
The clitoris is a female sex organ present in mammals, ostriches and a limited number of other animals. In humans, the visible portion – the glans – is at the front junction of the labia minora, above the opening of the urethra. Unlike the penis, the male homologue (equivalent) to the clitoris, it usually does not contain the distal portion of the urethra and is therefore not used for urination. In most species, the clitoris lacks any reproductive function. While few animals urinate through the clitoris or use it reproductively, the spotted hyena, which has an especially large clitoris, urinates, mates, and gives birth via the organ. Some other mammals, such as lemurs and spider monkeys, also have a large clitoris.

Orgasm or sexual climax is the sudden discharge of accumulated sexual excitement during the sexual response cycle, resulting in rhythmic, involuntary muscular contractions in the pelvic region characterized by sexual pleasure. Experienced by males and females, orgasms are controlled by the involuntary or autonomic nervous system. They are usually associated with involuntary actions, including muscular spasms in multiple areas of the body, a general euphoric sensation and, frequently, body movements and vocalizations. The period after orgasm is typically a relaxing experience, attributed to the release of the neurohormones oxytocin and prolactin as well as endorphins.
Sexual desire is an emotion and motivational state characterized by an interest in sexual objects or activities, or by a drive to seek out sexual objects or to engage in sexual activities. It is an aspect of sexuality, which varies significantly from one person to another and also fluctuates depending on circumstances.
The Masters and Johnson research team, composed of William H. Masters and Virginia E. Johnson, pioneered research into the nature of human sexual response and the diagnosis and treatment of sexual disorders and dysfunctions from 1957 until the 1990s.
Anorgasmia is a type of sexual dysfunction in which a person cannot achieve orgasm despite adequate stimulation. Anorgasmia is far more common in females than in males and is especially rare in younger men. The problem is greater in women who are post-menopausal. In males, it is most closely associated with delayed ejaculation. Anorgasmia can often cause sexual frustration.
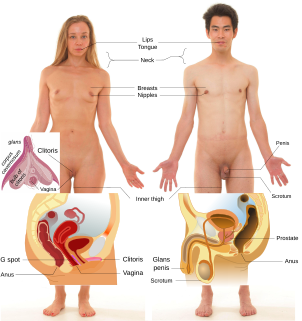
An erogenous zone is an area of the human body that has heightened sensitivity, the stimulation of which may generate a sexual response, such as relaxation, sexual fantasies, sexual arousal and orgasm.
Sexual stimulation is any stimulus that leads to, enhances and maintains sexual arousal, and may lead to orgasm. Although sexual arousal may arise without physical stimulation, achieving orgasm usually requires physical sexual stimulation.
Persistent genital arousal disorder (PGAD), previously called persistent sexual arousal syndrome, is spontaneous, persistent, unwanted and uncontrollable genital arousal in the absence of sexual stimulation or sexual desire, and is typically not relieved by orgasm. Instead, multiple orgasms over hours or days may be required for relief.
Hypoactive sexual desire disorder (HSDD), hyposexuality or inhibited sexual desire (ISD) is sometimes considered a sexual dysfunction, and is characterized as a lack or absence of sexual fantasies and desire for sexual activity, as judged by a clinician. For this to be regarded as a disorder, it must cause marked distress or interpersonal difficulties and not be better accounted for by another mental disorder, a drug, or some other medical condition. A person with ISD will not start, or respond to their partner's desire for, sexual activity. HSDD affects approximately 10% of all pre-menopausal women in the United States, or about 6 million women.
Sexual dysfunction is difficulty experienced by an individual or partners during any stage of normal sexual activity, including physical pleasure, desire, preference, arousal, or orgasm. The World Health Organization defines sexual dysfunction as a "person's inability to participate in a sexual relationship as they would wish". This definition is broad and is subject to many interpretations. A diagnosis of sexual dysfunction under the DSM-5 requires a person to feel extreme distress and interpersonal strain for a minimum of six months. Sexual dysfunction can have a profound impact on an individual's perceived quality of sexual life. The term sexual disorder may not only refer to physical sexual dysfunction, but to paraphilias as well; this is sometimes termed disorder of sexual preference.
The human sexual response cycle is a four-stage model of physiological responses to sexual stimulation, which, in order of their occurrence, are the excitement, plateau, orgasmic, and resolution phases. This physiological response model was first formulated by William H. Masters and Virginia E. Johnson, in their 1966 book Human Sexual Response. Since that time, other models regarding human sexual response have been formulated by several scholars who have criticized certain inaccuracies in the human sexual response cycle model.
Sexual arousal disorder is characterized by a lack or absence of sexual fantasies and desire for sexual activity in a situation that would normally produce sexual arousal, or the inability to attain or maintain typical responses to sexual arousal. The disorder is found in the DSM-IV. The condition should not be confused with a sexual desire disorder.
Female sexual arousal disorder (FSAD) is a disorder characterized by a persistent or recurrent inability to attain sexual arousal or to maintain arousal until the completion of a sexual activity. The diagnosis can also refer to an inadequate lubrication-swelling response normally present during arousal and sexual activity. The condition should be distinguished from a general loss of interest in sexual activity and from other sexual dysfunctions, such as the orgasmic disorder (anorgasmia) and hypoactive sexual desire disorder, which is characterized as a lack or absence of sexual fantasies and desire for sexual activity for some period of time.

Lesbian sexual practices are sexual activities involving women who have sex with women, regardless of their sexual orientation. A woman who has sex with another woman may identify as a lesbian if she is sexually attracted to women, or bisexual if she is not exclusively sexually attracted to women, or dispense with sexual identification altogether. The term may also be applied to a heterosexual or asexual woman who is unsure of or is exploring her sexuality.
Human sexuality is the way people experience and express themselves sexually. This involves biological, psychological, physical, erotic, emotional, social, or spiritual feelings and behaviors. Because it is a broad term, which has varied with historical contexts over time, it lacks a precise definition. The biological and physical aspects of sexuality largely concern the human reproductive functions, including the human sexual response cycle.

Human female sexuality encompasses a broad range of behaviors and processes, including female sexual identity and sexual behavior, the physiological, psychological, social, cultural, political, and spiritual or religious aspects of sexual activity. Various aspects and dimensions of female sexuality, as a part of human sexuality, have also been addressed by principles of ethics, morality, and theology. In almost any historical era and culture, the arts, including literary and visual arts, as well as popular culture, present a substantial portion of a given society's views on human sexuality, which include both implicit (covert) and explicit (overt) aspects and manifestations of feminine sexuality and behavior.
Alcohol and sex deals with the effects of the consumption of alcohol on sexual behavior. The effects of alcohol are balanced between its suppressive effects on sexual physiology, which will decrease sexual activity, and its suppression of psychological inhibitions, which may increase the desire for sex.

Although spinal cord injury (SCI) often causes sexual dysfunction, many people with SCI are able to have satisfying sex lives. Physical limitations acquired from SCI affect sexual function and sexuality in broader areas, which in turn has important effects on quality of life. Damage to the spinal cord impairs its ability to transmit messages between the brain and parts of the body below the level of the lesion. This results in lost or reduced sensation and muscle motion, and affects orgasm, erection, ejaculation, and vaginal lubrication. More indirect causes of sexual dysfunction include pain, weakness, and side effects of medications. Psycho-social causes include depression and altered self-image. Many people with SCI have satisfying sex lives, and many experience sexual arousal and orgasm. People with SCI may employ a variety of adaptations to help carry on their sex lives healthily, by focusing on different areas of the body and types of sexual acts. Neural plasticity may account for increases in sensitivity in parts of the body that have not lost sensation, so people often find newly sensitive erotic areas of the skin in erogenous zones or near borders between areas of preserved and lost sensation.

Nipple stimulation or breast stimulation is stimulation of the breast. Stimulation may be by breastfeeding, sexual activity, or an indirect non-sexual response. As part of sexual activity, the practice may be performed upon, or by, people of any gender or sexual orientation. It may occur with the use of fingers, orally, such as by sucking or licking, as well as by use of an object.

Meredith L. Chivers is a Canadian sexologist and clinical psychologist noted for her research on female sexuality, sexual orientation, paraphilias, sex differences, gender identity, and the physiology of sexual arousal. She is an associate professor in the Department of Psychology at Queen's University in Kingston, Ontario, Canada.



