
The parasympathetic nervous system (PSNS) is one of the three divisions of the autonomic nervous system, the others being the sympathetic nervous system and the enteric nervous system. The enteric nervous system is sometimes considered part of the autonomic nervous system, and sometimes considered an independent system.
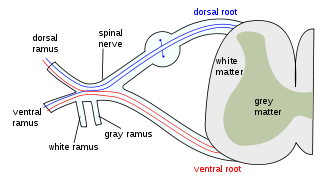
A spinal nerve is a mixed nerve, which carries motor, sensory, and autonomic signals between the spinal cord and the body. In the human body there are 31 pairs of spinal nerves, one on each side of the vertebral column. These are grouped into the corresponding cervical, thoracic, lumbar, sacral and coccygeal regions of the spine. There are eight pairs of cervical nerves, twelve pairs of thoracic nerves, five pairs of lumbar nerves, five pairs of sacral nerves, and one pair of coccygeal nerves. The spinal nerves are part of the peripheral nervous system.

Interventional radiology (IR) is a medical specialty that performs various minimally-invasive procedures using medical imaging guidance, such as x-ray fluoroscopy, computed tomography, magnetic resonance imaging, or ultrasound. IR performs both diagnostic and therapeutic procedures through very small incisions or body orifices. Diagnostic IR procedures are those intended to help make a diagnosis or guide further medical treatment, and include image-guided biopsy of a tumor or injection of an imaging contrast agent into a hollow structure, such as a blood vessel or a duct. By contrast, therapeutic IR procedures provide direct treatment—they include catheter-based medicine delivery, medical device placement, and angioplasty of narrowed structures.

In human anatomy, the abdominal aorta is the largest artery in the abdominal cavity. As part of the aorta, it is a direct continuation of the descending aorta.

The stellate ganglion is a sympathetic ganglion formed by the fusion of the inferior cervical ganglion and the first thoracic ganglion, which exists in 80% of people. Sometimes, the second and the third thoracic ganglia are included in this fusion. The stellate ganglion is relatively big compared to much smaller thoracic, lumbar and sacral ganglia, and is polygonal in shape. Stellate ganglion is located at the level of C7, anterior to the transverse process of C7 and the neck of the first rib, superior to the cervical pleura and just below the subclavian artery. It is superiorly covered by the prevertebral lamina of the cervical fascia and anteriorly in relation with common carotid artery, subclavian artery and the beginning of vertebral artery which sometimes leaves a groove at the apex of this ganglion.

The pterygopalatine ganglion is a parasympathetic ganglion found in the pterygopalatine fossa. It is largely innervated by the greater petrosal nerve ; and its postsinaptic axons project to the lacrimal glands and nasal mucosa. The flow of blood to the nasal mucosa, in particular the venous plexus of the conchae, is regulated by the pterygopalatine ganglion and heats or cools the air in the nose. It is one of four parasympathetic ganglia of the head and neck, the others being the submandibular ganglion, otic ganglion, and ciliary ganglion.

In human anatomy, the inferior mesenteric artery, often abbreviated as IMA, is the third main branch of the abdominal aorta and arises at the level of L3, supplying the large intestine from the distal transverse colon to the upper part of the anal canal. The regions supplied by the IMA are the descending colon, the sigmoid colon, and part of the rectum.

The psoas major is a long fusiform muscle located in the lateral lumbar region between the vertebral column and the brim of the lesser pelvis. It joins the iliacus muscle to form the iliopsoas. In animals, this muscle is equivalent to the tenderloin.

Nerve block or regional nerve blockade is any deliberate interruption of signals traveling along a nerve, often for the purpose of pain relief. Local anesthetic nerve block is a short-term block, usually lasting hours or days, involving the injection of an anesthetic, a corticosteroid, and other agents onto or near a nerve. Neurolytic block, the deliberate temporary degeneration of nerve fibers through the application of chemicals, heat, or freezing, produces a block that may persist for weeks, months, or indefinitely. Neurectomy, the cutting through or removal of a nerve or a section of a nerve, usually produces a permanent block. Because neurectomy of a sensory nerve is often followed, months later, by the emergence of new, more intense pain, sensory nerve neurectomy is rarely performed.

The iliopsoas muscle refers to the joined psoas major and the iliacus muscles. The two muscles are separate in the abdomen, but usually merge in the thigh. They are usually given the common name iliopsoas. The iliopsoas muscle joins to the femur at the lesser trochanter. It acts as the strongest flexor of the hip.

A nerve plexus is a plexus of intersecting nerves. A nerve plexus is composed of afferent and efferent fibers that arise from the merging of the anterior rami of spinal nerves and blood vessels. There are five spinal nerve plexuses, except in the thoracic region, as well as other forms of autonomic plexuses, many of which are a part of the enteric nervous system. The nerves that arise from the plexuses have both sensory and motor functions. These functions include muscle contraction, the maintenance of body coordination and control, and the reaction to sensations such as heat, cold, pain, and pressure. There are several plexuses in the body, including:
Neurolysis is the application of physical or chemical agents to a nerve in order to cause a temporary degeneration of targeted nerve fibers. When the nerve fibers degenerate, it causes an interruption in the transmission of nerve signals. In the medical field, this is most commonly and advantageously used to alleviate pain in cancer patients.

The obturator nerve in human anatomy arises from the ventral divisions of the second, third, and fourth lumbar nerves in the lumbar plexus; the branch from the third is the largest, while that from the second is often very small.

The lumbar arteries are arteries located in the lower back or lumbar region. The lumbar arteries are in parallel with the intercostals.
Each spinal nerve receives a branch called a gray ramus communicans from the adjacent paravertebral ganglion of the sympathetic trunk. The gray rami communicantes contain postganglionic nerve fibers of the sympathetic nervous system and are composed of largely unmyelinated neurons. This is in contrast to the white rami communicantes, in which heavily myelinated neurons give the rami their white appearance.

The sympathetic ganglia, or paravertebral ganglia are autonomic ganglia, of the sympathetic nervous system. Ganglia are 20,000 to 30,000 afferent and efferent nerve cell bodies that run along on either side of the spinal cord. Afferent nerve cell bodies bring information from the body to the brain and spinal cord, while efferent nerve cell bodies bring information from the brain and spinal cord to the rest of the body. The cell bodies create long sympathetic chains that are on either side of the spinal cord. They also form para- or pre-vertebral ganglia of gross anatomy.

The hypogastric nerve is the nerve that transitions between the superior hypogastric plexus and the inferior hypogastric plexus. The hypogastric nerve enters the sympathetic chain at T12-L3.

The lumbar ganglia are paravertebral ganglia located in the inferior portion of the sympathetic trunk. The lumbar portion of the sympathetic trunk typically has 4 lumbar ganglia. The lumbar splanchnic nerves arise from the ganglia here, and contribute sympathetic efferent fibers to the nearby plexuses. The first two lumbar ganglia have both white and gray rami communicates.

The following outline is provided as an overview of and topical guide to human anatomy:
Local anesthetic nerve block is a short-term nerve block involving the injection of local anesthetic as close to the nerve as possible for pain relief. The local anesthetic bathes the nerve and numbs the area of the body that is supplied by that nerve. The goal of the nerve block is to prevent pain by blocking the transmission of pain signals from the affected area. Nerve blocks have a number of uses including treating headache disorders and providing anesthesia during surgery. The pain relief provided by the block is present during the surgery and continues to last after the procedure. This can lead to a reduction in the amount of opiates needed for pain control. The advantages of nerve blocks over general anesthesia include faster recovery, monitored anesthesia care vs. intubation with an airway tube, and much less postoperative pain.
