 | |
| Clinical data | |
|---|---|
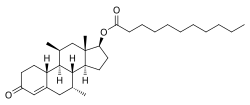
| Other names | Dimethandrolone undecylate; DMAU; CDB-4521; Dimethylnandrolone undecanoate; 7α,11β-Dimethyl-19-nortestosterone 17β-undecanoate; 7α,11β-Dimethylestr-4-en-17β-ol-3-one 17β-undecanoate |
| Routes of administration | By mouth, intramuscular injection [1] |
| Drug class | Androgen; Anabolic steroid; Androgen ester; Progestogen |
| Identifiers | |
| |
| CAS Number | |
| PubChem CID | |
| DrugBank | |
| ChemSpider | |
| UNII | |
| Chemical and physical data | |
| Formula | C31H50O3 |
| Molar mass | 470.738 g·mol−1 |
| 3D model (JSmol) | |
| |
| |
Dimethandrolone undecanoate (DMAU), also known by its developmental code name CDB-4521, is an experimental androgen/anabolic steroid (AAS) and progestogen medication which is under development as a potential birth control pill for men. [2] [3] [4] It is taken by mouth, but can also be given by injection into muscle. [2] [3] [1]
Contents
- Medical uses
- Side effects
- Low estrogen levels
- Liver toxicity
- Pharmacology
- Pharmacodynamics
- Pharmacokinetics
- Chemistry
- History
- References
Side effects of DMAU include mild weight gain and mild decreases in levels of HDL cholesterol. [5] [6] It may also cause low estrogen levels and associated symptoms such as reduced sexual function and decreased bone mineral density. [7] [8] DMAU is an AAS, and hence is an agonist of the androgen receptor, the biological target of androgens like testosterone. [2] [3] It is also a progestin, or a synthetic progestogen, and hence is an agonist of the progesterone receptor, the biological target of progestogens like progesterone. [2] [3] Due to its androgenic and progestogenic activity, DMAU has antigonadotropic effects. [2] [3] These effects result in reversible suppression of sperm production and are responsible for the contraceptive effects of DMAU in men. [2] [3] The medication has no estrogenic activity. [7] DMAU is a prodrug of dimethandrolone. [2] [3]
DMAU was first described in 2002. [9] It was developed by the Contraceptive Development Branch of the National Institute of Child Health and Human Development, an agency in the United States government. [2] [3] [4]