form of creatine monohydrate (CrM), tri-creatine citrate (CrC), or creatine pyruvate (CrPyr).
Endogenous serum or plasma creatine concentrations in healthy adults are normally in a range of 2–12mg/L. A single 5 gram (5000mg) oral dose in healthy adults results in a peak plasma creatine level of approximately 120mg/L at 1–2 hours post-ingestion. Creatine has a fairly short elimination half life, averaging just less than 3 hours, so to maintain an elevated plasma level it would be necessary to take small oral doses every 3–6 hours throughout the day. [citation needed]
Creatine supplementation for sporting performance enhancement is considered safe for short-term and long-term use, but there is a lack of safety data for use in children and in pregnancy.[39][40]
According to a 2018 review article in the Journal of the International Society of Sports Nutrition creatine monohydrate is the most effective nutritional supplement to increase high intensity exercise capacity and muscle mass during training.[41]
Creatine use can increase maximum power and performance in high-intensity anaerobic repetitive work (periods of work and rest) by 5% to 15%.[42][43][44] Creatine supplementation exerts positive ergogenic effects on single and multiple bouts of short-duration, high-intensity exercise activities, in addition to potentiating exercise training adaptations.[45] Creatine has no significant effect on aerobic endurance.[46][obsoletesource][47][obsoletesource]
A 2014 survey of 21,000 US college athletes showed that 14% of athletes take creatine supplements.[48]
Research
Cognitive performance
Creatine is sometimes reported to have a beneficial effect on brain function and cognitive processing, although the evidence is difficult to interpret systematically and the appropriate dosing is unknown.[49][50] The greatest effect appears to be in individuals who are stressed (due, for instance, to sleep deprivation) or cognitively impaired.[49][50][51]
A 2018 systematic review found that "generally, there was evidence that short-term memory and intelligence/reasoning may be improved by creatine administration", whereas for other cognitive domains "the results were conflicting".[52]
A 2023 meta-analysis including 8 randomized controlled trials found that creatine supplementation improved memory performance with dosing parameters such as intake amounts and duration having no additional effects.[53] Any positive effects on cognition from creatine supplementation seem to be greater for older adults.[53]
A 2024 systematic review found no significant effect for healthy, unstressed individuals and mixed results for people under stress, suggesting that more research is needed to determine optimal dosing parameters and quantify changes in brain creatine levels during supplementation.[54]
A 2024 randomized trial involving 15 sleep-deprived subjects found that a single large dose of creatine (0.35 g/kg) may partially restore cognitive performance and resolve aberrant brain metabolism parameters.[55]
In a 2024 scientific opinion article, the European Food Safety Authority Panel on Nutrition, Novel Foods and Food Allergens determined that a cause and effect relationship cannot be established between creatine supplementation and increased cognitive function based on existing studies.[56] In particular, it ruled that there is currently insufficient evidence on the mechanisms by which creatine can impact cognition.
Muscular disease
A meta-analysis found that creatine treatment increased muscle strength in muscular dystrophies, and potentially improved functional performance.[57] Creatine treatment does not appear to improve muscle strength in people who have metabolic myopathies.[57] High doses of creatine lead to increased muscle pain and an impairment in activities of daily living when taken by people who have McArdle disease.[57]
Mitochondrial diseases
Parkinson's disease
Creatine's impact on mitochondrial function has led to research on its efficacy and safety for slowing Parkinson's disease. As of 2014, the evidence did not provide a reliable foundation for treatment decisions, due to risk of bias, small sample sizes, and the short duration of trials.[58]
Huntington's disease
Several primary studies[59][60][61] have been completed but no systematic review on Huntington's disease has been completed yet.
A 2021 systemic review of studies found that "the current body of evidence does not indicate that creatine supplementation increases total testosterone, free testosterone, DHT or causes hair loss/baldness".[63]
Cardiovascular disease
A 2011 systematic review evaluated the effectiveness of creatine and creatine analogues in adults with cardiovascular disease, including heart failure and myocardial infarction. The studies assessed the use of various creatine-based compounds—such as creatine, creatine phosphate, and phosphocreatinine—administered via oral, intravenous, or intramuscular routes, typically as adjuncts to standard therapy.
The analysis found no conclusive evidence that creatine or its analogues significantly affect mortality, myocardial infarction progression, or ejection fraction. However, some studies suggested a potential improvement in cardiac dysrhythmias and dyspnoea. The trials varied considerably in terms of drug formulation, dosage, treatment duration, and patient populations. Notably, no studies were identified that examined the effects of these compounds in patients with essential hypertension.
Due to the small sample sizes, clinical heterogeneity, and inconsistent outcomes across trials, the authors concluded that more rigorous and larger-scale studies are necessary to establish the clinical utility of creatine analogues in cardiovascular care.[64]
Pregnancy
It has been found that women who consumed ≥13 mg of creatine per kg of body mass daily have a lower risk of obstetric conditions. Creatines properties support energy for production, stabilization of maternal plasma creatine, improved pregnancy outcomes, as well as reduced oxidative stress. It was also found to reduce risk of preterm birth, support immune function, and reduce risk of perinatal brain injury. Perinatal brain injury occurs after hypoxia events, creatine allows cells to recover faster.[65]
One well-documented effect of creatine supplementation is weight gain within the first week of the supplement schedule, likely attributable to greater water retention due to the increased muscle creatine concentrations by means of osmosis.[68]
A 2009 systematic review discredited concerns that creatine supplementation could affect hydration status and heat tolerance and lead to muscle cramping and diarrhea.[69][70]
Despite weight gain due to water retention and potential cramps being two seemingly "common" side effects, new research indicates that these side effects are likely not the result of creatine usage. In addition, the initial water retention is attributed to more short-term creatine use (the "loading" phase). Studies have shown that creatine usage does not necessarily affect total body water relative to muscle mass in the long-term.[71]
Renal function
A 2019 systematic review published by the National Kidney Foundation investigated whether creatine supplementation had adverse effects on renal function.[72] They identified 15 studies from 1997 to 2013 that looked at standard creatine loading and maintenance protocols of 4–20 g/day of creatine versus placebo. They utilized serum creatinine, creatinine clearance, and serum urea levels as a measure of renal damage. While in general creatine supplementation resulted in slightly elevated creatinine levels that remained within normal limits, supplementation did not induce renal damage (P value< 0.001). Special populations included in the 2019 Systematic review included type 2 diabetic patients[73] and post-menopausal women,[74] bodybuilders,[75] athletes,[76] and resistance trained populations.[77][78][79] The study also discussed 3 case studies where there were reports that creatine affected renal function.[80][81][82]
In a joint statement between the American College of Sports Medicine, Academy of Nutrition and Dietetics, and Dietitians in Canada on performance enhancing nutrition strategies, creatine was included in their list of ergogenic aids and they do not list renal function as a concern for use.[83]
The most recent position stand on creatine from the Journal of International Society of Sports Nutrition states that creatine is safe to take in healthy populations from infants to the elderly to performance athletes. They also state that long term (5 years) use of creatine has been considered safe.[32]
Safety
Contamination
A 2011 survey of 33 supplements commercially available in Italy found that over 50% of them exceeded the European Food Safety Authority recommendations in at least one contaminant. The most prevalent of these contaminants was creatinine, a breakdown product of creatine also produced by the body.[84] Creatinine was present in higher concentrations than the European Food Safety Authority recommendations in 44% of the samples. About 15% of the samples had detectable levels of dihydro-1,3,5-triazine or a high dicyandiamide concentration. Heavy metals contamination was not found to be a concern, with only minor levels of mercury being detectable. Two studies reviewed in 2007 found no impurities.[85]
Food and cooking
When creatine is mixed with protein and sugar at high temperatures (above 148°C), the resulting reaction produces carcinogenic heterocyclic amines (HCAs).[86] Such a reaction happens when grilling or pan-frying meat.[87] Creatine content (as a percentage of crude protein) can be used as an indicator of meat quality.[88]
Dietary considerations
Creatine-monohydrate is suitable for vegetarians and vegans, as the raw materials used for the production of the supplement have no animal origin.[89]
↑Stout JR, Antonio J, Kalman E, eds. (2008). Essentials of Creatine in Sports and Health. Humana. ISBN978-1-59745-573-2.
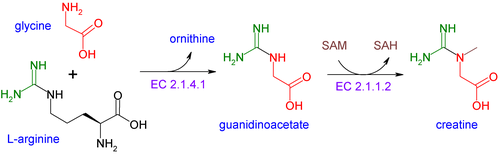
↑Barcelos RP, Stefanello ST, Mauriz JL, Gonzalez-Gallego J, Soares FA (2016). "Creatine and the Liver: Metabolism and Possible Interactions". Mini Reviews in Medicinal Chemistry. 16 (1): 12–8. doi:10.2174/1389557515666150722102613. PMID26202197. The process of creatine synthesis occurs in two steps, catalyzed by L-arginine:glycine amidinotransferase (AGAT) and guanidinoacetate N-methyltransferase (GAMT), which take place mainly in kidney and liver, respectively. This molecule plays an important energy/pH buffer function in tissues, and to guarantee the maintenance of its total body pool, the lost creatine must be replaced from diet or de novo synthesis.
↑Volek JS, Ballard KD, Forsythe CE (2008). "Overview of Creatine Metabolism". In Stout JR, Antonio J, Kalman E (eds.). Essentials of Creatine in Sports and Health. Humana. pp.1–23. ISBN978-1-59745-573-2.
12Green AL, Hultman E, Macdonald IA, Sewell DA, Greenhaff PL (November 1996). "Carbohydrate ingestion augments skeletal muscle creatine accumulation during creatine supplementation in humans". The American Journal of Physiology. 271 (5 Pt 1): E821-6. doi:10.1152/ajpendo.1996.271.5.E821. PMID8944667.
12Cooper R, Naclerio F, Allgrove J, Jimenez A (July 2012). "Creatine supplementation with specific view to exercise/sports performance: an update". Journal of the International Society of Sports Nutrition. 9 (1) 33. doi:10.1186/1550-2783-9-33. PMC3407788. PMID22817979. Creatine is produced endogenously at an amount of about 1 g/d. Synthesis predominately occurs in the liver, kidneys, and to a lesser extent in the pancreas. The remainder of the creatine available to the body is obtained through the diet at about 1 g/d for an omnivorous diet. 95% of the bodies creatine stores are found in the skeletal muscle and the remaining 5% is distributed in the brain, liver, kidney, and testes [1].
12Brosnan ME, Brosnan JT (August 2016). "The role of dietary creatine". Amino Acids. 48 (8): 1785–91. doi:10.1007/s00726-016-2188-1. PMID26874700. S2CID3700484. The daily requirement of a 70-kg male for creatine is about 2g; up to half of this may be obtained from a typical omnivorous diet, with the remainder being synthesized in the body... More than 90% of the body's creatine and phosphocreatine is present in muscle (Brosnan and Brosnan 2007), with some of the remainder being found in the brain (Braissant et al. 2011).... Creatine synthesized in liver must be secreted into the bloodstream by an unknown mechanism (Da Silva et al. 2014a)
12345Hultman E, Söderlund K, Timmons JA, Cederblad G, Greenhaff PL (July 1996). "Muscle creatine loading in men". Journal of Applied Physiology. 81 (1): 232–7. doi:10.1152/jappl.1996.81.1.232. PMID8828669.
12Harris RC, Söderlund K, Hultman E (September 1992). "Elevation of creatine in resting and exercised muscle of normal subjects by creatine supplementation". Clinical Science. 83 (3): 367–74. doi:10.1042/cs0830367. PMID1327657.
↑Brosnan JT, da Silva RP, Brosnan ME (May 2011). "The metabolic burden of creatine synthesis". Amino Acids. 40 (5): 1325–31. doi:10.1007/s00726-011-0853-y. PMID21387089. S2CID8293857. Creatinine loss averages approximately 2g (14.6mmol) for 70kg males in the 20- to 39-year age group.... Table 1 Comparison of rates of creatine synthesis in young adults with dietary intakes of the three precursor amino acids and with the whole body transmethylation flux Creatine synthesis (mmol/day)8.3
↑Wallimann, Theo; Tokarska-Schlattner, Malgorzata; Neumann, Dietbert; Epand, Richard M.; Epand, Raquel F.; Andres, Robert H.; Widmer, Hans Rudolf; Hornemann, Thorsten; Saks, Valdur; Agarkova, Irina; Schlattner, Uwe (2007). "The Phosphocreatine Circuit: Molecular and Cellular Physiology of Creatine Kinases, Sensitivity to Free Radicals, and Enhancement by Creatine Supplementation". Molecular System Bioenergetics. pp.195–264. doi:10.1002/9783527621095.ch7. ISBN978-3-527-31787-5.
↑Hanna-El-Daher L, Braissant O (August 2016). "Creatine synthesis and exchanges between brain cells: What can be learned from human creatine deficiencies and various experimental models?". Amino Acids. 48 (8): 1877–95. doi:10.1007/s00726-016-2189-0. PMID26861125. S2CID3675631.
↑Kreider RB (February 2003). "Effects of creatine supplementation on performance and training adaptations". Molecular and Cellular Biochemistry. 244 (1–2): 89–94. doi:10.1023/A:1022465203458. PMID12701815. S2CID35050122.
↑Greenhaff PL, Casey A, Short AH, Harris R, Soderlund K, Hultman E (May 1993). "Influence of oral creatine supplementation of muscle torque during repeated bouts of maximal voluntary exercise in man". Clinical Science. 84 (5): 565–71. doi:10.1042/cs0840565. PMID8504634.
↑Graham AS, Hatton RC (1999). "Creatine: a review of efficacy and safety". Journal of the American Pharmaceutical Association. 39 (6): 803–10, quiz 875–7. doi:10.1016/s1086-5802(15)30371-5. PMID10609446.
↑Abbie E. Smith-Ryan, Gabrielle M. DelBiondo, Ann F. Brown, Susan M. Kleiner, Nhi T. Tran & Stacey J. Ellery (2025) Creatine in Women's Health: Bridging the gap from Menstruation Through Pregnancy to Menopause, Journal of the International Society of Sports Nutrition, 22:1, 2502094, DOI: 10.1080/15502783.2025.2502094
↑Francaux M, Poortmans JR (December 2006). "Side effects of creatine supplementation in athletes". International Journal of Sports Physiology and Performance. 1 (4): 311–23. doi:10.1123/ijspp.1.4.311. PMID19124889. S2CID21330062.
↑de Souza E, Silva A, Pertille A, Reis Barbosa CG, Aparecida de Oliveira Silva J, de Jesus DV, etal. (November 2019). "Effects of Creatine Supplementation on Renal Function: A Systematic Review and Meta-Analysis". Journal of Renal Nutrition. 29 (6): 480–489. doi:10.1053/j.jrn.2019.05.004. PMID31375416. S2CID199388424.
↑Gualano B, de Salles Painelli V, Roschel H, Lugaresi R, Dorea E, Artioli GG, etal. (May 2011). "Creatine supplementation does not impair kidney function in type 2 diabetic patients: a randomized, double-blind, placebo-controlled, clinical trial". European Journal of Applied Physiology. 111 (5): 749–56. doi:10.1007/s00421-010-1676-3. PMID20976468. S2CID21335546.
↑Neves M, Gualano B, Roschel H, Lima FR, Lúcia de Sá-Pinto A, Seguro AC, etal. (June 2011). "Effect of creatine supplementation on measured glomerular filtration rate in postmenopausal women". Applied Physiology, Nutrition, and Metabolism. 36 (3): 419–22. doi:10.1139/h11-014. PMID21574777.
↑Kreider RB, Melton C, Rasmussen CJ, Greenwood M, Lancaster S, Cantler EC, etal. (February 2003). "Long-term creatine supplementation does not significantly affect clinical markers of health in athletes". Molecular and Cellular Biochemistry. 244 (1–2): 95–104. doi:10.1023/A:1022469320296. PMID12701816. S2CID25947100.
↑Cancela P, Ohanian C, Cuitiño E, Hackney AC (September 2008). "Creatine supplementation does not affect clinical health markers in football players". British Journal of Sports Medicine. 42 (9): 731–5. doi:10.1136/bjsm.2007.030700. PMID18780799. S2CID20876433.
↑Mayhew DL, Mayhew JL, Ware JS (December 2002). "Effects of long-term creatine supplementation on liver and kidney functions in American college football players". International Journal of Sport Nutrition and Exercise Metabolism. 12 (4): 453–60. doi:10.1123/ijsnem.12.4.453. PMID12500988.
↑Thorsteinsdottir B, Grande JP, Garovic VD (October 2006). "Acute renal failure in a young weight lifter taking multiple food supplements, including creatine monohydrate". Journal of Renal Nutrition. 16 (4): 341–5. doi:10.1053/j.jrn.2006.04.025. PMID17046619.
↑Moreta S, Prevarin A, Tubaro F (June 2011). "Levels of creatine, organic contaminants and heavy metals in creatine dietary supplements". Food Chemistry. 126 (3): 1232–1238. doi:10.1016/j.foodchem.2010.12.028.
↑Dahl O (1 July 1963). "Meat Quality Measurement, Creatine Content as an Index of Quality of Meat Products". Journal of Agricultural and Food Chemistry. 11 (4): 350–355. Bibcode:1963JAFC...11..350D. doi:10.1021/jf60128a026.
This page is based on this Wikipedia article Text is available under the CC BY-SA 4.0 license; additional terms may apply. Images, videos and audio are available under their respective licenses.