 | |
 | |
| Clinical data | |
|---|---|
| Pronunciation | /tɛˈstɒstəroʊnənˈdɛkənoʊeɪt/ teh-STOS-tə-rohn ən-DEK-ə-noh-ayt |
| Trade names | Oral: Kyzatrex, Andriol, Jatenzo, Testoheal, others IM: Aveed, Nebido, others |
| Other names | TU; Testosterone undecylate; Testosterone 17β-undecanoate; ORG-538; CLR-610 |
| AHFS/Drugs.com | Monograph |
| MedlinePlus | a614041 |
| License data | |
| Pregnancy category |
|
| Dependence liability | Moderate [2] |
| Addiction liability | Moderate [2] |
| Routes of administration | By mouth, intramuscular injection |
| Drug class | Androgen; Anabolic steroid; Androgen ester |
| ATC code | |
| Legal status | |
| Legal status |
|
| Pharmacokinetic data | |
| Bioavailability | Oral: 3–7%[ medical citation needed ] Intramuscular: high |
| Protein binding | High (testosterone) |
| Metabolism | Liver |
| Metabolites | Testosterone, undecanoic acid, metabolites of testosterone |
| Elimination half-life | IM (in tea seed oil): 20.9 days [6] [7] IM (in castor oil): 33.9 days [6] [7] |
| Excretion | ~90% Urine, 6% feces |
| Identifiers | |
| |
| CAS Number | |
| PubChem CID | |
| DrugBank | |
| ChemSpider | |
| UNII | |
| KEGG | |
| ChEBI | |
| ChEMBL | |
| CompTox Dashboard (EPA) | |
| ECHA InfoCard | 100.025.193 |
| Chemical and physical data | |
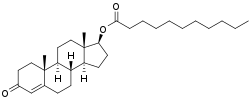
| Formula | C30H48O3 |
| Molar mass | 456.711 g·mol−1 |
| 3D model (JSmol) | |
| |
| |
| (verify) | |
Testosterone undecanoate, sold under the brand name Nebido among others, is an androgen and anabolic steroid (AAS) medication that is used mainly in the treatment of low testosterone levels in men, [8] [6] [9] [10] [11] [12] [13] It is taken by mouth or given by injection into muscle. [10] [14]
Contents
- Medical uses
- Side effects
- Anaphylaxis
- Pharmacology
- Pharmacodynamics
- Pharmacokinetics
- Chemistry
- History
- Society and culture
- Generic names
- Brand names
- Availability
- Legal status
- Research
- Non-alcoholic steatohepatitis
- Osteoporosis
- Health implications
- Risks associated with treatment of late-onset hypogonadism
- Body composition
- Bone density
- References
Side effects of testosterone undecanoate include symptoms of masculinization like acne, increased hair growth, voice changes, hypertension, elevated liver enzymes, hypertriglyceridemia, and increased sexual desire. [10] The drug is a prodrug of testosterone, the biological ligand of the androgen receptor (AR) and hence is an androgen and anabolic steroid. [15] [10] It has strong androgenic effects and moderate anabolic effects, which make it useful for producing masculinization and suitable for androgen replacement therapy. [10] Testosterone undecanoate is a testosterone ester and a prodrug of testosterone in the body. [9] [8] [6] Because of this, it is considered to be a natural and bioidentical form of testosterone. [16]
Testosterone undecanoate was introduced in China for use by injection and in the European Union for use by mouth in the 1970s. [17] [18] It became available for use by injection in the European Union in the early to mid 2000s and in the United States in 2014. [19] [20] Formulations for use by mouth are approved in the United States. [3] [4] [21] Along with testosterone enanthate, testosterone cypionate, and testosterone propionate, testosterone undecanoate is one of the most widely used testosterone esters. [15] [6] [10] However, it has advantages over other testosterone esters in that it can be taken by mouth and in that it has a far longer duration when given by injection. [22] [8] [6] [7] [10] In addition to its medical use, testosterone undecanoate is used to improve physique and performance. [10] The drug is a controlled substance in many countries. [10]
Oral administration of testosterone undecanoate is an effective method to achieve therapeutic physiological levels of serum testosterone in patients with hypogonadism. In addition, oral therapy has been found to have a positive impact in these patients on quality of life factors such as sexual function, mood, and mental status, as documented in various studies. [23]