The progesterone receptor (PR), also known as NR3C3 or nuclear receptor subfamily 3, group C, member 3, is a protein found inside cells. It is activated by the steroid hormone progesterone.
In humans, PR is encoded by a single PGRgene residing on chromosome 11q22,[5][6][7] it has three isoforms: PR-A, PR-B, and PR-C. Though PR-A and PR-B are much more well studied compared to PR-C.[8][9][10] The PR-B is the positive regulator of the effects of progesterone, while PR-A serve to antagonize the effects of PR-B.[11]
Mechanism
Progesterone is necessary to induce activation of the progesterone receptors. When no binding hormone is present the carboxyl terminal inhibits transcription. Binding to a hormone induces a structural change that removes the inhibitory action. Progesterone antagonists prevent the structural reconfiguration.
After progesterone binds to the receptor, restructuring with dimerization follows and the complex enters the nucleus and binds to DNA. There transcription takes place, resulting in formation of messenger RNA that is translated by ribosomes to produce specific proteins.
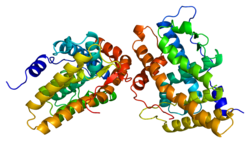
In common with other steroid receptors, the progesterone receptor has a N-terminal regulatory domain, a DNA binding domain, a hinge section, and a C-terminal ligand binding domain. A special transcription activation function (TAF), called TAF3, is present in the progesterone receptor-B, in a B-upstream segment (BUS) at the amino acid terminal. This segment is not present in the receptor-A.
The single-copy human (hPR) gene uses separate promoters and translational start sites to produce three isoforms, PR-A, -B, and -C. PR-A and -B are identical except for an additional 165 amino acids present only in the N terminus of PR-B.[12] PR-C is even smaller, starting at the 595th amino acid of PR-B.[9] Although the three isoforms share many important structural domains, they are functionally distinct.
PR-A and PR-B are disticnt transcription factors, which mediate their own response genes and physiological effects with little overlap.
PR-C being the smallest, does not have the important AF1, AF3, or DNA-binding domains. Thus, PR-C is not a transcription factor. However, PR-C can dimerize, participate in nuclear translocation, and modulate the actions of PR-A and PR-B.[9]
Selective ablation of PR-A in a mouse model, resulting in exclusive production of PR-B, unexpectedly revealed that PR-B contributes to, rather than inhibits, epithelial cell proliferation both in response to estrogen alone and in the presence of progesterone and estrogen. These results suggest that in the uterus, the PR-A isoform is necessary to oppose estrogen-induced proliferation as well as PR-B-dependent proliferation.
Functional polymorphisms
Six variable sites, including four polymorphisms and five common haplotypes have been identified in the human PR gene .[13] One promoter region polymorphism, +331G/A, creates a unique transcription start site. Biochemical assays showed that the +331G/A polymorphism increases transcription of the PR gene, favoring production of hPR-B in an Ishikawa endometrial cancer cell line.[14]
Several studies have now shown no association between progesterone receptor gene +331G/A polymorphisms and breast or endometrial cancers.[15][16] However, these follow-up studies lacked the sample size and statistical power to make any definitive conclusions, due to the rarity of the +331A SNP. It is currently unknown which if any polymorphisms in this receptor are of significance to cancer. A study of 21 non-European populations identified two markers within the PROGINS haplotype of the PR gene as positively correlated with ovarian and breast cancer.[17]
During rodent perinatal life, progesterone receptor (PR) is known to be transiently expressed in both the ventral tegmental area (VTA) and the medial prefrontal cortex (mPFC) of the mesocortical dopaminergic pathway. PR activity during this time period impacts the development of dopaminergic innervation of the mPFC from the VTA. If PR activity is altered, a change in dopaminergic innervation of the mPFC is seen and tyrosine hydroxylase (TH), the rate-limiting enzyme for dopamine synthesis, in the VTA will also be impacted. TH expression in this area is an indicator of dopaminergic activity, which is believed to be involved in normal and critical development of complex cognitive behaviors that are mediated by the mesocortical dopaminergic pathway, such as working memory, attention, behavioral inhibition, and cognitive flexibility.[21]
Research has shown that when a PR antagonist, such as RU486 (also known as mifepristone), is administered to rats during the neonatal period, decreased tyrosine hydroxylase immunoreactive (TH-ir) cells density, a strong co-expresser with PR-immunoreactivity (PR-ir), is seen in the mPFC of juvenile rodents. Later on, in adulthood, decreased levels of TH-ir in the VTA are also shown. This alteration in TH-ir fiber expression, an indicator of altered dopaminergic activity resulting from neonatal PR antagonist administration, has been shown to impair later performance on tasks that measure behavioral inhibition and impulsivity, as well as cognitive flexibility in adulthood. Similar cognitive flexibility impairments were also seen in PR knockout mice as a result of reduced dopaminergic activity in the VTA.[21]
Conversely, when a PR agonist, such as 17α-hydroxyprogesterone caproate, is administered to rodents during perinatal life, as the mesocortical dopaminergic pathway is developing, dopaminergic innervation of the mPFC increases. As a result, TH-ir fiber density also increases. Interestingly, this increase in TH-ir fibers and dopaminergic activity is also linked to impaired cognitive flexibility with increased perseveration later on in life.[22]
In combination, these findings suggest that PR expression during early development impact later cognitive functioning in rodents. Furthermore, it appears as though abnormal levels of PR activity during this critical period of mesocortical dopaminergic pathway development may have profound effects on specific behavioral neural circuits involved in the formation of later complex cognitive behavior.[21][22]
Progesterone receptor has been shown to interact with many other proteins since it is a transcription factor with many cofactors. A small selection of these includes:
↑ "Human PubMed Reference:". National Center for Biotechnology Information, U.S. National Library of Medicine.
↑ "Mouse PubMed Reference:". National Center for Biotechnology Information, U.S. National Library of Medicine.
↑ Misrahi M, Atger M, d'Auriol L, Loosfelt H, Meriel C, Fridlansky F, etal. (March 1987). "Complete amino acid sequence of the human progesterone receptor deduced from cloned cDNA". Biochemical and Biophysical Research Communications. 143 (2): 740–8. doi:10.1016/0006-291X(87)91416-1. PMID3551956.
↑ Rockwell LC, Rowe EJ, Arnson K, Jackson F, Froment A, Ndumbe P, etal. (2012). "Worldwide distribution of allelic variation at the progesterone receptor locus and the incidence of female reproductive cancers". American Journal of Human Biology. 24 (1): 42–51. doi:10.1002/ajhb.21233. PMID22121098. S2CID205302494.
Mansour I, Reznikoff-Etievant MF, Netter A (August 1994). "No evidence for the expression of the progesterone receptor on peripheral blood lymphocytes during pregnancy". Human Reproduction. 9 (8): 1546–9. doi:10.1093/oxfordjournals.humrep.a138746. PMID7989520.
Wang JD, Zhu JB, Fu Y, Shi WL, Qiao GM, Wang YQ, etal. (February 1996). "Progesterone receptor immunoreactivity at the maternofetal interface of first trimester pregnancy: a study of the trophoblast population". Human Reproduction. 11 (2): 413–9. doi:10.1093/humrep/11.2.413. PMID8671234.
Richer JK, Lange CA, Wierman AM, Brooks KM, Tung L, Takimoto GS, etal. (April 1998). "Progesterone receptor variants found in breast cells repress transcription by wild-type receptors". Breast Cancer Research and Treatment. 48 (3): 231–41. doi:10.1023/A:1005941117247. PMID9598870. S2CID27266907.
This page is based on this Wikipedia article Text is available under the CC BY-SA 4.0 license; additional terms may apply. Images, videos and audio are available under their respective licenses.