Gynaecology encompasses preventative care, sexual health and diagnosing and treating health issues arising from the female reproduction system, such as the uterus, vagina, cervix, fallopian tubes, ovaries, and breasts; subspecialties include family planning; minimally invasive surgery; paediatric and adolescent gynaecology; and pelvic medicine and reconstructive surgery. Transgender, intersex and nonbinary individuals can in some instances require gynaecological care.[2]
Etymology
The word gynaecology comes from the oblique stem (γυναικ-) of the Greek word γυνή (gyne) meaning 'woman', and -logia meaning 'study'.[3] Literally translated, it means 'the study of women'.[4][5] Its counterpart is andrology, which deals with medical issues specific to the male reproductive system.[6]
History
Antiquity
The Kahun Gynaecological Papyrus, dated to about 1800 BC, deals with gynaecological diseases, fertility, pregnancy, contraception, etc. The text is divided into thirty-four sections, each dealing with a specific problem and containing diagnosis and treatment; no prognosis is suggested. Treatments are non-surgical, consisting of applying medicines to the affected body part or delivering medicines orally. During this time, the womb was sometimes seen as the source of problems manifesting in other body parts.[7]
Ayurveda, an Indian traditional medical system, also provides details about concepts and techniques related to gynaecology, addressing fertility, childbirth complications, and menstrual disorders among other things.[8][9] These writings provide a post and prenatal care, integrating lifestyle practices, meditations and yoga, and a dietary regime for overall well-being.
The Hippocratic Corpus contains several gynaecological treatises dating to the 5th and 4th centuries BC. Aristotle is another source for medical texts from the 4th century BC with his descriptions of biology primarily found in History of Animals, Parts of Animals, Generation of Animals.[10] The gynaecological treatise Gynaikeia by Soranus of Ephesus (1st/2nd century AD) is extant (together with a 6th-century Latin paraphrase by Muscio, a physician of the same school). He was the chief representative of the school of physicians known as the "methodists."
Middle ages and renaissance period
During the Middle Age midwives dominated women's health concerns through experienced-based knowledge, traditional remedies, and herbal medicines. Midwifery was often regarded unscientific and was challenged with the rise of gynaecology as an official medical field. The Renaissance period, 16th century, brought about a resurgence of classical scientific advancements, including the rise of medical advancements in the field of gynaecology and obstetrics. Figures like Ambroise Pare were imperative in improving obstetrics techniques during this period. Peter Chamberlen developed the forceps, an important surgical tool that transformed childbirth and lessened maternal mortality.[11]
18th, 19th and 20th centuries
As medical institutions continued to expand in the 18th-19th centuries, the authority of midwives was challenged by men who dominated medical professions.[12] The formalization of midwifery training by male doctors and advancements in medical knowledge of women's health and anatomy occurred during this period. Figures such as William Smellie, William Hunter, Paul Zweifel, Franz Karl Naegele, and Carl Crede contributed to the understanding of childbirth and women's health in Europe.[11]
In the early 18th and 19th centuries, in the United States, the field of gyneacology, as with most medical specialities, had ties to black women and therefore slavery. Brothers Henry and Robert Campbell were editors of the first medical journal in the deep south. Henry worked as gynaecologist including on enslaved women, whilst publishing medical case narratives of operations in the journal the brothers edited. This created a conflict of interest.[12] Others, such as Dr. Mary Putnam Jacobi, challenged the exclusion of women from medical education and shifted gynaecology to a scientific practice.[13]
J. Marion Sims is regarded as the father of modern gynaecology.[14] Some of his medical contributions were published, such as development of the Sims' position (1845), the Sims' speculum (1845), the Sims' sigmoid catheter, and gynaecological surgery. He was the first to develop surgical techniques for the repair of vesico-vaginal fistulas (1849), a consequence of protracted childbirth which at the time was without treatment. He founded the first women's hospital in the country in Alabama 1855 and subsequently the Woman's Hospital of New York in 1857. He was elected president of the American Medical Association in 1876. Sims died in 1883.[15] His statue was removed from Central Park, after a unanimous vote in 2018.[16]
Sims' legacy is controversial and debated as he conducted experimental operations on black enslaved women, as recounted in his autobiography.[17][18] In this era, anaesthesia use was novice and considered dangerous. Sims developed his techniques and instruments by operating on women, without anaesthesia.[19][20] The ethical issues this created are discussed in the Journal of Medical Ethics and by academic scholars, some of whom have different opinions in regards to consent and why anaesthesia was not used, whilst showing that white women were also subject to experimental procedures.[21][22] When he left Alabama in 1853, a local newspaper called him "an honor to our state."[23]
In terms of common procedures used within the now recognized specialism of gynaecology, the first hysteroscopy was completed in 1869 by Pantaleoni, to treat an endometrial polyp, using a cystoscope.[24]
Obstetrics and gynaecology were recognized as specialties in the mid-19th century, in the United Kingdom. Specialist societies came into being but it became clear that to become disciplines in their own right a separate college was required. William Fletcher Shaw (Professor of Midwifery at Manchester University) and William Blair-Bell (Professor of Obstetrics at Liverpool University) worked to establish The British College of Obstetricians and Gynaecologists in 1929,[25] this later became the Royal College of Obstetricians and Gynaecologists.[26]
George Nicholas Papanicolaou, from Greece, is credited with discovering the pap smear test, he identified differences in the cytology of normal and malignant cervical cells by viewing swabs smeared on microscopic slides. His first publication of the finding in 1928 went relatively unnoticed. It wasn't until he collaborated with Dr Herbert Traut at an American hospital and they published a book, Diagnosis of Uterine Cancer by the Vaginal Smear that this medical advancement became widely known about.[27] By the 20th century, the American College of Obstetricians and Gynecologists (1951) was founded. There were advances in antiseptic techniques, anaesthesia, and diagnostic tools, which transformed gynaecological care.[28]
Some discrimination continued in the United States with forced sterilizations and eugenic policies that disproportionately targeted minorities. In addition to black women, coerced sterilization was used as a method to restrict perceived undesirable groups from reproducing, such as immigrants, poor people, unmarried mothers, disabled and mentally ill people.[29] Between 1909 and 1979, an estimated 20,000 forced sterilizations occurred in California, primarily in state run mental institutions and prisons.[30] Healthcare later became more focused on the importance of informed consent.[31] Since the 1950's an emphasis on a patients right to choose whether to have treatment or not has existed, albeit with a reliance on those with medical knowledge to advise the best course of treatment. Technological advances have in more recent decades enabled patients themselves to obtain medical information more easily.[32]
In Canada, The Royal College of Physicians and Surgeons did not formally recognize obstetrics & gynaecology as specialist fields until 1957.[33] Obstetrics and gynaecology were considered part of the division of surgery. During the 1940's, practitioners focused on obstetrics and gynaecology began identifying the need for a separate organization to deal with this specialism and the idea to form the Society of Obstetricians and Gynaecologists of Canada (SOGC) was conceived.[34]
Ian Donald, a gynaecologist from the United Kingdom was an early pioneer of the use of sonography within gyneacology and obstetrics. He gained knowledge of radar technology in the air force and working with an engineer called Tom Brown and an engineering company, they developed a compact 2D ultrasound machine. In 1958, he published a paper in the Lancet.[35]
Women like Margaret Sanger dedicated themselves to making contraception legal and available. She had worked as a nurse caring for women who had illegal abortions, this created a desire to engage in later activism related to birth control. In 1951 she met Gregory Pincus, a human reproduction medical expert who worked to create a contraceptive pill. She also found a sponsor for the project and trials, Katharine McCormick.[36]
The trials for birth control were controversial for a number of reasons. In 1954, due to anti-birth control laws, the first trials in Massachusetts were positioned as being fertility trials. Gregory Pincus and John Rock conducted these trials. Oral progesterone was tested on fertility patients, with consent, however the oral contraceptive was also tested on 28 psychiatric patients (male and female) at Worcester State Hospital. No direct consent was given by these people, instead relatives gave consent on their behalf. They discovered that women stopped ovulating and that this occurred only whilst taking this. To get FDA approval, a larger clinical trial was needed.[37]
To expand this research, further clinical trials of took place in Puerto Rico, a territory of the United States. Puerto Rico was densely populated with significant poverty, had no anti-birth control laws and already had services offering birth control. Trials began in Rio Piedras in 1956, and women were offered the pill, called Envoid in 1960, on the basis it prevented pregnancy but without knowing it did not have FDA approval. Three women died in the trial and criticisms include that side effects were not taken as seriously as they should have been.[38][39][40] Dr. Edris Rice-Wray, a professor at the Puerto Rico Medical School was aware and vocal of the negative side effects of the pill.[41] Although these trials did not follow modern medical ethical practices, they spearheaded the development of the first oral contraceptive.
Diagnosis
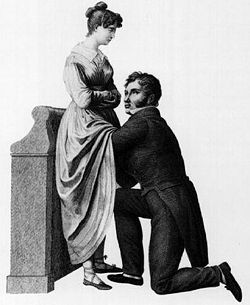
The historic taboo associated with the examination of female genitalia has long inhibited the science of gynaecology. This 1822 drawing by Jacques-Pierre Maygrier shows a "compromise" procedure, in which the physician is kneeling before the woman but cannot see her genitalia. Modern gynaecology no longer uses such a position.
In some countries or within some healthcare systems, women must first see a general practitioner or family practitioner before seeing a gynaecologist. If the condition cannot be diagnosed or treated and requires a specialist the patient is referred to a gynaecologist.[43] In other countries, patients can see a gynaecologist without a referral.[44]
Gynecologists[45] give reproductive and sexual health services that include pelvic exams, Pap tests, cancer screenings, treatment for hormone imbalance, and testing and treatment for vaginal infections.
They diagnose and treat reproductive system disorders such as endometriosis, infertility, ovarian cysts, and pelvic pain. They may also care for people with ovarian, cervical, and other reproductive cancers.
As with all of medicine, the main tools of diagnosis are clinical history, examination and investigations.[46] Gynaecological examination is quite intimate, more so than a routine physical exam. It can also require instruments such as the speculum. The speculum is used to retract the tissues of the vagina to allow examination of the cervix, the lower part of the uterus located within the upper portion of the vagina. Gynaecologists may do a bimanual examination (one hand on the abdomen and one or two fingers in the vagina) to palpate the cervix, uterus, ovaries and pelvis.[47] It is not uncommon to do a rectovaginal examination for a complete evaluation of the pelvis, particularly if any suspicious masses are suspected. Gynaecologists may have a chaperone for their examination or a patient can request this.
An abdominal or vaginal ultrasound can be used for diagnostic purposes. This can help to detect growths, such as polyps, endometrial hyperplasia, carcinoma, endometriosis, pelvic inflammatory disease, polycystic ovary syndrome and many other gynaecology conditions. This is a very common diagnostic tool.[48]
Hormone tests can be useful when investigating gynaecology based conditions or symptoms. These may check the hormone levels of oestradiol, progesterone, follicle stimulating hormone and luteinizing hormones, for example. Levels considered not normal, could indicate the presence of conditions and could impact reproductive function.[49]
Conditions and diseases
"List of reproductive issues" redirects here. For ethical issues, see Bioethics.
Some of these conditions are dealt with by doctors with specialisms other than, or in addition to, gynaecology. For example, a woman with urinary incontinence may be referred to a doctor with urology specialist experience[63] and someone with cancer may be treated by a multidisciplinary team with specialist oncology experience.[64]
Treatments
Surgeries
Gynaecologists may employ medical and/or surgical treatments, depending on the medical condition they are treating. Pre- and post-operative medical management often employs drug therapies, such as antibiotics, diuretics, antihypertensives, and antiemetics. Additionally, gynaecologists make frequent use of specialized hormone-modulating therapies (such as Clomifene citrate and hormonal contraception) to treat disorders of the female genital tract that are responsive to pituitary or gonadal signals.
Surgery is commonly used to treat gynaecology conditions. In the past, gynaecologists were not considered "surgeons", although this point has always been the source of controversy. Modern advancements in general surgery and gynaecology, have blurred the lines of distinction. The rise of sub-specialties within gynaecology which are primarily surgical in nature (for example urogynaecology and gynaecological oncology) have strengthened the reputations of gynaecologists as surgical practitioners, and many surgeons and surgical societies have come to view gynaecologists as peers. Gynaecologists are now eligible for fellowship in both the American College of Surgeons and Royal Colleges of Surgeons, and many newer surgical textbooks include chapters on (at least basic) gynaecological surgery.
Some of the more common operations that gynaecologists perform include:[65]
Dilation and curettage (removal of the uterine contents for various reasons, including completing a partial miscarriage and diagnostic sampling for dysfunctional uterine bleeding refractive to medical therapy)[66]
Laparoscopy – minimally invasive surgery used to diagnose or treat a variety of conditions.[73] Laparoscopy can accurately diagnose pelvic/abdominal endometriosis,[74] more recently non-operative methods have been used for endometriosis diagnosis[75]
Laparotomy– may be used to investigate the level of progression of benign or malignant disease, or to assess and repair damage to the pelvic organs[76][77]
Various surgical treatments for urinary incontinence and pelvic prolapse, including mid-urethral mesh sling procedures[78]
Cervical Excision Procedures (including cryosurgery)– removal of the surface of the cervix containing pre-cancerous cells which have been previously identified on Pap smear.
Non-surgical treatments
Tranexamic acid has been found to be an effective drug to reduce the amount of bleeding during menstruation and medical procedures, so can be used to treat menorrhagia.[79] Hormone based IUDs, such as Mirena have also been shown to help reduce heavy periods.[80]
There are an increasing number of non-surgical treatments available to help uterine fibroids, along with tranexamic acid and progesterone releasing IUSs, such as contraceptive steroid hormones, gonadotropin releasing hormone (GnRH) agonists and antagonists with and without additional hormones, and selective progesterone receptor modulator (SPRM). Organizations such as the American College of Obstetricians and Gynecologists (ACOG) advocate such treatments before surgical intervention, but studies reveal many women who had a hysterectomy between 2011 and 2019 did not receive any other treatments before this.[81]
Hormonal therapy can be used as a non-surgical treatment for endometriosis. Research shows gonadotropin-releasing hormone (GnRH) antagonists, like elagolix, can give encouraging results in managing some symptoms. Also encouraging is research on aromatase inhibitors, such as letrozole that has shown efficacy in reducing lesion size and pain severity.[82] Overall, more recent research shows a trend of new non-surgical treatments becoming available for a number of common gynaecology conditions.
Recent discoveries
Newer advancements in gynaecology are using integration of artificial intelligence (AI) in clinical practice, specifically with diagnostics and predictive analytics. AI algorithms are able to interpret complex gynaecological imaging and pathology data, which improves diagnostic accuracy. These technologies are especially used in identifying cervical and ovarian cancers and predicting treatment outcomes.[83]
Liquid biopsy is emerging as an important noninvasive tool to detect and monitor gynaecology cancers. Tumour-derived biomarkers, such as circulating tumour DNA (ctDNA), circulating tumour cells (CTCs), exosomes and microRNA, can provide insights into the biological behaviour of gynaecology cancers. Some believe this could revolutionize cancer treatment, assisting with earlier detection and predicting disease recurrence but as of 2025, it is not widely used in clinical practice.[84]
In terms of surgery, research has led to minimally invasive approaches, such as vaginal natural orifice transluminal endoscopic surgery. This technique allows surgeons to access the pelvic cavity through the vaginal canal, reducing recovery times, postoperative pain, and complication rates in comparison to traditional methods.[85]
In the United Kingdom, the Royal College of Obstetricians and Gynaecologists, based in London, encourages the study and advancement of both the science and practice of obstetrics and gynaecology. This is done through postgraduate medical education and training development, and the publication of clinical guidelines and reports on aspects of the specialty and service provision. The RCOG International Office works with other international organizations to help lower maternal morbidity and mortality in under-resourced countries.[86]
In the United States, obstetrics and gynaecology requires residency training for four years. This encompasses comprehensive clinical and surgical education. OBGYN residents participate in a yearly in-training exam that is administered by the Council on Resident Education in Obstetrics and Gynecology (CREOG). Research suggests that combining curriculum and focused mentorship can improve residents' performance on the exam and overall educational outcomes.[87]
Gynaecologic oncology is a subspecialty of gynaecology, dealing with gynaecology-related cancer.[88] To become a gynaecology oncologist requires specialist further training.[89]Urogynaecology is also a subspecialty of gynaecology and urology.[63] Further fellowship training is needed to become a urogynaecologist.[90]
Gender of physicians
Improved access to education and the professions in recent decades has seen women gynaecologists outnumber men in the once male-dominated medical field of gynaecology.[91] In some gynaecological sub-specialties, where an over-representation of males persists, income discrepancies appear to show male practitioners earning higher averages.[92]
Speculations on the decreased numbers of male gynaecologist practitioners report a perceived lack of respect from within the medical profession, limited future employment opportunities and questions to the motivations and character of men who choose the medical field concerned with female sexual organs.[93][94][95][96][97]
Surveys of women's views on the issue of male doctors conducting intimate examinations show a large and consistent majority found it uncomfortable, were more likely to be embarrassed and less likely to talk openly or in detail about personal information, or discuss their sexual history with a man. The findings raised questions about the ability of male gynaecologists to offer quality care to patients.[98] This, when coupled with more women choosing female physicians[99] has decreased the employment opportunities for men choosing to become gynaecologists.[100]
According to one source, "there is a sharp decline in the number of men opting for OB/GYN residency programs and general OB/GYN programs due to the sexist market trends. Female OB/GYN physicians are preferred over males by certain employers due to preference given to the female physicians by health care seekers."[101]
In the United States, it has been reported that four in five students choosing a residency in gynaecology are now female.[102] In several places in Sweden, to comply with discrimination laws, patients may not choose a doctor—regardless of specialty—based on factors such as gender and declining to see a doctor because of their gender may legally be viewed as refusing care.[103][104] In Turkey, due to patient preference to be seen by another female, there are now few male gynaecologists working in the field.[105]
There have been a number of legal challenges in the US against healthcare providers who have started hiring based on the gender of physicians. Mircea Veleanu argued, in part, that his former employers discriminated against him by accommodating the wishes of female patients who had requested female doctors for intimate exams.[106] A male nurse complained about an advert for an all-female obstetrics and gynaecology practice in Columbia, Maryland, claiming this was a form of sexual discrimination.[107] In 2000, David Garfinkel, a New Jersey-based OB-GYN, sued his former employer[108] after being fired due to, as he claimed, "because I was male, I wasn't drawing as many patients as they'd expected".[106]
Subsequent to research, some organizations such as the Royal College of Obstetricians and Gynaecologists have called on global governments and international health bodies to address the impact of benign gynaecology conditions in low and middle income countries. They found the years lost to disability from these conditions was greater than combined morbidity from malaria, TB and HIV/AIDS, accounting for 8% of all years lost to disability, for women aged 15–49. They argue that such conditions are neglected within the global health arena and have a significant impact on women in low and middle income countries.[109]
Some benign and common gynaecology conditions have been found to disproportionately impact certain racial and ethnic groups. One study found that black women are three times more likely than white women, to have uterine fibroids, a variety of studies found they are more likely to get these at a younger age and are more likely to have numerous and rapid growing fibroids. This may be due to biological, lifestyle, environmental and clinical factors, further research is needed to understand why this disparity exists. In regards to endometriosis, some research suggests this disproportionately impacts asian women, with black and hispanic women less likely to have this condition. Research about this is somewhat inconsistent suggesting further studies would be beneficial.[110]
In the United States, health disparities persist in gynaecology, disproportionately affecting women of colour, low-income women, and those living in rural areas.[111] Black women face higher rates of mortality from some gynaecology based cancers. The reasons for these disparities is complex and involves racial, economic, educational and geographic factors that influence treatment and survival. Importantly, a variation from evidenced-based treatment has been indicated as a modifiable factor that can effect survival outcomes. This problem disproportionately impacts black women and poorer women. These disparities are compounded by barriers such as lack of insurance and best practice not being followed, particularly when funded by Medicaid.[112]
Some research in the United States shows that hispanic women had a more favourable prognosis compared to non-hispanic women, in regards to certain gynaecology based cancers. With ovarian cancer black women tended to present with more advanced ovarian cancer compared to white women, so were diagnosed at a later stage. The incidence rates of endometrial and ovarian cancer was highest in white women and the incidence of cervical cancer was highest in black women. Research showed that black and hispanic women were less likely to complete the full number of HPV vaccinations, the cause of some gynaecology based cancers.[112] Marginalized groups are less likely to have their pain and symptoms taken seriously by providers, leading to delayed diagnoses and worse outcomes.[113] Addressing these disparities requires having physicians practice cultural humility and physician's addressing their possible bias.[111]
Research from the United States shows that disabled women are screened less for cervical cancer and less likely to have pelvic examinations. They report lower levels of receiving family planning services. Health service usage and whether or not they have insurance did not explain differences in screening levels. Research showed they were less likely to receive doctors recommendations.[114] Women with disabilities also have a greater chance of dying from cervical cancer in counties such as South Korea and Sweden.[115]
In the United Kingdom, in regards to ovarian cancer socioeconomic factors appear to create a disparity in treatment and outcomes. Delays and treatment inequalities may contribute to worse outcomes for women from more deprived areas, with them less likely to receive surgery or chemotherapy. How wealthy a woman is, directly impacted mortality rates.[116] Cervical screening attendance, which helps to diagnose cervical cancer at an early stage has declined, particularly among minority ethnic groups and in more deprived areas. Medical bias in doctor and patient interactions can cause delays to diagnosis and can stem from subconscious stereotypes, in relation to ethnicity or socioeconomic status.[117]
The LGBTQ+ community also face health disparities within gyneacology care. Nearly one in five lesbian and bisexual women have never attended cervical screening. Transexual men and non binary people with a cervix are also less likely to access cervical screening.[118] Research has shown that 22.8% of transgender people avoid accessing healthcare due to anticipated discrimination.[119] Gyneacologists play an important role in caring for transgender patients, who face barriers within health care, as a result of marginalization and discrimination.[120]
Indigenous women in Australia are more likely to die from gynaecology cancers. Research suggests that strategies to reduce survival disparities should target earlier diagnosis and earlier treatment, as aboriginal women were more likely to present with more advanced cancer at the point of diagnosis and decline treatment.[121] Research in Australia examined the issue of pelvic floor dysfunction in aboriginal women, in New South Wales. This showed a high burden of disease and that there was a reluctance of these women to seek care, due to fear of judgement and embarrassment. The authors concluded that culturally appropriate and tailored care was needed to tackle this.[36]
↑Dixon, Laurinda S. (1995). Perilous Chastity: Women and Illness in Pre-Enlightenment Art and Medicine. Cornell University Press. p.15f. ISBN978-0-8014-3026-8.
↑Dean-Jones, Lesley (2003). "The Cultural Construct of the Female Body in Classical Greek Science". Sex and Difference in Ancient Greece and Rome. pp.183–201. doi:10.1515/9781474468541-014. ISBN978-1-4744-6854-1.
12Owens, Deirdre Cooper (2017). Medical Bondage Race, Gender, and the Origins of American Gynecology. Athens: University of Georgia Press (published 15 November 2017). pp.15–18. ISBN978-0-8203-5303-6.
↑Morantz-Sanchez, R. (1985). Sympathy and Science: Women Physicians in American Medicine. Oxford University Press.
↑"The story of my life". Library of Congress, Washington, D.C. 20540 USA. Retrieved 24 March 2025.
↑Cooper Owens, Deirdre Benia (2018). Medical bondage: race, gender, and the origins of American gynecology (Paperbacked.). Athens: The University of Georgia Press. ISBN978-0-8203-5475-0.
↑Russ, Joanna; Daly, Mary (1979). "Gyn/Ecology: The Metaethics of Radical Feminism". Frontiers: A Journal of Women Studies. 4 (1): 68. doi:10.2307/3346672. ISSN0160-9009. JSTOR3346672.
↑Moore, Jessica F.; Carugno, Jose (6 April 2025), "Hysteroscopy", StatPearls, Treasure Island (FL): StatPearls Publishing, PMID33232015, retrieved 19 August 2025
↑Balogh, Erin P.; Miller, Bryan T.; Ball, John R.; Care, Committee on Diagnostic Error in Health; Services, Board on Health Care; Medicine, Institute of; The National Academies of Sciences, Engineering (29 December 2015), "The Diagnostic Process", Improving Diagnosis in Health Care, National Academies Press (US), retrieved 13 April 2025
↑Long, W. Newton (1990), Walker, H. Kenneth; Hall, W. Dallas; Hurst, J. Willis (eds.), "Pelvic Examination", Clinical Methods: The History, Physical, and Laboratory Examinations (3rded.), Boston: Butterworths, ISBN978-0-409-90077-4, PMID21250129, retrieved 13 April 2025{{citation}}: CS1 maint: work parameter with ISBN (link)
↑Cooper, Danielle B.; Menefee, Gary W. (2025), "Dilation and Curettage", StatPearls, Treasure Island (FL): StatPearls Publishing, PMID33760550, retrieved 21 August 2025
↑Don, Emma E.; Mijatovic, Velja; van Eekelen, Rik; Huirne, Judith A. F. (November 2023). "The effect of myomectomy on reproductive outcomes in patients with uterine fibroids: A retrospective cohort study". Reproductive Biomedicine Online. 45 (5): 970–978. doi:10.1016/j.rbmo.2022.05.025. ISSN1472-6491. PMID36041962.
↑Minalt, Nicole; Canela, Christinne D.; Marino, Sarah (11 September 2024), "Endometrial Ablation", StatPearls, Treasure Island (FL): StatPearls Publishing, PMID29083707, retrieved 21 August 2025
↑Sufriyana, H., Wu, Y. W., Su, E. C. Y. (2024). Artificial Intelligence–Assisted Gynecology: Emerging Applications and Future Directions. Journal of Clinical Medicine, 13(4), 1061. https://doi.org/10.3390/jcm13041061
↑Dückelmann, A. M., & Maia, L. (2023). vNOTES in Modern Gynecology: A Review of Current Evidence and Outcomes. Healthcare, 13(7), 720. https://doi.org/10.3390/healthcare13070720
↑Gerber, Susan E.; Lo Sasso, Anthony T. (November 2006). "The evolving gender gap in general obstetrics and gynecology". American Journal of Obstetrics and Gynecology. 195 (5): 1427–1430. doi:10.1016/j.ajog.2006.07.043. PMID17074550.
↑Hall Judith A, Roter Debra L (2 December 2002). "Do patients talk differently to male and female physicians?: A meta-analytic review". Patient Education and Counseling. 48 (3): 217–224. doi:10.1016/S0738-3991(02)00174-X. PMID12477606.
↑Schnatz, Peter F.; Murphy, Jessica L.; O'Sullivan, David M.; Sorosky, Joel I. (November 2007). "Patient choice: comparing criteria for selecting an obstetrician-gynecologist based on image, gender, and professional attributes". American Journal of Obstetrics and Gynecology. 197 (5): 548.e1–548.e7. doi:10.1016/j.ajog.2007.07.025. PMID17980206.
↑Trysell, Katrin (11 April 2018). "Byta doktor ingen rättighet"[Switching Doctor Not a Right]. Läkartidningen (in Swedish). Archived from the original on 26 April 2018. Retrieved 25 April 2018.
Rowland, Beryl, ed. (1981). Medieval Woman's Guide to Health: The First English Gynecological Handbook. Kent, OH: Kent State University Press. ISBN978-0-87338-243-4.
This page is based on this Wikipedia article Text is available under the CC BY-SA 4.0 license; additional terms may apply. Images, videos and audio are available under their respective licenses.