Related Research Articles

Cholesteatoma is a destructive and expanding growth consisting of keratinizing squamous epithelium in the middle ear and/or mastoid process. Cholesteatomas are not cancerous as the name may suggest, but can cause significant problems because of their erosive and expansile properties. This can result in the destruction of the bones of the middle ear (ossicles), as well as growth through the base of the skull into the brain. They often become infected and can result in chronically draining ears. Treatment almost always consists of surgical removal.

Rhinoplasty, commonly called nose job, medically called nasal reconstruction, is a plastic surgery procedure for altering and reconstructing the nose. There are two types of plastic surgery used – reconstructive surgery that restores the form and functions of the nose and cosmetic surgery that changes the appearance of the nose. Reconstructive surgery seeks to resolve nasal injuries caused by various traumas including blunt, and penetrating trauma and trauma caused by blast injury. Reconstructive surgery can also treat birth defects, breathing problems, and failed primary rhinoplasties. Rhinoplasty may remove a bump, narrow nostril width, change the angle between the nose and the mouth, or address injuries, birth defects, or other problems that affect breathing, such as a deviated nasal septum or a sinus condition. Surgery only on the septum is called a septoplasty.

Rhinitis, also known as coryza, is irritation and inflammation of the mucous membrane inside the nose. Common symptoms are a stuffy nose, runny nose, sneezing, and post-nasal drip.

A nosebleed, also known as epistaxis, is an instance of bleeding from the nose. Blood can flow down into the stomach, and cause nausea and vomiting. In more severe cases, blood may come out of both nostrils. Rarely, bleeding may be so significant that low blood pressure occurs. Blood may also be forced to flow up and through the nasolacrimal duct and out of the eye, producing bloody tears.

Septoplasty, or alternatively submucous septal resection and septal reconstruction, is a corrective surgical procedure done to straighten a deviated nasal septum – the nasal septum being the partition between the two nasal cavities. Ideally, the septum should run down the center of the nose. When it deviates into one of the cavities, it narrows that cavity and impedes airflow. Deviated nasal septum or “crooked” internal nose can occur at childbirth or as the result of an injury or other trauma. If the wall that functions as a separator of both sides of the nose is tilted towards one side at a degree greater than 50%, it might cause difficulty breathing. Often the inferior turbinate on the opposite side enlarges, which is termed compensatory hypertrophy. Deviations of the septum can lead to nasal obstruction. Most surgeries are completed in 60 minutes or less, while the recovery time could be up to several weeks. Put simply, septoplasty is a surgery that helps repair the passageways in the nose making it easier to breathe. This surgery is usually performed on patients with a deviated septum, recurrent rhinitis, or sinus issues.

Laryngectomy is the removal of the larynx. In a total laryngectomy, the entire larynx is removed with the separation of the airway from the mouth, nose and esophagus. In a partial laryngectomy, only a portion of the larynx is removed. Following the procedure, the person breathes through an opening in the neck known as a stoma. This procedure is usually performed by an ENT surgeon in cases of laryngeal cancer. Many cases of laryngeal cancer are treated with more conservative methods. A laryngectomy is performed when these treatments fail to conserve the larynx or when the cancer has progressed such that normal functioning would be prevented. Laryngectomies are also performed on individuals with other types of head and neck cancer. Less invasive partial laryngectomies, including tracheal shaves and feminization laryngoplasty may also be performed on transgender women and other female or non-binary identified individuals to feminize the larynx and/or voice. Post-laryngectomy rehabilitation includes voice restoration, oral feeding and more recently, smell and taste rehabilitation. An individual's quality of life can be affected post-surgery.
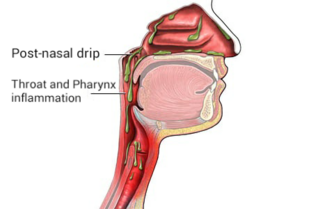
Post-nasal drip (PND), also known as upper airway cough syndrome (UACS), occurs when excessive mucus is produced by the nasal mucosa. The excess mucus accumulates in the back of the nose, and eventually in the throat once it drips down the back of the throat. It can be caused by rhinitis, sinusitis, gastroesophageal reflux disease (GERD), or by a disorder of swallowing. Other causes can be allergy, cold, flu, and side effects from medications.

The dilator naris muscle is a part of the nasalis muscle. It has an anterior and a posterior part. It has origins from the nasal notch of the maxilla and the major alar cartilage, and a single insertion near the margin of the nostril. It controls nostril width, including changes during breathing. Its function can be tested as an analogue for the function of the facial nerve (VII), which supplies it.

Empty nose syndrome (ENS) is a clinical syndrome, the hallmark symptom of which is a sensation of suffocation despite a clear airway. This syndrome is often referred to as a form of secondary atrophic rhinitis. ENS is a potential complication of nasal turbinate surgery or injury. Patients have usually undergone a turbinectomy or other surgical procedures that injure the nasal turbinates.
Phantosmia, also called an olfactory hallucination or a phantom odor, is smelling an odor that is not actually there. This is intrinsically suspicious as the formal evaluation and detection of relatively low levels of odour particles is itself a very tricky task in air epistemology. It can occur in one nostril or both. Unpleasant phantosmia, cacosmia, is more common and is often described as smelling something that is burned, foul, spoiled, or rotten. Experiencing occasional phantom smells is normal and usually goes away on its own in time. When hallucinations of this type do not seem to go away or when they keep coming back, it can be very upsetting and can disrupt an individual's quality of life.
Chronic atrophic rhinitis, or simply atrophic rhinitis, is a chronic inflammation of the nose characterised by atrophy of nasal mucosa, including the glands, turbinate bones and the nerve elements supplying the nose. Chronic atrophic rhinitis may be primary and secondary. Special forms of chronic atrophic rhinitis are rhinitis sicca anterior and ozaena. It can also be described as the empty nose syndrome.
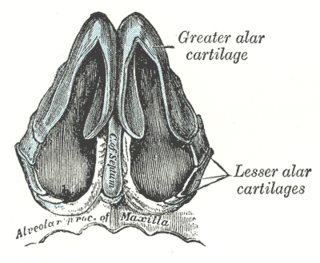
The nasal cartilages are structures within the nose that provide form and support to the nasal cavity. The nasal cartilages are made up of a flexible material called hyaline cartilage in the distal portion of the nose. There are five individual cartilages that make up the nasal cavity: septal nasal cartilage, lateral nasal cartilage, major alar cartilage, minor alar cartilage, and vomeronasal cartilage.

Dacryocystorhinostomy (DCR) is a surgical procedure to restore the flow of tears into the nose from the lacrimal sac when the nasolacrimal duct does not function.
Adenoid hypertrophy, also known as enlarged adenoids refers to an enlargement of the adenoid that is linked to nasopharyngeal mechanical blockage and/or chronic inflammation. Adenoid hypertrophy is a characterized by hearing loss, recurrent otitis media, mucopurulent rhinorrhea, chronic mouth breathing, nasal airway obstruction, increased infection susceptibility, and dental malposition.

The human nose is the first organ of the respiratory system. It is also the principal organ in the olfactory system. The shape of the nose is determined by the nasal bones and the nasal cartilages, including the nasal septum, which separates the nostrils and divides the nasal cavity into two.

Tympanosclerosis is a condition caused by hyalinization and subsequent calcification of subepithelial connective tissue of the tympanic membrane and middle ear, sometimes resulting in a detrimental effect to hearing.
A turbinectomy or turbinoplasty is a surgical procedure, that removes tissue, and sometimes bone, of the turbinates in the nasal passage, particularly the inferior nasal concha. The procedure is usually performed to relieve nasal obstructions. In most cases, turbinate hypertrophy is accompanied by some septum deviation, so the surgery is done along with septoplasty.

Hypernasal speech is a disorder that causes abnormal resonance in a human's voice due to increased airflow through the nose during speech. It is caused by an open nasal cavity resulting from an incomplete closure of the soft palate and/or velopharyngeal sphincter. In normal speech, nasality is referred to as nasalization and is a linguistic category that can apply to vowels or consonants in a specific language. The primary underlying physical variable determining the degree of nasality in normal speech is the opening and closing of a velopharyngeal passageway between the oral vocal tract and the nasal vocal tract. In the normal vocal tract anatomy, this opening is controlled by lowering and raising the velum or soft palate, to open or close, respectively, the velopharyngeal passageway.

An oroantral fistula (OAF) is an epithelialized oroantral communication (OAC), which refers to an abnormal connection between the oral cavity and the antrum. The creation of an OAC is most commonly due to the extraction of a maxillary tooth (typically a maxillary first molar) which is closely related to the antral floor. A small OAC up to 5 millimeters may heal spontaneously, but a larger OAC would require surgical closure to prevent the development of a persistent OAF and chronic sinusitis.
Laryngotracheal reconstruction is a surgical procedure that involves expanding or removing parts of the airway to widen a narrowing within it, called laryngotracheal stenosis or subglottic stenosis.
References
- ↑ Young, A (May 1967). "Closure of the Nostrils in Atrophic Rhinitis". The Journal of Laryngology & Otology. 81 (5): 515–524. doi:10.1017/S0022215100067426. PMID 6024992. S2CID 45818218 . Retrieved 2009-07-06.
- ↑ Gadre, K. C.; K. B. Bhargava; R. Y. Pradhax; J. D. Lodaya; M. V. Ingle (1971). "Closure of the nostrils (Young's operation) in atrophic rhinitis". The Journal of Laryngology and Otology. 85 (7): 711–714. doi:10.1017/s0022215100073977. PMID 5104495. S2CID 38540336 . Retrieved 2009-07-06.
- ↑ Poddar, Sangeet Kumar; M. V. Jagade (2001). "Modification of Modified Young's Operation in the Management of Primary Atrophic Rhinitis". Indian Journal of Otolaryngology and Head and Neck Surgery. 53 (3): 252–254. doi:10.1007/BF03028570. PMC 3450669 . PMID 23119813.