Brucella spp. are the cause of brucellosis, which is a zoonosis transmitted by ingesting contaminated food (such as unpasteurized milk products), direct contact with an infected animal, or inhalation of aerosols. Transmission from human to human, for example, through sexual intercourse, or from mother to child, is exceedingly rare, but possible.[5] Minimum infectious exposure is between 10 and 100 organisms.
The different species of Brucella are genetically very similar, although each has a slightly different host specificity. Hence, the National Center for Biotechnology Information taxonomy includes most Brucella species under B. melitensis.
The many names of brucellosis include (human disease/animal disease):
Sir David Bruce isolated B. melitensis from British soldiers who died from Malta fever in Malta. After exposure to Brucella, humans generally have a two- to four-week latency period before exhibiting symptoms, which include acute undulating fever (>90% of all cases), headache, arthralgia (>50%), night sweats, fatigue, and anorexia.[7] Later complications may include arthritis or epididymo-orchitis, spondylitis, neurobrucellosis, liver abscess formation, and endocarditis, the latter potentially fatal.[8]
Human brucellosis is usually not transmitted from human to human; people become infected by contact with fluids from infected animals (sheep, cattle, or pigs) or derived food products, such as unpasteurized milk and cheese. Brucellosis is also considered an occupational disease because of a higher incidence in people working with animals (slaughterhouse cases). People may also be infected by inhalation of contaminated dust or aerosols, and as such, the CDC has labeled Brucella species as highly weaponizable. Human and animal brucellosis share the persistence of the bacteria in tissues of the mononuclear phagocyte system, including the spleen, liver, lymph nodes, and bone marrow. Brucella can also target the male reproductive tract.[7]
Globally, an estimated 500,000 cases of brucellosis occur each year.[7]
Malta fever was a major health problem to British troops in Malta in the 19th and early 20th centuries, resulting in over 6000 cases and 574 deaths.[9] In 1860, J.A. Maraston, assistant surgeon in the British Army in Malta, gave the first accurate description of the disease he called "Mediterranian gastric remittent fever". In 1897, A.E. Wright, a pathologist in British army, developed the agglutination test, diagnostic of the disease.
In 1905, Zammit, a Maltese physician, identified goats as the source of infection. E. Bang, a Danish veterinarian, described the intracellular pathogen causing abortion in cattle in 1897, and named it Bacillus abortus. In 1918, A. Evans, an American microbiologist, made the connection between B. abortus and Micrococcus melitensis, and placed them in the Bacteriaceae.
In 1914, Mohler isolated an organism from the liver and spleen of pigs, B. suis; B. neotome, B. ovis, and B. canis were described in 1957, 1963, and 1966, respectively.[9]
Transmission
Zoonosis affecting domestic animals is caused by contact with milk, urine, and genital organs, which concentrate the causative organisms. Some reservoirs include buffalo and other animals, but mostly cattle.[10] In humans, the disease is acquired from unpasteurised milk and products or undercooked meat (consumers), laboratory inhalation (lab workers), accidental skin penetration or abrasion (farmers, slaughterhouse workers, and veterinarians), and (rarely) conjunctival contact, blood transfusion, transplacental, and person-to-person.[11][12]
Human disease
Brucellosis can affect any organ or organ system, and 90% of patients have a cyclical (undulant) fever. Though variable, symptoms can also include these clinical signs: headache, weakness, arthralgia, depression, weight loss, fatigue, and liver dysfunction. Foul-smelling perspiration is considered a classical sign. Between 20 and 60% of cases have osteoarticular complications: arthritis, spondylitis, or osteomyelitis. Hepatomegaly may occur, as can gastrointestinal complications.
Up to 20% of cases can have genitourinary involvement; orchitis and epididymitis are most common. Neurological symptoms include depression and mental fatigue. Cardiovascular involvement can include endocarditis resulting in death.
Chronic brucellosis is hard to define; length, type, and response to treatment are variable. Localized infection can occur. Blood donations of infected persons should not be accepted.[13]
The general agreement is that brucellosis in pregnant women is not linked to congenital malformations. The newborn can be either uninfected, which is more common, or infected with congenital or neonatal brucellosis. The majority of uninfected neonates delivered at term have a favorable outcome, whereas preterm births and cases with congenital brucellosis have an increased risk of neonatal death. Congenital brucellosis can be transmitted transplacentally, whereas neonatal brucellosis can be acquired through contact with body fluids secreted during birth or through postpartum breastfeeding. Congenital brucellosis, on the other hand, is a rare condition; most cases are associated with premature birth, and it affects about 2% of infants exposed to brucellosis in utero.[14] Congenitally infected infants can exhibit low birth weight, failure to thrive, jaundice, hepatomegaly, splenomegaly, respiratory difficulty, and general signs of sepsis (fever, vomiting). Some cases are asymptomatic.[13]
Characteristics
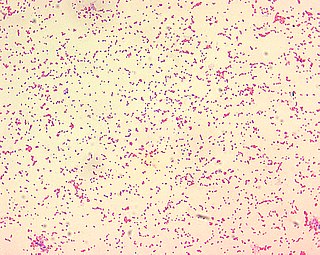
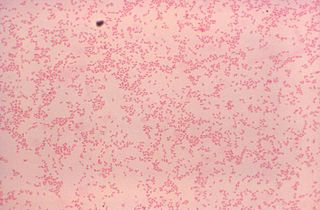
Brucella species are small, Gram-negative, facultative coccobacilli, most lacking a capsule, endospores, or native plasmids. They are intracellular within the host organism, and show environmental persistence outside the host. The intracellular trafficking includes two or three main steps, starting with endosomal vacuoles, then endoplasmic reticulum-derived compartments and finally vacuoles having several markers of atypical autophagy.[15] They survive extremes in temperature, pH, and humidity, and in frozen and aborted materials. They infect many species, but with some specificity.[16]
The Brucella species belongs to the Rhizobiales group, in the Alphaproteobacteria class. They are growing by unipolar growth, like Agrobacterium tumefaciens, Sinorhizobium meliloti, and Ochrobactrum anthropi.[17] They usually have two chromosomes[15] and their replication and segregation are temporally organized.[18]
Clinical manifestations
The gastrointestinal tract is affected in about 70% of cases, including anorexia, abdominal pain, vomiting, diarrhea, constipation, hepatomegaly, and splenomegaly. The liver is involved in most cases, but function tests are normal or mildly abnormal. Granulomas (B. abortus), hepatitis (B. melitensis), and abscesses (B. suis) are seen.
The skeletal system is affected in 20–60% of cases, including arthritis (hip, knee, and ankle), spondylitis, osteomyelitis, and sacroiliitis (most common). Lumbar vertebrae can be affected showing the classical radiological sign of vertebral erosion. Neurological symptoms include meningitis, encephalitis, radiculopathy, peripheral neuropathy, intracerebral abscesses, and acute or chronic neck rigidity (<50%), and the cerebrospinal fluid can show lymphocytic pleocytosis, low sugar, increased protein, positive bacterial culture (<50%), and agglutination (positive in >95%).
Cardiovascular involvement is low (endocarditis at 2%), but is the major cause of mortality. Often, valve replacement and antibiotics are needed. Pericarditis and myocarditis are seen, too.
Pulmonary infection can be from inhalation or hematogenous sources, and can cause any chest syndrome. Rarely is Brucella isolated from sputum. Genitourinary infection can include epidydemoorchitis or pyonephrosis (rare). Cutaneous involvement is not specific. Hematological signs include anemia, leukopenia, and thrombocytopenia.[19]
Diagnosis
Brucella is isolated from a blood culture on Castaneda medium or from bone marrow. Prolonged incubation (up to six weeks) may be required, as they are slow-growing, but on modern automated machines, the cultures often show positive results within 7 days. On Gram stain, they appear as dense clumps of Gram-negative coccobacilli and are exceedingly difficult to see. In recent years, molecular diagnostic techniques based on the genetic component of the pathogen have become more popular.[3]
Differentiating Brucella from Salmonella is crucial, as the latter could also be isolated from blood cultures and is Gram-negative. Testing for urease would successfully accomplish the task; it is positive for Brucella and negative for Salmonella. Brucella can also be seen in bone marrow biopsies.
Laboratory-acquired brucellosis is common.[20] This most often happens when the disease is not thought of until cultures become positive, by which time the specimens have already been handled by a number of laboratory staff. The idea of preventive treatment is to stop people who have been exposed to Brucella from becoming ill with the disease. Polymerase chain reaction (PCR) shows promise for rapid diagnosis of Brucella species in human blood specimens. Positive PCR at the completion of treatment is not predictive of subsequent relapse. PCR testing for fluid and tissue samples other than blood has also been described. A history of animal contact is pivotal; in endemic area, it should be in the diagnosis of any nonspecific febrile illness.
In the laboratory, biochemical tests can be diagnostic.[19] Oxidase and catalase tests are positive for most members of the genus Brucella.
Test
B. melitensis
B. abortus
B. suis
B. neotomae
B. ovis
B. canis
Need to CO2
-
+
-
-
+
-
production of H2S
-
+
+
+
-
-
Growth on basic fushin 0.002%
+
+
-
-
+
-
Growth on thionin 0.004%
-
-
+
-
+
+
Growth on thionin 0.002%
+
-
+
+
+
+
Destroy with Tb phage
-
+
-
-
-
-
Serum agglutination with a titer > 1:160 in the presence of a compatible illness supports the diagnosis of brucellosis. Demonstration of a four-fold or greater increase or decrease in agglutinating antibodies over four to 12 weeks provides even stronger evidence for the diagnosis.
ELISA is probably the second-most common serologic method.[21] The sensitivity of the ELISA was 100% when compared with blood culture, but only 44% compared with serologic tests other than ELISA. The specificity was >99%. In a study including 75 patients with brucellosis, five patients with positive ELISA had a negative tube agglutination test. In several Brucella-endemic regions, the Febrile Antigen Brucella Agglutination Test (FBAT) is primarily used for diagnostics. Recent investigations on the use of FBAT have however illustrated its high inaccuracy in proper diagnosis, highlighting the difficulty of brucellosis control in low-income settings.[22]
In the setting of Brucella arthritis, the synovial-fluid white blood cell count does not generally exceed 15,000 cells/μl.[21] In brucellosis, lymphocytes frequently predominate (in contrast to septic arthritis due to other bacteria, in which polymorphonuclear leukocytes frequently predominate.
The prognosis[23] for brucellosis before the use of antibiotics had a mortality of 2%, mainly due to endocarditis, and morbidity was high, especially with B. melitensis. Permanent nerve deafness and spinal cord damage often occurred.
Control of disease in domestic animals by immunization using B. abortus strain 19 and B. melitensis strain Rev 1: Vaccination in young cattle helps in protection, but does not offer full effectiveness.
Routine pasteurization of milk
In labs, strict biosafety precautions
As regions endemic with Brucella primarily are low-income environments, approaching proper control of brucellosis remains a challenge. A recent case-based investigation in north-eastern Kenya illustrated how community engagement with veterinarians and medical professionals might contribute in preventive strategies, but that additional political engagement is called for to ensure proper diagnostic and treatment standards.[22]
Treatment
No clinical trials exist to be relied on as a guide for optimal treatment, but an at least six-week course of rifampicin or gentamicin and doxycycline twice daily is the combination most often used, and appears to be efficacious;[20][24][25][26] the advantage of this regimen is that it is oral medication with no injections; however, a high rate of side effects (nausea, vomiting, loss of appetite) has also been reported.[26] The relatedness in treatment and endemic overlap of tuberculosis remains an issue however, as treatment of one might cause resistance in the second. Local dispensaries dealing first-hand with brucellosis are occasionally also not aware on how to treat properly, highlighting the need for reevaluation on implementation of international treatment regimes.[22]
As of August 2013, Allison Rice-Ficht, Ph.D. at Texas A&M University and her team claim to be close to creating a human vaccine. It would primarily be used to immunize members of the military in case of exposure to weaponized Brucella on the battlefield.[27]
Host specificity and animal brucellosis
Brucella species have been found primarily in mammals:[7]
Pathogenic Brucella species can cause abortion in female animals by colonization of placental trophoblasts, and sterility in male animals.[28] Drugs with effects against Brucella include tetracyclines, aminoglycosides (streptomycin, [since 1947], gentamicin, netilmicin), rifampicin, quinolones (ciprofloxacin), and third-generation cephalosporins. Treatment for uncomplicated brucellosis includes:
Streptomycin + doxycycline for 6 weeks
TMP/SMX + doxycycline for 6 weeks
Rifampicin + doxycycline for 6 weeks
Treatment of complicated brucellosis (endocarditis, meningitis) has no uniform agreement, but usually uses three anti-Brucella drugs for three months.
The plague of Thebes
Brucellosis caused by B. abortus best fits the characteristics of the plague described in Oedipus Rex. Although the disease progression of brucellosis in modern times may make it seem unlikely, it was at least one agent in what may have been a multicomponent plague, along with Salmonella enterica serovar Typhi or another pathogen, or possibly the ancestral versions of Brucella were more lethal.[29]
Genomics
The Brucella genome includes two chromosomes; the first chromosome codes mostly for genes related to metabolism, while the second (smaller one) includes several genes related to pathogenicity. The genomes of most Brucella species have been sequenced,[30] and typically encode 3,200 to 3,500 open reading frames (ORFs). Examples include:
Genome data for these and other Brucella strains are available in the GOLD[30] and PATRIC[31] databases. Also, a public and editable spreadsheet of B. abortus 2308W genome annotation has been created, to be updated based on new discoveries. Also, the genome annotation is available in a user friendly table at the web page http://hdl.handle.net/11056/23125.
Infection of macrophages by B. abortus is stimulated by blue light in the wild type, but is limited in photochemically inactive and null mutants, indicating a flavin-containing histidine kinase functions as a photoreceptor regulating B. abortus virulence. Conversely, depriving Brucella of the blue wavelengths dropped its reproductive rate by 90%.[33][34]
Notes
↑ Brucella abortus, Brucella canis, Brucella neotomae, Brucella ovis, and Brucella suis are all synonyms of Brucella melitensis.
Related Research Articles
Q fever or query fever is a disease caused by infection with Coxiella burnetii, a bacterium that affects humans and other animals. This organism is uncommon, but may be found in cattle, sheep, goats, and other domestic mammals, including cats and dogs. The infection results from inhalation of a spore-like small-cell variant, and from contact with the milk, urine, feces, vaginal mucus, or semen of infected animals. Rarely, the disease is tick-borne. The incubation period can range from 9 to 40 days. Humans are vulnerable to Q fever, and infection can result from even a few organisms. The bacterium is an obligate intracellular pathogenic parasite.
Babesiosis or piroplasmosis is a malaria-like parasitic disease caused by infection with a eukaryotic parasite in the order Piroplasmida, typically a Babesia or Theileria, in the phylum Apicomplexa. Human babesiosis transmission via tick bite is most common in the Northeastern and Midwestern United States and parts of Europe, and sporadic throughout the rest of the world. It occurs in warm weather. People can get infected with Babesia parasites by the bite of an infected tick, by getting a blood transfusion from an infected donor of blood products, or by congenital transmission . Ticks transmit the human strain of babesiosis, so it often presents with other tick-borne illnesses such as Lyme disease. After trypanosomes, Babesia is thought to be the second-most common blood parasite of mammals. They can have major adverse effects on the health of domestic animals in areas without severe winters. In cattle, the disease is known as Texas cattle fever or redwater.
Brucellosis is a zoonosis caused by ingestion of unpasteurized milk from infected animals, or close contact with their secretions. It is also known as undulant fever, Malta fever, and Mediterranean fever.
Infective endocarditis is an infection of the inner surface of the heart, usually the valves. Signs and symptoms may include fever, small areas of bleeding into the skin, heart murmur, feeling tired, and low red blood cell count. Complications may include backward blood flow in the heart, heart failure – the heart struggling to pump a sufficient amount of blood to meet the body's needs, abnormal electrical conduction in the heart, stroke, and kidney failure.
Leptospirosis is a blood infection caused by the bacteria Leptospira that can infect humans, dogs, rodents and many other wild and domesticated animals. Signs and symptoms can range from none to mild to severe. Weil's disease, the acute, severe form of leptospirosis, causes the infected individual to become jaundiced, develop kidney failure, and bleed. Bleeding from the lungs associated with leptospirosis is known as severe pulmonary haemorrhage syndrome.
Rat-bite fever (RBF) is an acute, febrile human illness caused by bacteria transmitted by rodents, in most cases, which is passed from rodent to human by the rodent's urine or mucous secretions. Alternative names for rat-bite fever include streptobacillary fever, streptobacillosis, spirillary fever, bogger, and epidemic arthritic erythema. It is a rare disease spread by infected rodents and caused by two specific types of bacteria:
Streptobacillus moniliformis, the only reported bacteria that causes RBF in North America
Spirillum minus, common in Asia. Most cases occur in Japan, but specific strains of the disease are present in the United States, Europe, Australia, and Africa.
Brucella melitensis is a Gram-negative coccobacillus bacterium from the Brucellaceae family. The bacterium causes ovine brucellosis, along with Brucella ovis. It affects primarily sheep and goats, but cases have also been observed in cattle, yaks, water buffalo, Bactrian and dromedary camels, alpacas, dogs, horses and pigs. Humans can become infected if they have contact with an infected animal or its byproducts. Animals acquire B. melitensis by venereal transmission and contact with the placenta, fetus, fetal fluids, and vaginal discharges from infected animals. The organism is found in blood, urine, milk, and semen. It is zoonotic, unlike B. ovis, causing Malta fever or localized brucellosis in humans.
Brucella suis is a bacterium that causes swine brucellosis, a zoonosis that affects pigs. The disease typically causes chronic inflammatory lesions in the reproductive organs of susceptible animals or orchitis, and may even affect joints and other organs. The most common symptom is abortion in pregnant susceptible sows at any stage of gestation. Other manifestations are temporary or permanent sterility, lameness, posterior paralysis, spondylitis, and abscess formation. It is transmitted mainly by ingestion of infected tissues or fluids, semen during breeding, and suckling infected animals.
Bartonellosis is an infectious disease produced by bacteria of the genus Bartonella. Bartonella species cause diseases such as Carrión's disease, trench fever, cat-scratch disease, bacillary angiomatosis, peliosis hepatis, chronic bacteremia, endocarditis, chronic lymphadenopathy, and neurological disorders.
Campylobacter fetus is a rod-shaped, gram-negative species of bacteria within the genus Campylobacter of phylum Pseudomonadota. Identification of C. fetus species in infected animals or people is routinely performed by culture on blood or cefoperazone deoxycholate agar. Subspecies of C. fetus commonly causes reproductive disease in ruminants and gastrointestinal disease in humans. Transmission of C. fetus subspecies venerealis occurs mainly through venereal contact while transmission of C. fetus subspecies fetus occurs mainly through ingestion of bacteria in a contaminated environment. Infertility in cattle and abortion in sheep are common outcomes of infection associated with C. fetus subspecies venerealis and C. fetus subspecies fetus, respectively. Disease in humans occurs through zoonotic transmission of C. fetus mainly via ingestion of contaminated food or water sources. C. fetus can be diagnosed with polymerase chain reaction assays, enzyme linked immunosorbent assays and vaginal mucus agglutination testing. As vaccines are typically not efficient in preventing future spread, infected bulls are often culled. Human infections may be treated with erythromycin as antimicrobial resistance has been emerging for the fluoroquinolones.
Babesia, also called Nuttallia, is an apicomplexan parasite that infects red blood cells and is transmitted by ticks. Originally discovered by the Romanian bacteriologist Victor Babeș in 1888, over 100 species of Babesia have since been identified.
Brucella abortus is a Gram-negative bacterium in the family Brucellaceae and is one of the causative agents of brucellosis. The rod-shaped pathogen is classified under the domain Bacteria. The prokaryotic B. abortus is non-spore-forming, non-motile and aerobic.
Bartonella rochalimae is a recently discovered strain of Gram-negative bacteria in the genus Bartonella, isolated by researchers at the University of California, San Francisco (UCSF), Massachusetts General Hospital, and the United States Centers for Disease Control and Prevention. The bacterium is a close relative of Bartonella quintana, the microbe which caused trench fever in thousands of soldiers during World War I. Named after Brazilian scientist Henrique da Rocha Lima, B. rochalimae is also closely related to Bartonella henselae, a bacterium identified in the mid-1990s during the AIDS epidemic in San Francisco as the cause of cat scratch fever, which still infects more than 24,000 people in the United States each year.
Bartonella quintana, originally known as Rochalimaea quintana, and "Rickettsia quintana", is a bacterium transmitted by the human body louse that causes trench fever. This bacterial species caused outbreaks of trench fever affecting 1 million soldiers in Europe during World War I.
Alice Catherine Evans was an American microbiologist. She became a researcher at the U.S. Department of Agriculture where she investigated bacteriology in milk and cheese. She proved that Bacillus abortus caused the disease brucellosis in both cattle and humans which led to the pasteurization of milk in US in 1930. Evans was the first woman president elected by the Society of American Bacteriologists.
Brucella canis is a Gram-negative bacterium in the family Brucellaceae that causes brucellosis in dogs and other canids. It is a non-motile short-rod or coccus-shaped organism, and is oxidase, catalase, and urease positive. B. canis causes infertility in both male and female dogs. It can also cause inflammation in the eyes. The hosts of B. canis ranges from domestic animals to foxes and coyotes. It is passed from species to species via genital fluids. Treatments such as spaying, neutering, and long-term antibiotics have been used to combat B. canis. The species was first described in the United States in 1966 where mass abortions of beagles were documented. Brucella canis can be found in both pets and wild animals and lasts the lifespan of the animal it has affected. B. canis has two distinct circular chromosomes that can attribute to horizontal gene transfer.
Brucella ceti is a gram negative bacterial pathogen of the Brucellaceae family that causes brucellosis in cetaceans. Brucella ceti has been found in both classes of cetaceans, mysticetes and odontocetes. Brucellosis in some dolphins and porpoises can result in serious clinical signs including fetal abortions, male infertility, neurobrucellosis, cardiopathies, bone and skin lesions, stranding events, and death.
Brucella intermedia is a bacterium from the genus of Brucella. It was first described by Velasco and others in 1998. It causes diseases in humans only rarely, with single case reports of cholangitis following liver transplantation, bacteremia in a patient with bladder cancer, a pelvic abscess after abdominal surgery, dyspepsia, endophthalmitis in the presence of a foreign body, pneumonia, and endocarditis.
Remittent fever is a type or pattern of fever in which temperature does not touch the baseline and remains above normal throughout the day. Daily variation in temperature is more than 1°C in 24 hours, which is also the main difference as compared to continuous fever. Fever due to most infectious diseases is remittent. Diagnosis is based upon clinical history, blood tests, blood culture and chest X-ray.
Joseph Michael Vinetz is a Professor of Medicine and Anthropology at Yale University, Research Professor at the Universidad Peruana Cayetano Heredia and Associate Investigator of the Alexander von Humboldt Institute of Tropical Medicine at the Universidad Peruana Cayetano Heredia.
1 2 3 4 Atluri VL, Xavier MN, de Jong MF, den Hartigh AB, Tsolis RM (2011). "Interactions of the human pathogenic Brucella species with their hosts". Annual Review of Microbiology. 65: 523–541. doi:10.1146/annurev-micro-090110-102905. PMID21939378.
This page is based on this Wikipedia article Text is available under the CC BY-SA 4.0 license; additional terms may apply. Images, videos and audio are available under their respective licenses.