EMP is indicated, in the United States, for the palliative treatment of metastatic and/or progressive prostate cancer,[4] whereas in the United Kingdom it is indicated for the treatment of unresponsive or relapsing prostate cancer.[17][6][1][10] The medication is usually reserved for use in hormone-refractory cases of prostate cancer, although it has been used as a first-line monotherapy as well.[3]Response rates with EMP in prostate cancer are said to be equivalent to conventional high-dose estrogen therapy.[18]
Due to its relatively severe side effects and toxicity, EMP has rarely been used in the treatment of prostate cancer.[5] This is especially true in Western countries today.[5] As a result, and also due to the scarce side effects of gonadotropin-releasing hormone modulators (GnRH modulators) like leuprorelin, EMP was almost abandoned.[3] However, encouraging clinical research findings resulted in renewed interest of EMP for the treatment of prostate cancer.[3]
EMP has been used at doses of 140 to 1,400mg/day orally in the treatment of prostate cancer.[19] However, oral EMP is most commonly used at a dose of 560 to 640mg/day (280–320mg twice daily).[1] The recommended dosage of oral EMP in the Food and Drug Administration (FDA) label for Emcyt is 14mg per kg of body weight (i.e., one 140mg oral capsule for each 10kg or 22lbs of body weight) given in 3 or 4 divided doses per day.[7] The label states that most patients in studies of oral EMP in the United States have received 10 to 16mg per kg per day.[7] This would be about 900 to 1,440mg/day for a 90-kg or 200-lb man.[7] Lower doses of oral EMP, such as 280mg/day, have been found to have comparable effectiveness as higher doses but with improved tolerability and reduced toxicity.[5] Doses of 140mg/day have been described as a very low dosage.[20] EMP has been used at doses of 240 to 450mg/day intravenously.[1]
The side effects of EMP overall have been described as relatively severe.[3] The most common side effects of EMP have been reported to be gastrointestinal side effects like nausea, vomiting, and diarrhea, with nausea and vomiting occurring in 40% of men.[9][1] They are usually mild or moderate in severity, and the nausea and vomiting can be managed with prophylacticantiemetic medications.[9] Nonetheless, severe cases of gastrointestinal side effects with EMP may require dose reduction or discontinuation of therapy.[1] Although nausea and vomiting have been reported to be the most common side effects of EMP, gynecomastia (male breast development) has been found to occur in as many as 83% of men treated with EMP, and the incidence of erectile dysfunction is possibly similar to or slightly less than the risk of gynecomastia.[3] As a rule, feminization, a gynoid fat distribution, demasculinization, and impotence are said to occur in virtually or nearly 100% of men treated with high-dose estrogen therapy.[13][26] Decreased sexual activity has also been reported in men treated with EMP.[1] These side effects are due to high estrogen levels and low testosterone levels.[1][3] Prophylactic irradiation of the breasts can be used to decrease the incidence and severity of gynecomastia with estrogens.[13]
Adverse liver function tests are commonly seen with EMP, but severe liver dysfunction is rare with the medication.[1]Central nervous system side effects are rarely seen with EMP, although enlarged ventricles and neuronalpigmentation have been reported in monkeys treated with very high doses of EMP (20–140mg/kg/day) for 3 to 6months.[1] EMP does not appear to have cytostatic effects in normal brain tissue.[1] In women treated with EMP in clinical studies, a few instances of minor gynecologicalhemorrhages have been observed.[1] EMP is described as relatively well tolerated among cytostatic antineoplastic and nitrogen-mustard agents, rarely or not at all being associated with significant hematologictoxicity such as myelosuppression (bone marrow suppression), gastrointestinal toxicity, or other more marked toxicity associated with such agents.[6][1][31] In contrast to most other cytostatic agents, which often cause myelosuppression, leukopenia (decreased white blood cell count), and neutropenia (decreased neutrophil count), EMP actually produces leukocytosis (increased white blood cell count) as a side effect.[32][33]
In a small low-dose study using 280mg/day oral EMP for 150days, tolerability was significantly improved, with gastrointestinal irritation occurring in only 15% of men, and there was no incidence of severe cardiovascular toxicity or deep vein thrombosis.[3][5] In addition, no other side effects besides slight transient elevated liver enzymes were observed.[3] These findings suggest that lower doses of oral EMP may be a safer option than higher doses for the treatment of prostate cancer.[5] However, a subsequent 2004 meta-analysis of 23studies of thromboembolic events with EMP found substantial incidence of thromboembolic events regardless of dosage and no association of EMP dose with risk of these complications.[28]
Footnotes:a = Could not be estimated from available data. b = Especially during the first 2weeks of therapy. c = Angioedema (Quincke edema, larynx edema) can occur. Often occurs in combination with ACE inhibitors. EMP should be immediately discontinued if angioedema occurs. Sources: See template.
There has been no clinical experience with overdose of EMP.[7] Overdose of EMP may result in pronounced manifestations of the known adverse effects of the medication.[7] There is no specific antidote for overdose of EMP.[17] In the event of overdose, gastric lavage should be used to evacuate gastric contents as necessary and treatment should be symptom-based and supportive.[7][17] In the case of dangerously low counts of red blood cells, white blood cells, or platelets, whole blood may be given as needed.[17]Liver function should be monitored with EMP overdose.[17] After an overdose of EMP, hematological and hepatic parameters should continue to be monitored for at least 6weeks.[7]
EMP has been used at high doses of as much as 1,260mg/day by the oral route and 240 to 450mg/day by intravenous injection.[3][1]
EMP acts by a dual mechanism of action: 1) direct cytostatic activity via a number of actions; and 2) as a form of high-dose estrogen therapy via estrogen receptor-mediated antigonadotropic and functional antiandrogenic effects.[1][3][14] The antigonadotropic and functional antiandrogenic effects of EMP consist of strong suppression of gonadalandrogenproduction and hence circulating levels of androgens such as testosterone; greatly increased levels of sex hormone-binding globulin and hence a decreased fraction of free androgens in the circulation; and direct antiandrogenic actions in prostate cells.[31][1][3][5][36][37][38] The free androgen index with oral EMP has been found to be on average 4.6-fold lower than with orchiectomy.[37] As such, EMP therapy results in considerably stronger androgen deprivation than orchiectomy.[38] Metabolites of EMP, including estramustine, estromustine, estradiol, and estrone, have been found to act as weak antagonists of the androgen receptor (EC50Tooltip half-maximal effective concentration = 0.5–3.1μM), although the clinical significance of this is unknown.[39][36][3][1]
Extremely high levels of estradiol and estrone occur during EMP therapy.[3][5] The estrogenic metabolites of EMP are responsible for its most common adverse effects and its cardiovasculartoxicity.[1] EMP has been described as having relatively weak estrogenic effects in some publications.[6][31] However, it has shown essentially the same rates and degrees of estrogenic effects, such as breast tenderness, gynecomastia, cardiovascular toxicity, changes in liver protein synthesis, and testosterone suppression, as high-dose diethylstilbestrol and ethinylestradiol in clinical studies.[7][5][31][38][40] The notion that EMP has relatively weak estrogen activity may have been based on animal research, which found that EMP had 100-fold lower uterotrophic effects than estradiol in rats, and may also not have taken into account the very high doses of EMP used clinically in humans.[40][41]
The mechanism of action of the cytostatic effects of EMP is complex and only partially understood.[1] EMP is considered to mainly be a mitotic inhibitor, inhibiting mechanisms involved in the mitosis phase of the cell cycle.[1][5] Specifically, it binds to microtubule-associated proteins and/or to tubulin and produces depolymerization of microtubules (Kd = 10–20μM for estramustine), resulting in the arrest of cell division in the G2/M phase (specifically metaphase).[1][5][42] EMP was originally thought to mediate its cytostatic effects as a prodrug of normustine, a nitrogen mustard, and hence was thought to be an alkylating antineoplastic agent.[3][10][6][14] However, subsequent research has found that EMP is devoid of alkylating actions, and that the influence of EMP on microtubules is mediated by intact estramustine and estromustine, with normustine or estradiol alone having only minor or negligible effects.[1][3][43] As such, the unique properties of the estramustine and estromustine structures, containing a carbamate-esterbond, appear to be responsible for the cytostatic effects of EMP.[1] In addition to its antimitotic actions, EMP has also been found to produce other cytostatic effects, including induction of apoptosis, interference with DNA synthesis, nuclear matrix interaction, cell membrane alterations, induction of reactive oxygen species (free oxygen radicals), and possibly additional mechanisms.[1][5] EMP has been found to have a radiosensitizing effect in prostate cancer and glioma cells, improving sensitivity to radiation therapy as well.[1]
The cytostatic metabolites of EMP are accumulated in tissues in a selective manner, for instance in prostate cancercells.[6][1][5] This may be due to the presence of a specific estramustine-binding protein (EMBP) (Kd = 10–35nM for estramustine), also known as prostatin or prostatic secretion protein (PSP), which has been detected in prostate cancer, glioma, melanoma, and breast cancer cells.[1][5][44] Because of its tissue selectivity, EMP is said to produce minimal cytostatic effects in healthy tissues, and its tissue selectivity may be responsible for its therapeutic cytostatic efficacy against prostate cancer cells.[6][5][1]
EMP was originally developed as a dual ester prodrug of an estrogen and normustine as a nitrogen mustard alkylating antineoplastic agent which, due to the affinity of the estrogen moiety for estrogen receptors, would be selectively accumulated in estrogen target tissues and hence estrogen receptor-positive tumor cells.[5][14][2] Consequentially, it was thought that EMP would preferentially deliver the alkylating normustine moiety to these tissues, allowing for reduced cytostatic effects in healthy tissues and hence improved efficacy and tolerability.[5] However, subsequent research found that there is very limited and slow cleavage of the normustine ester and that EMP is devoid of alkylating activity.[5][1][3][31] In addition, it appears that estramustine and estromustine may be preferentially accumulated in estrogen target tissues not due to affinity for the estrogen receptors, but instead due to affinity for the distinct EMBP.[1][3]
EMP at a dosage 280mg/day has been found to suppress testosterone levels in men into the castrate range (to 30ng/dL) within 20days and to the low castrate range (to 10ng/dL) within 30days.[3] Similarly, a dosage of 70mg/day EMP suppressed testosterone levels into the castrate range within 4weeks.[3]
The oral bioavailability of EMP is low, which is due to profound first-pass metabolism; specifically, dephosphorylation of EMP.[1] The oral bioavailability of EMP specifically as estramustine and estromustine is 44 to 75%, suggesting that absorption may be incomplete.[1] In any case, there is a linear relationship between the oral dose of EMP and circulating levels of estramustine and estromustine.[1] Consumption of calcium, aluminium, or magnesium with oral EMP can markedly impair its bioavailability due to diminished absorption from the intestines, and this may interfere with its therapeutic effectiveness at low doses.[3][17]
Following a single oral dose of 420mg EMP in men with prostate cancer, maximal levels of estromustine were 310 to 475ng/mL (475,000pg/mL) and occurred after 2 to 3hours.[1] Estradiol levels with 280mg/day oral EMP have been found to increase to very high concentrations within one week of therapy.[3] In one study, levels of estradiol were over 20,000pg/mL after 10days, were about 30,000pg/mL after 30days, and peaked at about 40,000pg/mL at 50days.[3] Another study found lower estradiol levels of 4,900 to 9,000pg/mL during chronic therapy with 560mg/day oral EMP.[31] An additional study found estradiol levels of about 17,000pg/mL with 140mg/day oral EMP and 38,000pg/mL with 280mg/day oral EMP.[citation needed] The circulating levels of estradiol and estrone during EMP therapy have been reported to exceed normal levels in men by more than 100- and 1,000-fold, respectively.[5][31] Levels of estramustine and estradiol in the circulation are markedly lower than those of estromustine and estrone, respectively, with a ratio of about 1:10 in both cases.[1][31] Nonetheless, estradiol levels during EMP therapy appear to be similar to those that occur in mid-to-late pregnancy, which range from 5,000 to 40,000pg/mL.[50] No unchanged EMP is seen in the circulation with oral administration.[1]
The pharmacokinetics of EMP are different with intravenous injection.[1] Following a single intravenous injection of 300mg EMP, levels of EMP were higher than those of its metabolites for the first 8hours.[1] This is likely due to the bypassing of first-pass metabolism.[1] However, by 24hours after the dose, unchanged EMP could no longer be detected in the circulation.[1] The clearance of EMP from blood plasma is 4.85 ± 0.684L/h.[1] The volumes of distribution of EMP with intravenous injection were small; under a two-compartment model, the volume of distribution for the central compartment was 0.043L/kg and for the peripheral compartment was 0.11L/kg.[1] The plasma protein binding of EMP is high.[1] Estramustine is accumulated in tumor tissue, for instance prostate cancer and glioma tissue, with estramustine levels much higher in these tissues than in plasma (e.g., 6.3- and 15.9-fold, respectively).[1] Conversely, levels of estromustine in tumor versus plasma are similar (1.0- and 0.5-fold, respectively).[1] Estramustine and estromustine appear to accumulate in adipose tissue.[1]
The elimination half-life of estromustine with oral EMP was 13.6hours on average, with a range of 8.8 to 22.7hours.[1] Conversely, the elimination half-life of estromustine with intravenous injection was 10.3hours, with a range of 7.36 to 12.3hours.[1] For comparison, the corresponding elimination half-lives of estrone were 16.5 and 14.7 hours for oral and intravenous administration, respectively.[1] Estramustine and estromustine are mainly excreted in bile and hence in feces.[1][31] They are not believed to be excreted in urine.[1]
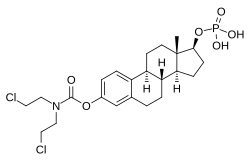
Metabolism of oral estramustine phosphate in humans.
Due to its hydrophilic phosphate ester moiety, EMP is a readily water-soluble compound.[51][52][53] This is in contrast to most other estradiol esters, which are fatty acid esters and lipophilic compounds that are not particularly soluble in water.[2] Unlike EMP, estramustine is highly lipophilic, practically insoluble in water, and non-ionizable.[19] The phosphate ester of EMP was incorporated into the molecule in order to increase its water solubility and allow for intravenous administration.[7]
The molecular weight of EMP sodium is 564.3g/mol, of EMP meglumine is 715.6g/mol, of EMP is 520.4g/mol, of estramustine is 440.4g/mol, and of estradiol is 272.4g/mol.[54] As a result of these differences in molecular weights, EMP contains about 52%, EMP sodium about 48%, and EMP meglumine about 38% of the amount of estradiol within their structures as does an equal-mass quantity of estradiol.[54]
EMP was first synthesized in the mid-1960s and was patented in 1967.[42] It was initially developed for the treatment of breast cancer.[1] The idea for EMP was inspired by the uptake and accumulation of radiolabeled estrogens into breast cancer tissue.[1] However, initial clinical findings of EMP in women with breast cancer were disappointing.[1] Subsequently, radiolabeled EMP was found to be taken up into and accumulated rat prostate gland, and this finding culminated in the medication being repurposed for the treatment of prostate cancer.[1][3] EMP was introduced for medical use in the treatment of this condition in the early 1970s, and was approved in the United States for this indication in 1981.[1][3][55] EMP was originally introduced for use by intravenous injection.[31] Subsequently, an oral formulation was introduced, and the intravenous preparation was almost abandoned in favor of the oral version.[31]
Society and culture
Generic names
EMP is provided as the sodiumsalt for oral administration, which has the generic namesestramustine phosphate sodium (USANTooltip United States Adopted Name) and estramustine sodium phosphate (BANMTooltip British Approved Name, JANTooltip Japanese Accepted Name), and as the meglumine salt for intravenous administration, which has the generic name estramustine phosphate meglumine.[24][35][15][56][16] The INNMTooltip International Nonproprietary Name is estramustine phosphate.[35] The name estramustine phosphate is a contraction of estradiol normustine phosphate.[35][16] EMP is also known by its former developmental code names Leo 299, Ro 21-8837, and Ro 21-8837/001.[35][15][16]
Brand names
EMP is most commonly marketed under the brand names Estracyt and Emcyt, but has also been sold under a number of other brand names, including Amsupros, Biasetyl, Cellmustin, Estramustin HEXAL, Estramustina Filaxis, Estranovag, Multosin, Multosin Injekt, Proesta, Prostamustin, and Suloprost.[15][16][24]
EMP has been studied in the treatment of other cancers such as glioma and breast cancer.[1] It has been found to slightly improve quality of life in people with glioma during the first 3months of therapy.[1]
12Hedlund PO, Henriksson P (March 2000). "Parenteral estrogen versus total androgen ablation in the treatment of advanced prostate carcinoma: effects on overall survival and cardiovascular mortality. The Scandinavian Prostatic Cancer Group (SPCG)-5 Trial Study". Urology. 55 (3): 328–333. doi:10.1016/s0090-4295(99)00580-4. PMID10699602.
↑Shimizu TS, Shibata Y, Jinbo H, Satoh J, Yamanaka H (1995). "Estramustine phosphate for preventing flare-up in luteinizing hormone-releasing hormone analogue depot therapy". European Urology. 27 (3): 192–195. doi:10.1159/000475159. PMID7541359.
↑Cox RL, Crawford ED (December 1995). "Estrogens in the treatment of prostate cancer". The Journal of Urology. 154 (6): 1991–1998. doi:10.1016/S0022-5347(01)66670-9. PMID7500443.
12Lubiniecki GM, Berlin JA, Weinstein RB, Vaughn DJ (December 2004). "Thromboembolic events with estramustine phosphate-based chemotherapy in patients with hormone-refractory prostate carcinoma: results of a meta-analysis". Cancer. 101 (12): 2755–2759. doi:10.1002/cncr.20673. PMID15536625. S2CID21465413.
↑Fizazi K, Le Maitre A, Hudes G, Berry WR, Kelly WK, Eymard JC, etal. (November 2007). "Addition of estramustine to chemotherapy and survival of patients with castration-refractory prostate cancer: a meta-analysis of individual patient data". The Lancet. Oncology. 8 (11): 994–1000. doi:10.1016/S1470-2045(07)70284-X. PMID17942366.
12Alexander NC, Hancock AK, Masood MB, Peet BG, Price JJ, Turner RL, etal. (March 1979). "Estracyt in advanced carcinoma of the breast: a phase II study". Clinical Radiology. 30 (2): 139–147. doi:10.1016/S0009-9260(79)80133-6. PMID86404.
12Daponte D, Sylvester R, De Pauw M, Fryszman A, Smith RM, Smith PH (August 1983). "Change in white cell count during treatment of advanced cancer of the prostate with estramustine phosphate and with stilboestrol". British Journal of Urology. 55 (4): 408–412. doi:10.1111/j.1464-410X.1983.tb03333.x. PMID6349745.
12Van Poppel H, Werbrouck PW, Baert L (1990). "Effect of estramustine phosphate on free androgens. A comparative study of the effect of orchiectomy and estramustine phosphate on free androgens in patients with prostatic cancer". Acta Urologica Belgica. 58 (4): 89–95. PMID2093302.
123Karr JP, Wajsman Z, Kirdani RY, Murphy GP, Sandberg AA (August 1980). "Effects of diethylstilbestrol and estramustine phosphate on serum sex hormone binding globulin and testosterone levels in prostate cancer patients". The Journal of Urology. 124 (2): 232–236. doi:10.1016/S0022-5347(17)55383-5. PMID7190620.
12Daehlin L, Damber JE, von Schoultz B, Bergman B (August 1986). "The oestrogenic effects of ethinyl oestradiol/polyoestradiol phosphate and estramustine phosphate in patients with prostatic carcinoma. A comparative study of oestrogen sensitive liver proteins, gonadotrophins and prolactin". British Journal of Urology. 58 (4): 412–416. doi:10.1111/j.1464-410X.1986.tb09095.x. PMID3092893.
↑Fredholm, B., Jensen, G., Lindskog, M., & Muntzing, J. (1974, January). Effects of estramustine phosphate (Estracyt) on growth of DMBA-induced mammary tumors in rats. In Acta Pharmacologica et Toxicologica (Vol. 35, pp. 28-28). 35 Norre Sogade, PO Box 2148, DK-1016 Copenhagen, Denmark: Munksgaard Int Publ Ltd.
↑Gunnarsson O, Andersson SB, Johansson SA (1983). "The hydrolysis of estramustine phosphate; in vitro studies". European Journal of Drug Metabolism and Pharmacokinetics. 8 (4): 395–402. doi:10.1007/BF03188772. PMID6673977. S2CID22105700.
12Ozeki T, Takeuchi M, Suzuki M, Kitamura T, Takayanagi R, Yokoyama H, Yamada Y (October 2009). "Single nucleotide polymorphisms of 17beta-hydroxysteroid dehydrogenase type 7 gene: mechanism of estramustine-related adverse reactions?". International Journal of Urology. 16 (10): 836–841. doi:10.1111/j.1442-2042.2009.02374.x. PMID19735314. S2CID38350076.
12Suzuki M, Muto S, Hara K, Ozeki T, Yamada Y, Kadowaki T, etal. (February 2005). "Single-nucleotide polymorphisms in the 17beta-hydroxysteroid dehydrogenase genes might predict the risk of side-effects of estramustine phosphate sodium in prostate cancer patients". International Journal of Urology. 12 (2): 166–172. doi:10.1111/j.1442-2042.2005.01004.x. PMID15733111. S2CID71166897.
↑Gate L, Tew KD (2011). "Alkylating Agents". Cancer Management in Man: Chemotherapy, Biological Therapy, Hyperthermia and Supporting Measures. Cancer Growth and Progression. Springer. pp.61–85. doi:10.1007/978-90-481-9704-0_4. ISBN978-90-481-9703-3.
↑"Estradiol"(PDF). Abbott Laboratories. November 2009. Archived from the original(PDF) on 2021-11-27. Retrieved 2018-09-20.
↑Sweetman, S, ed. (12 February 2013). "Estramustine Sodium Phosphate". Martindale: The Complete Drug Reference. London, UK: Pharmaceutical Press. Retrieved 8 February 2014.
Further reading
Tew KD (September 1983). "The mechanism of action of estramustine". Seminars in Oncology. 10 (3 Suppl 3): 21–26. PMID6364362.
Hoisaeter PA, Bakke A (September 1983). "Estramustine phosphate (Estracyt): experimental and clinical studies in Europe". Seminars in Oncology. 10 (3 Suppl 3): 27–33. PMID6364363.
Sandberg AA (September 1983). "Metabolic aspects and actions unique to Estracyt". Seminars in Oncology. 10 (3 Suppl 3): 3–15. PMID6364364.
Haukaas SA (1984). "Immunological effects of diethylstilbestrol and estramustine phosphate". Scandinavian Journal of Urology and Nephrology. Supplementum. 83: 1–32. PMID6387896.
Sandberg AA (June 1984). "Metabolic parameters of Estracyt pertinent to its effects in prostatic cancer". Urology. 23 (6 Suppl): 11–21. doi:10.1016/S0090-4295(84)80092-8. PMID6375075.
Gunnarsson PO, Forshell GP (June 1984). "Clinical pharmacokinetics of estramustine phosphate". Urology. 23 (6 Suppl): 22–27. doi:10.1016/S0090-4295(84)80093-X. PMID6375076.
Müntzing J, Gunnarsson K (June 1984). "Preclinical pharmacology and toxicology of estramustine phosphate". Urology. 23 (6 Suppl): 6–10. doi:10.1016/S0090-4295(84)80091-6. PMID6375082.
Slack NH, Murphy GP (June 1984). "Clinical toxicity and long-term results of Emcyt therapy for prostate cancer". Urology. 23 (6 Suppl): 73–77. doi:10.1016/S0090-4295(84)80103-X. PMID6375085.
Hedlund PO (1985). "Mode of action of estramustine phosphate in hormone dependent and hormone non-dependent prostate cancer". Progress in Clinical and Biological Research. 185A: 197–202. PMID3898129.
Hedlund PO (1987). "Estracyt--mode of action and clinical experience". Progress in Clinical and Biological Research. 243B: 215–219. PMID3309981.
Murphy GP (1987). "A current review of the clinical experience with Estracyt". Progress in Clinical and Biological Research. 243B: 221–225. PMID3309982.
Forsgren B (1988). "Estramustine-binding protein in rat and human prostate". Scandinavian Journal of Urology and Nephrology. Supplementum. 107: 56–58. PMID3287598.
Tew KD, Stearns ME (1989). "Intracellular effects of estramustine (Estracyt/Emcyt)". Progress in Clinical and Biological Research. 303: 169–175. PMID2674983.
Tew KD, Stearns ME (1989). "Estramustine--a nitrogen mustard/steroid with antimicrotubule activity". Pharmacology & Therapeutics. 43 (3): 299–319. doi:10.1016/0163-7258(89)90012-0. PMID2682681.
Könyves I (1989). "Estramustine phosphate (Estracyt) in the treatment of prostatic carcinoma". International Urology and Nephrology. 21 (4): 393–397. doi:10.1007/BF02559635. PMID2693392. S2CID9727646.
Benson R, Hartley-Asp B (1990). "Mechanisms of action and clinical uses of estramustine". Cancer Investigation. 8 (3–4): 375–380. doi:10.3109/07357909009012056. PMID2207764.
Van Poppel H, Baert L (1991). "The present role of estramustine phosphate in advanced prostate cancer". Progress in Clinical and Biological Research. 370: 323–341. PMID1924466.
Janknegt RA (1992). "Estramustine phosphate and other cytotoxic drugs in the treatment of poor prognostic advanced prostate cancer". The Prostate. Supplement. 4: 105–110. doi:10.1002/pros.2990210516. PMID1574449. S2CID40562112.
Tew KD, Glusker JP, Hartley-Asp B, Hudes G, Speicher LA (December 1992). "Preclinical and clinical perspectives on the use of estramustine as an antimitotic drug". Pharmacology & Therapeutics. 56 (3): 323–339. doi:10.1016/0163-7258(92)90023-S. PMID1301594.
Perry CM, McTavish D (July 1995). "Estramustine phosphate sodium. A review of its pharmacodynamic and pharmacokinetic properties, and therapeutic efficacy in prostate cancer". Drugs & Aging. 7 (1): 49–74. doi:10.2165/00002512-199507010-00006. PMID7579781. S2CID36725810.
Hudes G (February 1997). "Estramustine-based chemotherapy". Seminars in Urologic Oncology. 15 (1): 13–19. PMID9050135.
Kitamura T (February 2001). "Necessity of re-evaluation of estramustine phosphate sodium (EMP) as a treatment option for first-line monotherapy in advanced prostate cancer". International Journal of Urology. 8 (2): 33–36. doi:10.1046/j.1442-2042.2001.00254.x. PMID11240822. S2CID43384150.
Ravery V, Fizazi K, Oudard S, Drouet L, Eymard JC, Culine S, etal. (December 2011). "The use of estramustine phosphate in the modern management of advanced prostate cancer". BJU International. 108 (11): 1782–1786. doi:10.1111/j.1464-410X.2011.10201.x. PMID21756277. S2CID33456591.
This page is based on this Wikipedia article Text is available under the CC BY-SA 4.0 license; additional terms may apply. Images, videos and audio are available under their respective licenses.