| Anabolic–androgenic steroids | |
|---|---|
| Drug class | |
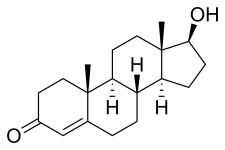 Chemical structure of the natural AAS testosterone (androst-4-en-17β-ol-3-one). | |
| Class identifiers | |
| Synonyms | Anabolic steroids; Androgens |
| Use | Various |
| ATC code | A14A |
| Biological target | Androgen receptor (AR) |
| Chemical class | Steroids; Androstanes; Estranes |
| Clinical data | |
| Drugs.com | Drug Classes |
| External links | |
| MeSH | D045165 |
| Legal status | |
| Legal status |
|
| In Wikidata | |
Anabolic steroids, also known as anabolic-androgenic steroids (AAS), are a class of drugs that are structurally related to testosterone, the main male sex hormone, and produce effects by binding to the androgen receptor (AR). Anabolic steroids have a number of medical uses, [1] but are also used by athletes to increase muscle size, strength, and performance.
Contents
- Uses
- Medical
- Enhancing performance
- Dosages
- Available forms
- Routes of administration
- Adverse effects
- Physiological
- Neuropsychiatric
- Reproductive
- Pharmacology
- Mechanism of action
- Anabolic and androgenic effects
- Dissociation of effects
- GABAA receptor modulation
- Comparison of AAS
- Chemistry
- Structural conversions of anabolic steroids
- Detection in body fluids
- History
- Discovery of androgens
- Development of synthetic AAS
- Society and culture
- Etymology
- Legal status
- Status in sports
- Usage
- Economics
- Research
- See also
- References
- Further reading
- External links
Health risks can be produced by long-term use or excessive doses of AAS. [2] [3] These effects include harmful changes in cholesterol levels (increased low-density lipoprotein and decreased high-density lipoprotein), acne, high blood pressure, liver damage (mainly with most oral AAS), and left ventricular hypertrophy. [4] These risks are further increased when athletes take steroids alongside other drugs, causing significantly more damage to their bodies. [5] The effect of anabolic steroids on the heart can cause myocardial infarction and strokes. [5] Conditions pertaining to hormonal imbalances such as gynecomastia and testicular size reduction may also be caused by AAS. [6] In women and children, AAS can cause irreversible masculinization. [6]
Ergogenic uses for AAS in sports, racing, and bodybuilding as performance-enhancing drugs are controversial because of their adverse effects and the potential to gain advantage in physical competitions. Their use is referred to as doping and banned by most major sporting bodies. Athletes have been looking for drugs to enhance their athletic abilities since the Olympics started in Ancient Greece. [5] For many years, AAS have been by far the most-detected doping substances in IOC-accredited laboratories. [7] [8] Anabolic steroids are classified as Schedule III controlled substances in many countries, [9] meaning that AAS have recognized medical use but are also recognized as having a potential for abuse and dependence, leading to their regulation and control. In countries where AAS are controlled substances, there is often a black market in which smuggled, clandestinely manufactured or even counterfeit drugs are sold to users.