Anemia (also spelt anaemia in British English) is a blood disorder in which the blood has a reduced ability to carry oxygen. This can be due to a lower than normal number of red blood cells, a reduction in the amount of hemoglobin available for oxygen transport, or abnormalities in hemoglobin that impair its function.[3][4]
Anemia can also be classified based on the size of the red blood cells and amount of hemoglobin in each cell.[1] If the cells are small, it is called microcytic anemia; if they are large, it is called macrocytic anemia; and if they are normal sized, it is called normocytic anemia.[1] The diagnosis of anemia in men is based on a hemoglobin of less than 130g/L; in non-pregnant women, it is less than 120g/L, while in pregnant women it is less than 105–110.[6][7] Further testing is then required to determine the cause.[1][8]
Treatment depends on the specific cause. Certain groups of individuals, such as pregnant women, can benefit from the use of iron pills for prevention.[1][9]Dietary supplementation, without determining the specific cause, is not recommended.[1] The use of blood transfusions is typically based on a person's signs and symptoms.[1] In those without symptoms, they are not recommended unless hemoglobin levels are less than 60 to 80g/L (6 to 8g/dL).[1][10] These recommendations may also apply to some people with acute bleeding.[1]Erythropoiesis-stimulating agents are only recommended in those with severe anemia.[10]
Anemia is the most common blood disorder, affecting about a fifth to a third of the global population.[1][11][12]Iron-deficiency anemia is the most common cause of anemia worldwide, and affects nearly one billion people.[13] In 2013, anemia due to iron deficiency resulted in about 183,000 deaths – down from 213,000 deaths in 1990.[14] This condition is most prevalent in children[15][16] with also an above average prevalence in elderly[1] and women of reproductive age (especially during pregnancy).[13] Women aged 15 to 49 years experienced an increase in the global prevalence from 27.6% to 30.7% between 2012 to 2023 with either no improvement or an increase in prevalence in nearly all regions.[17] Anemia is one of the six WHO global nutrition targets for 2025 and for diet-related global targets endorsed by World Health Assembly in 2012 and 2013. Efforts to reach global targets contribute to reaching Sustainable Development Goals (SDGs),[18] with anemia as one of the targets in SDG 2 for achieving zero world hunger.[19]
Signs and symptoms
Main symptoms that may appear in anemia
Symptoms of anemia can come on quickly or slowly.[21] If the anemia develops slowly (chronic), the body may adapt and compensate for this change up to a point. In this case, no symptoms may appear until the anemia becomes more severe.[20][22] General symptoms of mild anemia can include feeling tired, weak, dizziness, headaches, shortness of breath, and pale or yellowish skin.[22][23]
The hand of a person with severe anemia (on the left, with ring) compared to the hand of a person without anemia (on the right)
Chronic anemia in infants may result in poor growth and impaired neurological development.[26]
Pallor resulting from severe anemia may be visible in the hand palms and fingernails beds, although it may be difficult to detect in dark toned skin. Other locations to detect pallor are the inner lining of the lower eyelid and the tongue.[27][28][29]
Other symptoms associated with anemia depend on the underlying cause of the disorder; for example -
Chronic iron-deficiency anemia may be associated with symptoms that can include spoon-shaped nails, sore or abnormally smooth tongue, hair loss, or pica (the desire to eat things which are not food, such as ice or earth).[30]
Anemia caused by vitamin B12 deficiency may be associated with psychological problems such as anxiety and confusion, memory loss, and depression.[31]
Diagnosis
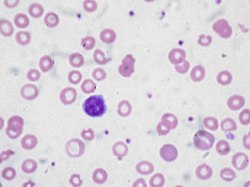
Peripheral blood smear microscopy of a patient with iron-deficiency anemiaA Giemsa-stained blood film from a person with iron-deficiency anemia. This person also had hemoglobin Kenya.
Definitions
There are several definitions of anemia.[32] A strict but broad definition is an absolute decrease in red blood cell mass,[33] however, a broader definition is a lowered ability of the blood to carry oxygen.[34] An operational definition is a decrease in whole-blood hemoglobin concentration of more than 2 standard deviations below the mean of an age- and sex-matched reference range.[35]
World Health Organization Hemoglobin thresholds used to define anemia[36]
Age or gender group
Hb threshold (g/L)
Children (0.5–2 yrs)
105
Children (2–5 yrs)
110
Children (5–12 yrs)
115
Teens (12–15 yrs)
120
Non-pregnant women (>15yrs)
120
Pregnant girls and women
105–110
Men (>15yrs)
130
Etymology
The name is derived from Ancient Greekἀν- (an-)'not' and "αἷμᾰ" (haîmă)'blood'.[37] A related word, ischemia, derives from the Greek from ῐ̓́σχω (ĭ́skhō, “stop”) and αἷμᾰ (haîmă, “blood”); the roots of the both words refer to the basic idea of "lack of blood", but the meaning is significantly different. Anemia implies widespread effects from blood that either is too scarce (e.g., blood loss) or is dysfunctional in its oxygen-supplying ability (due to whatever type of hemoglobin or erythrocyte problem). Ischemia is a restriction in blood supply to any tissue, muscle, or organ of the body, causing a shortage of oxygen that is needed to keep tissues alive, as may occur for example in a stroke.[38][39][40]
Testing
Anemia is typically diagnosed on a complete blood count from a blood sample. An automated hematology analyzer measures the hemoglobin level, hematocrit (% volume of RBCs in the blood), the size of the RBCs,[41] and counts of white blood cells and platelets.
Further tests will be needed to determine the underlying cause; these may include (not a complete list):[42][43]
A count of reticulocytes (immature RBCs), which measures the capacity of the bone marrow to produce new RBCs.[44]
Iron profile, to establish if there is underlying iron deficiency (the most common cause of anemia).[45]
Peripheral blood smear - a small blood sample is examined under a microscope to check the size and shape of RBCs. Among other things, this should detect malaria parasites, which are globally the third most common cause.[46][47]
Figure shows normal red blood cells flowing freely in a blood vessel. The inset image shows a cross-section of a normal red blood cell with normal hemoglobin.
In humans, mature red blood cells (RBCs) are flexible biconcave disks, lacking cell nucleus and organelles. The process by which new RBCs are produced is termed erythropoiesis; committed stem cells in the red bone marrow of large bones take 7 days to mature into red blood cells. Between 2 and 3 million new RBCs are produced per second in human adults.[50] The functional lifetime of a RBC is about 100–120 days, during which time the cells are continually moving within the blood circulation.[51] The aging RBC undergoes changes in its plasma membrane, making it susceptible to recognition by macrophages and subsequent breakdown in the spleen, thus removing old and defective cells and continually purging the blood.[52] This process is termed eryptosis; much of the resulting breakdown products are recirculated in the body.[53] RBC breakdown by eryptosis normally occurs at the same rate as production by erythropoiesis, thus maintaining a balanced RBC population in the circulation.[54]
Aplastic anemia[56] affects all kinds of blood cells. Fanconi anemia is a hereditary disorder or defect featuring aplastic anemia and various other abnormalities, including malformation of the extremities.[57]
Anemia of prematurity, by diminished erythropoietin response to declining hematocrit levels, combined with blood loss from laboratory testing, generally occurs in premature infants at two to six weeks of age.[59]
Myelophthisic anemia or myelophthisis is a severe type of anemia resulting from the replacement of bone marrow by other materials, such as malignant tumors, fibrosis, or granulomas.[56] The term Leukoerythroblastic is applied to a typical blood smear showing immature and abnormal erythrocytes.[64]
Chronic inflammation can disrupt iron handling, limiting its availability for red blood cell formation.[56] In chronic inflammation, the liver produces high levels of hepcidin, a hormone which regulates iron metabolism.[65] This leads to high ferritin levels and low transferrin saturation, a pattern known as "functional iron deficiency." In this condition, iron availability is restricted even when total body iron stores are adequate, contributing to anemia common in inflammatory bowel diseases and chronic infections.[66] This mechanism is commonly seen in older hospitalized patients with long-standing illnesses such as infections, heart failure or autoimmune conditions.[67]
Hereditary spherocytosis[56] is a hereditary defect that results in defects in the RBC cell membrane, causing the erythrocytes to be sequestered and destroyed by the spleen.[76]
Repeated pregnancies and short birth intervals.[66]
Many types of cancers, such as leukemia and multiple myeloma, may cause acute or chronic blood loss.[91]
Anemia caused by medical interventions (Iatrogenic anemia): acute blood loss blood loss from repeated blood draws, surgical procedures, or as a side effect of chemotherapy.[92][93][91]
Fluid overload
Fluid overload (hypervolemia) causes decreased hemoglobin concentration and apparent anemia:[94]
General causes of hypervolemia include excessive sodium or fluid intake, sodium or water retention.[95]
During early pregnancy, hormonal changes trigger an increase in blood plasma volume, while red cell mass increases more slowly. This physiological change dilutes existing RBCs and may trigger a diagnosis of anemia.[66][96]
General global contributors
In many regions, nutritional deficiencies are major drivers of reduced RBC production. Poor intake of iron, folate, and vitamin B12 can significantly impair hemoglobin synthesis and erythropoiesis. This is especially common in low-income populations, areas with limited food diversity, and communities experiencing famine.[66] Socioeconomic factors such as poverty, limited access to nutrient-rich foods, and high rates of parasitic exposure increase the risk of iron-deficiency anemia in women and children.[66]
Pregnancy greatly increases iron requirements, and inadequate dietary intake during pregnancy is one of the leading causes of anemia among reproductive-age women worldwide.[66]
Chronic infections common in developing countries, such as malaria and hookworm disease, impair erythropoiesis either through inflammatory suppression or recurrent blood loss leading to iron depletion.[66]
Classification systems
Anemia is often classified by the size of red blood cells, visible in a peripheral blood smear. The mean corpuscular volume (MCV) of a normal RBC is between 80 and 100 femtoliters. If the cells are smaller than 80 fl, the anemia is said to be microcytic; if they are larger than 100 fl, the anemia is macrocytic. Within the normal range, the anemia is normocytic.[97]
The other principal principle method of classification looks at the balance between erythropoiesis (RBC production in the bone marrow) and eryptosis (RBC breakdown, principally in the spleen). Anemias in which the bone marrow fails to make sufficient RBCs are termed hypoproliferative; included in this group are nutrient deficiencies (e.g. iron, B12, folate), thalassemia, and cancers which affect the bone marrow.[97] When production is normal but there is excessively rapid breakdown of RBCs, the term is hemolytic anemia. This group includes sickle cell anemia, malaria, glucose-6-phosphate dehydrogenase deficiency and some autoimmune conditions such as lupus.[100][101] Acute anemia caused by blood loss - e.g. following injury, surgery or childbirth - doesn't fit into this classification.[102]
Transfusion dependence
Anemia is classified as transfusion-dependent if regular blood transfusions are required to maintain quality of life, or to prevent death.[103] Most people with myelodysplastic syndrome develop this state at some point in time.[104]Beta thalassemia may also result in transfusion dependence.[105][106] Concerns from repeated blood transfusions include iron overload,[104] which may require chelation therapy.[107]
Treatment
In order to treat anemia, the underlying cause and its severity would first need to be identified[5]. Different causes and types of anemia mean there are different treatments. Drugs, for example, are used to treat iron-deficiency anemia, thalassemia, aplastic anemia, hemolytic anemia, sickle cell anemia, and pernicious anemia, with iron-deficiency and sickle cell anemia taking up 60% of market share due to having the highest prevalence as well as highest treatment costs.[108]
More specifically, iron supplements, antibiotics, immunosuppressants, bone marrow stimulants, corticosteroids, gene therapy, and iron chelating agents are forms of anemia treatment drugs, with immunosuppressants and corticosteroids accounting for 58% of the market share.[108] A paradigm shift towards gene therapy and monoclonal antibody therapies is observed.[108] Besides drugs, treatments include replenishing specific deficiencies that may be causing anemia.[5] Vitamin supplements given orally (folic acid or vitamin B12) or intramuscularly (vitamin B12) to replace specific deficiencies.[1] More invasive treatments include blood transfusions, blood or bone marrow transplantation, or even surgery.[4] Otherwise, oxygen may be given, and a dietary change is suggested.[5]
Oral Iron
Iron deficiency results in the decreased production of hemoglobin, the oxygen-carrying protein in red blood cells.[109] In developing nations, an estimated two-thirds of children and women of childbearing age (15-49) are estimated to have iron deficiency without anemia, with one-third of them having an iron deficiency with anemia.[110] Child-bearing women may not have access to certain medications or appropriate nutrition due to socioeconomic factors, which may affect the chances for developing anemia.[111] Iron deficiency due to inadequate dietary iron intake is rare in men and postmenopausal women. In some cases, the diagnosis of iron deficiency mandates a search for potential sources of blood loss, such as gastrointestinal bleeding from ulcers or colon cancer.[110]
Mild to moderate iron-deficiency anemia is treated by oral iron supplementation with ferrous sulfate, ferrous fumarate, or ferrous gluconate.[109] Daily iron supplements are effective in reducing anemia in women of childbearing age.[112] Because these iron supplements are taken orally, gastrointestinal side effects, including stomach upset, vomiting, or darkening of the feces, are commonly experienced.[109] The stomach upset can be alleviated by taking the iron with food; however, this decreases the amount of iron absorbed. Vitamin C aids in the body's ability to absorb iron, so taking oral iron supplements with orange juice is of benefit.[113]
In the anemia of chronic kidney disease, recombinanterythropoietin or epoetin alfa is recommended to stimulate RBC production, and if iron deficiency and inflammation are also present, concurrent parenteral iron is also recommended.[114]
Injectable Iron
In cases where oral iron has either proven ineffective, would be too slow (for example, pre-operatively), or where absorption is impeded (for example, in cases of inflammation), parenteral iron preparations can be used. Parenteral iron can improve iron stores rapidly and is also effective for treating people with postpartum haemorrhage, inflammatory bowel disease, and chronic heart failure.[115] The body can absorb up to 6mg iron daily from the gastrointestinal tract. In many cases, the patient has a deficit of over 1,000mg of iron, which would require several months to replace. This can be given concurrently with erythropoietin to ensure sufficient iron for increased rates of erythropoiesis.[116]
Injectable iron (iron supplement) is available both intravenously and intramuscularly, with IV treatment more common than IM as IM may have inconsistent absorption. Possible side effects of IV iron supplementation include infusion reactions and anaphylaxis, depending on the patient's conditions. Possible side effects of IM iron supplementation include site injection pain and stained skin.[109] Before an individual is given any iron supplements, an extensive workup is performed by a primary healthcare provider. Too much iron can be damaging, and intake is monitored.[109]
Blood transfusions
Blood bag used for blood transfusion
Blood transfusions work to replace blood lost in surgery, injury, or to make up for the blood the body isn't producing. More blood means more hemoglobin and oxygen being carried throughout the body. In this treatment, healthy blood, often voluntarily donated, is provided through an IV line connected to the blood vessels. The healthy blood, before being given, is carefully tested and handled, and further tests are conducted to confirm a match with the patient.[117]
Blood transfusions in those without symptoms is not recommended until the hemoglobin is below 60 to 80g/L (6 to 8g/dL).[1] In those with coronary artery disease who are not actively bleeding transfusions are only recommended when the hemoglobin is below 70 to 80g/L (7 to 8 g/dL).[10] Transfusing earlier does not improve survival.[118] Transfusions otherwise should only be undertaken in cases of cardiovascular instability.[119]
A 2012 review concluded that when considering blood transfusions for anaemia in people with advanced cancer who have fatigue and breathlessness (not related to cancer treatment or haemorrhage), consideration should be given to whether there are alternative strategies that can be tried before a blood transfusion.[120]
A blood transfusion is not without risk. During a blood transfusion, the patient is monitored during and after for any side effects. Even if the donor blood is tested, handled, and matched correctly, patients can still experience reactions ranging from mild (fevers) to severe (alloimmunization). Otherwise, there is a chance of getting too much iron from extensive transfusions and a very slim chance of getting an infectious disease (extensive testing is done).[117]
Bone marrow transplant
Procedure of harvesting blood stem cells for transplantation
Bone marrow is the site for new red blood cell production, and if the bone marrow is unable to produce enough red blood cells, a transplant could be recommended. Aplastic anemia, for example, is the result of bone marrow failing to produce red blood cells.[121] In a bone marrow transplant, old defective bone marrow is destroyed using drugs or radiation and replaced with new stem cells. Before the transplant, like a blood transplant, the bone marrow must be carefully tested and must be compatible. Sometimes, the stem cells can come from the patient themselves (autologous), and other times, the cells will come from a donor (allogenic). The patient is monitored before, during, and after the transplant for any complications.[117]
A bone marrow transplant is an intensive therapy and comes with risks and possible complications. The treatment weakens the immune system and leaves the body weak against possible infections and bleeding, especially while the stem cells get settled and grow into bone marrow.[121] In other cases, there's the risk that the donated stem cells attack the body (graft-versus-host disease) or the patient's body rejects the donated stem cells. Additionally, the patient is likely to be put on medication that could have their own side effects, or experience side effects of the radiation and drugs used to destroy the old bone marrow.[117]
Vitamin B12 intramuscular injections
Pernicious anemia results from a lack of vitamin B12 absorbed. Vitamin B12 is supplemented via intramuscular injection in severe cases or cases of malabsorption of dietary-B12. Pernicious anemia caused by loss of intrinsic factor cannot be prevented.[122] If there are other, reversible causes of low vitamin B12 levels, the cause must be treated.[123]
Vitamin B12 deficiency anemia is usually easily treated by providing the necessary level of vitamin B12 supplementation.[124] The injections are quick-acting, and symptoms usually go away within one to two weeks.[124] As the condition improves, doses are reduced to weeks and then can be given monthly. Intramuscular therapy leads to more rapid improvement and should be considered in patients with severe deficiency or severe neurologic symptoms.[124] Treatment should begin rapidly for severe neurological symptoms, as some changes can become permanent.[125] In some individuals lifelong treatment may be needed.[125]
Erythropoiesis-stimulating agents
Erythropoiesis-stimulating agents (ESA) work to increase endogenous erythropoietin (EPO) production, a hormone that increases the production of red blood cells.[126] The objective for the administration of an ESA is to maintain hemoglobin at the lowest level that both minimizes transfusions and meets the person's needs.[127] They should not be used for mild or moderate anemia.[118] They are not recommended in people with chronic kidney disease unless hemoglobin levels are less than 10 g/dL or they have symptoms of anemia. Their use should be along with parenteral iron.[127][128]
The 2020 Cochrane Anaesthesia Review Group review of erythropoietin (EPO) plus iron versus control treatment including placebo or iron for preoperative anaemic adults undergoing non-cardiac surgery demonstrated that patients were much less likely to require red cell transfusion, and in those transfused, the volumes were unchanged (mean difference -0.09, 95% CI -0.23 to 0.05). Pre-operative hemoglobin concentration was increased in those receiving 'high dose' EPO, but not 'low dose'.[129]
The use of ESAs is heavily monitored by healthcare professionals as dosage and type vary among patients. A baseline for hemoglobin is set prior to treatment and continuously monitored throughout treatment. Risks involve reactions to the ESA and possible overdose if not carefully monitored.[126]
Epidemiology
Anemia affects 24% of the world's population, with iron-deficiency anemia accounting for the majority of cases.[130] Approximately 9.3% of the world population have a moderate degree of anemia, and 0.9% have severe anemia.[131] The proportions of moderate-to-severe anaemia may be higher among hospitalised children in endemic areas.[132][133] Women and girls are more likely to be anemic with a prevalence of 31% compared to 17% for men and boys. The difference is starkest during reproductive years.[130] Women aged 15 to 49 years experienced an increase in the global prevalence from 27.6% to 30.7% between 2012 to 2023 with either no improvement or an increase in prevalence in nearly all regions.[17]
Age-related differences
Anemia is most frequent in older populations, affecting up to ~17% of a cohort of individuals above the age of 65 years old.[134] In neonates (0-6 days old), hemoglobinopathies are the primary contributor to disorders related to anemia, as newborns retain their iron stores they accumulated during pregnancy. As children grow, the causes and patterns of developing anemia shift. Anemia-related disability rate is especially high among children under 5 years old, with boys experiencing slightly higher rates, potentially due to biological differences in iron metabolism.[135]
Population groups at higher risk
Certain populations experience disproportionately higher rates of anemia. For example, African Americans have an elevated risk of developing anemia compared with other racial groups.[136] Severe anaemia is prevalent globally, and especially in sub-Saharan Africa[137] where it is associated with infections including malaria and invasive bacterial infections.[138][139] Children under 5 years old in low-income regions represent a high-risk population, although the age profile might be shifting with declining malaria prevalence in endemic areas[140]. In a survey of 96,804 children across 27 sub-Saharan African countries, nearly 60% were anemic (one of the highest regional burdens worldwide). Socioeconomic and maternal factors accounted for more than two-thirds of this burden, with children from crowded households or communities with inadequate sanitation facing substantially higher risk.[141] Pregnant women also carry an increased risk of developing anemia when infected with malaria.[142] Globally, the prevalence of anaemia in women aged 15 to 49 years increased from 28.5% in 2012 to 29.9% in 2019 and is projected to reach 32.3% by 2030, missing the Sustainable Development Goal target of a 50 percent reduction by 2030.[143]
Signs of severe anemia in human bones from 4000 years ago have been uncovered in Thailand.[144]
The first discovery and discussion of blood was in 1674 when Antoni van Leeuwenhoek described red blood cells (RBCs) as "small round globules." RBCs counterpart, hemoglobin, wasn't discovered until much later by FL Hünefeld in 1840. In 1746, Vincenzo Menghini showed that iron was concentrated in the red blood cells using a magnetic knife[145]. Between 1877-1885, many key tools emerged like hemocytometer (RBC count), hemoglobin measurement, and hematocrit measurement that allowed for quantitative diagnosis of blood[146]. By the 1920s it was confirmed by multiple different studies that iron existed in plasma. McCance and Widdowson showed that iron is not excreted from the body in 1938, and it was later confirmed that iron absorption is the main way the body regulates iron levels. Factors that increase absorption are anemia, hypoxia, and iron depletion, while factors that decrease absorption are transfusions and iron overload.
In ancient cultures, like Assyria and Mediterranean societies, used iron for medical treatments, however, this occurred before iron's biological role was understood. In the 1500s, Nicholas Monarde used iron's "healing powers" to treat gout, acne and hair loss[145]. Anemia started out as a clinical entity in 1807. Early diagnosis of anemia in the early 1800s were based solely on physical examinations such as fatigue, paleness, sweating, difficulty breathing, and dizziness. It wasn't until late in the 1800s when new technologies allowed for a more in depth, lab-based diagnosis on anemia. Also in the 17th and 18th century, water borne parasites may have contributed to the spread of iron deficiency anemia.[147] In 1939, anemia was officially defined as "a deficiency of blood not due to hemorrhage[146]." The term Chlorosis or "green disease" was used in the 17th century and referred to a disease that affected mostly adolescent females with the symptoms of paleness, headaches, loss of appetite, indigestion, and exhaustion. In the late 17th century, Thomas Sydenham advocated for the use of iron as treatment for the disease. The disease mysteriously disappeared, and it was determined that it was likely due to the change in American lifestyles in the early 20th century, such as diminished prejudice or eating meat and abandonment of tight lacing/corsets. The term can not be found in any hematology textbooks, but is generally understood that chlorosis was caused by iron deficiency[145].
↑National Institute for Care and Health Excellence (NICE) (October 2025). "Anaemia - iron deficiency". Clinical Knowledge Summaries. Retrieved December 23, 2025.
↑Bhutta ZA, Das JK, Rizvi A, Gaffey MF, Walker N, Horton S, Webb P, Lartey A, Black RE (August 2013). "Evidence-based interventions for improvement of maternal and child nutrition: what can be done and at what cost?". Lancet. 382 (9890): 452–477. Bibcode:2013Lanc..382..452B. doi:10.1016/S0140-6736(13)60996-4. PMID23746776. S2CID11748341.
123Qaseem A, Humphrey LL, Fitterman N, Starkey M, Shekelle P (December 2013). "Treatment of anemia in patients with heart disease: a clinical practice guideline from the American College of Physicians". Annals of Internal Medicine. 159 (11): 770–779. doi:10.7326/0003-4819-159-11-201312030-00009. PMID24297193. S2CID4712203.
12"Anemia". American Society of Hematology. Retrieved January 9, 2026.
↑"Anemia". Yale Medicine. Retrieved January 9, 2026.
12Killeen RB, Kaur A, Afzal M (2026), "Acute Anemia", StatPearls, Treasure Island (FL): StatPearls Publishing, PMID30725917, retrieved March 21, 2026
↑De Franceschi L, Iolascon A, Taher A, Cappellini MD (July 2017). "Clinical management of iron deficiency anemia in adults: Systemic review on advances in diagnosis and treatment". European Journal of Internal Medicine. 42: 16–23. doi:10.1016/j.ejim.2017.04.018. PMID28528999.
↑"anaemia". Dictionary.com. Archived from the original on July 14, 2014. Retrieved July 7, 2014.
↑Merck & Co. Occlusive Peripheral Arterial Disease, The Merck Manual Home Health Handbook website, revised and updated March 2010. Retrieved March 4, 2012.
↑Bellotto F, Cati A (March 2006). "Anemia ed ischemia miocardica: relazioni ed interferenze" [Anemia and myocardial ischemia: relationships and interferences]. Recenti Progressi in Medicina (in Italian). 97 (3): 153–164. doi:10.1701/121.1312. PMID16700423.
↑Dean L (2005), "Blood and the cells it contains", Blood Groups and Red Cell Antigens [Internet], National Center for Biotechnology Information (US), retrieved March 16, 2026
↑Cotran RS, Kumar V, Fausto N, Robbins SL, Abbas AK (2005). Robbins and Cotran pathologic basis of disease. St. Louis, Mo: Elsevier Saunders. p.637. ISBN978-0-7216-0187-8.
↑Stijlemans B, Guilliams M, Raes G, Beschin A, Magez S, De Baetselier P (August 2007). "African trypanosomosis: From immune escape and immunopathology to immune intervention". Veterinary Parasitology. 148 (1): 3–13. doi:10.1016/j.vetpar.2007.05.005. PMID17560035.
↑Herman TF, Killeen RB, Javaid MU (June 8, 2023), "Heinz Body", StatPearls [Internet], StatPearls Publishing, PMID31869086, retrieved April 7, 2026
↑Gyorkos TW, Gilbert NL, Larocque R, Casapía M (April 2011). "Trichuris and hookworm infections associated with anaemia during pregnancy". Tropical Medicine & International Health. 16 (4): 531–537. doi:10.1111/j.1365-3156.2011.02727.x. PMID21281406. S2CID205391965.
↑Karami M, Chaleshgar M, Salari N, Akbari H, Mohammadi M (July 1, 2022). "Global Prevalence of Anemia in Pregnant Women: A Comprehensive Systematic Review and Meta-Analysis". Maternal and Child Health Journal. 26 (7): 1473–1487. doi:10.1007/s10995-022-03450-1. ISSN1573-6628. PMID35608810.
12Johns Hopkins Medicine. (n.d.). Aplastic anemia. The Johns Hopkins University & Health System. Retrieved October 19, 2025 https://www.hopkinsmedicine.org/kimmel-cancer-center/cancers-we-treat/blood-bone-marrow-cancers/aplastic-anemia
12Aapro MS, Link H (2008). "September 2007 update on EORTC guidelines and anemia management with erythropoiesis-stimulating agents". The Oncologist. 13 Suppl 3 (Supplement 3): 33–36. doi:10.1634/theoncologist.13-S3-33. PMID18458123.
↑Karami M, Chaleshgar M, Salari N, Akbari H, Mohammadi M (July 1, 2022). "Global Prevalence of Anemia in Pregnant Women: A Comprehensive Systematic Review and Meta-Analysis". Maternal and Child Health Journal. 26 (7): 1473–1487. doi:10.1007/s10995-022-03450-1. ISSN1573-6628. PMID35608810.
This page is based on this Wikipedia article Text is available under the CC BY-SA 4.0 license; additional terms may apply. Images, videos and audio are available under their respective licenses.