
In humans and other primates, the knee joins the thigh with the leg and consists of two joints: one between the femur and tibia, and one between the femur and patella. It is the largest joint in the human body. The knee is a modified hinge joint, which permits flexion and extension as well as slight internal and external rotation. The knee is vulnerable to injury and to the development of osteoarthritis.

The posterior cruciate ligament (PCL) is a ligament in each knee of humans and various other animals. It works as a counterpart to the anterior cruciate ligament (ACL). It connects the posterior intercondylar area of the tibia to the medial condyle of the femur. This configuration allows the PCL to resist forces pushing the tibia posteriorly relative to the femur.
The anterior cruciate ligament (ACL) is one of a pair of cruciate ligaments in the human knee. The two ligaments are also called "cruciform" ligaments, as they are arranged in a crossed formation. In the quadruped stifle joint, based on its anatomical position, it is also referred to as the cranial cruciate ligament. The term cruciate translates to cross. This name is fitting because the ACL crosses the posterior cruciate ligament to form an "X". It is composed of strong, fibrous material and assists in controlling excessive motion. This is done by limiting mobility of the joint. The anterior cruciate ligament is one of the four main ligaments of the knee, providing 85% of the restraining force to anterior tibial displacement at 30 and 90° of knee flexion. The ACL is the most injured ligament of the four located in the knee.
Allotransplant is the transplantation of cells, tissues, or organs to a recipient from a genetically non-identical donor of the same species. The transplant is called an allograft, allogeneic transplant, or homograft. Most human tissue and organ transplants are allografts.

Osgood–Schlatter disease (OSD) is inflammation of the patellar ligament at the tibial tuberosity (apophysitis) usually affecting adolescents during growth spurts. It is characterized by a painful bump just below the knee that is worse with activity and better with rest. Episodes of pain typically last a few weeks to months. One or both knees may be affected and flares may recur.

The semitendinosus is a long superficial muscle in the back of the thigh. It is so named because it has a very long tendon of insertion. It lies posteromedially in the thigh, superficial to the semimembranosus.

Patellar tendon rupture is a tear of the tendon that connects the knee cap (patella) to the tibia. Often there is sudden onset of pain and walking is difficult. In a complete rupture, the ability to extend that knee is decreased. A pop may be felt when it occurs.
An anterior cruciate ligament injury occurs when the anterior cruciate ligament (ACL) is either stretched, partially torn, or completely torn. The most common injury is a complete tear. Symptoms include pain, an audible cracking sound during injury, instability of the knee, and joint swelling. Swelling generally appears within a couple of hours. In approximately 50% of cases, other structures of the knee such as surrounding ligaments, cartilage, or meniscus are damaged.

The patellar tendon is the distal portion of the common tendon of the quadriceps femoris, which is continued from the patella to the tibial tuberosity. It is also sometimes called the patellar ligament as it forms a bone to bone connection when the patella is fully ossified.
The unhappy triad, also known as a blown knee among other names, is an injury to the anterior cruciate ligament, medial collateral ligament, and meniscus. Analysis during the 1990s indicated that this 'classic' O'Donoghue triad is actually an unusual clinical entity among athletes with knee injuries. Some authors mistakenly believe that in this type of injury, "combined anterior cruciate and medial collateral ligament disruptions that were incurred during athletic endeavors" always present with concomitant medial meniscus injury. However, the 1990 analysis showed that lateral meniscus tears are more common than medial meniscus tears in conjunction with sprains of the ACL.

A tear of a meniscus is a rupturing of one or more of the fibrocartilage strips in the knee called menisci. When doctors and patients refer to "torn cartilage" in the knee, they actually may be referring to an injury to a meniscus at the top of one of the tibiae. Menisci can be torn during innocuous activities such as walking or squatting. They can also be torn by traumatic force encountered in sports or other forms of physical exertion. The traumatic action is most often a twisting movement at the knee while the leg is bent. In older adults, the meniscus can be damaged following prolonged 'wear and tear'. Especially acute injuries can lead to displaced tears which can cause mechanical symptoms such as clicking, catching, or locking during motion of the joint. The joint will be in pain when in use, but when there is no load, the pain goes away.

A patellar dislocation is a knee injury in which the patella (kneecap) slips out of its normal position. Often the knee is partly bent, painful and swollen. The patella is also often felt and seen out of place. Complications may include a patella fracture or arthritis.
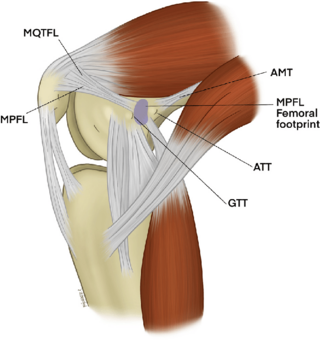
The medial patellofemoral ligament (MPFL) is one of several ligaments on the medial aspect of the knee. It originates in the superomedial aspect of the patella and inserts in the space between the adductor tubercle and the medial femoral epicondyle. The ligament itself extends from the femur to the superomedial patella, and its shape is similar to a trapezoid. It keeps the patella in place, but its main function is to prevent lateral displacement of the patella.

Knee pain is pain in or around the knee.
Eccentric training is a type of strength training that involves using the target muscles to control weight as it moves in a downward motion. This type of training can help build muscle, improve athletic performance, and reduce the risk of injury. An eccentric contraction is the motion of an active muscle while it is lengthening under load. Eccentric training is repetitively doing eccentric muscle contractions. For example, in a biceps curl the action of lowering the dumbbell back down from the lift is the eccentric phase of that exercise – as long as the dumbbell is lowered slowly rather than letting it drop.
Posterolateral corner injuries of the knee are injuries to a complex area formed by the interaction of multiple structures. Injuries to the posterolateral corner can be debilitating to the person and require recognition and treatment to avoid long term consequences. Injuries to the PLC often occur in combination with other ligamentous injuries to the knee; most commonly the anterior cruciate ligament (ACL) and posterior cruciate ligament (PCL). As with any injury, an understanding of the anatomy and functional interactions of the posterolateral corner is important to diagnosing and treating the injury.
Medial knee injuries are the most common type of knee injury. The medial ligament complex of the knee consists of:

The function of the posterior cruciate ligament (PCL) is to prevent the femur from sliding off the anterior edge of the tibia and to prevent the tibia from displacing posterior to the femur. Common causes of PCL injuries are direct blows to the flexed knee, such as the knee hitting the dashboard in a car accident or falling hard on the knee, both instances displacing the tibia posterior to the femur.

Labral reconstruction is a type of hip arthroscopy in which the patient's native labrum is partially or completely removed and reconstructed using either autograft or allograft tissue. Originally described in 2009 using the ligamentum teres capitis, arthroscopic labral reconstruction using a variety of graft tissue has demonstrated promising short and mid-term clinical outcomes. Most importantly, labral reconstruction has demonstrated utility when the patient's native labral tissue is far too damaged for debridement or repair.
Artificial ligaments are devices used to replace damaged ligaments. Today, the most common use of artificial ligaments is in anterior cruciate ligament reconstruction. Although autotransplantation remains the most common method of ligament reconstruction, numerous materials and structures were developed to optimize the artificial ligament since its creation in the World War I era. Many modern artificial ligaments are made of synthetic polymers, such as polyethylene terephthalate. Various coatings have been added to improve the biocompatibility of the synthetic polymers. Early artificial ligaments developed in the 1980s were ineffective due to material deterioration. Currently, the Ligament Advanced Reinforcement System (LARS) artificial ligament has been utilized extensively in clinical applications. Tissue engineering is a growing area of research which aims to regenerate and restore ligament function.



