
Infectious mononucleosis, also known as glandular fever, is an infection usually caused by the Epstein–Barr virus (EBV). Most people are infected by the virus as children, when the disease produces few or no symptoms. In young adults, the disease often results in fever, sore throat, enlarged lymph nodes in the neck, and fatigue. Most people recover in two to four weeks; however, feeling tired may last for months. The liver or spleen may also become swollen, and in less than one percent of cases splenic rupture may occur.
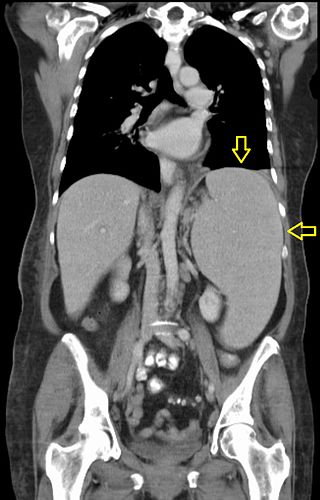
Splenomegaly is an enlargement of the spleen. The spleen usually lies in the left upper quadrant (LUQ) of the human abdomen. Splenomegaly is one of the four cardinal signs of hypersplenism which include: some reduction in number of circulating blood cells affecting granulocytes, erythrocytes or platelets in any combination; a compensatory proliferative response in the bone marrow; and the potential for correction of these abnormalities by splenectomy. Splenomegaly is usually associated with increased workload, which suggests that it is a response to hyperfunction. It is therefore not surprising that splenomegaly is associated with any disease process that involves abnormal red blood cells being destroyed in the spleen. Other common causes include congestion due to portal hypertension and infiltration by leukemias and lymphomas. Thus, the finding of an enlarged spleen, along with caput medusae, is an important sign of portal hypertension.

Palpation is the process of using one's hands to check the body, especially while perceiving/diagnosing a disease or illness. Usually performed by a health care practitioner, it is the process of feeling an object in or on the body to determine its size, shape, firmness, or location.
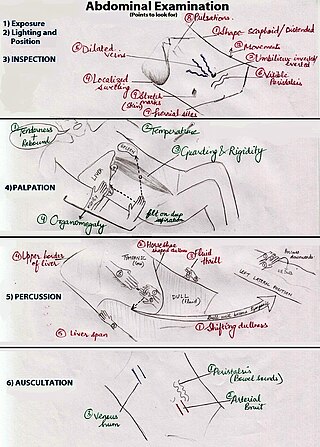
An abdominal examination is a portion of the physical examination which a physician or nurse uses to clinically observe the abdomen of a patient for signs of disease. The abdominal examination is conventionally split into four different stages: first, inspection of the patient and the visible characteristics of their abdomen. Auscultation (listening) of the abdomen with a stethoscope. Palpation of the patient's abdomen. Finally, percussion (tapping) of the patient's abdomen and abdominal organs. Depending on the need to test for specific diseases such as ascites, special tests may be performed as a part of the physical examination. An abdominal examination may be performed because the physician suspects a disease of the organs inside the abdominal cavity (including the liver, spleen, large or small intestines), or simply as a part of a complete physical examination for other conditions. In a complete physical examination, the abdominal exam classically follows the respiratory examination and cardiovascular examination.
In medicine, Murphy's sign is a maneuver during a physical examination as part of the abdominal examination. It is useful for differentiating pain in the right upper quadrant. Typically, it is positive in cholecystitis, but negative in choledocholithiasis, pyelonephritis, and ascending cholangitis.
In medicine, the cardiac examination, also precordial exam, is performed as part of a physical examination, or when a patient presents with chest pain suggestive of a cardiovascular pathology. It would typically be modified depending on the indication and integrated with other examinations especially the respiratory examination.

A respiratory examination, or lung examination, is performed as part of a physical examination, in response to respiratory symptoms such as shortness of breath, cough, or chest pain, and is often carried out with a cardiac examination.
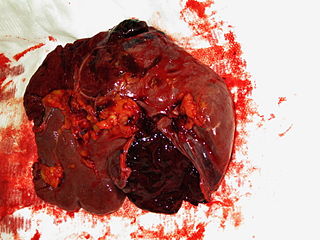
A splenic injury, which includes a ruptured spleen, is any injury to the spleen. The rupture of a normal spleen can be caused by trauma, such as a traffic collision.
In medicine, shifting dullness refers to a sign elicited on physical examination for ascites.
An abdominal mass is any localized enlargement or swelling in the human abdomen. Depending on its location, the abdominal mass may be caused by an enlarged liver (hepatomegaly), enlarged spleen (splenomegaly), protruding kidney, a pancreatic mass, a retroperitoneal mass, an abdominal aortic aneurysm, or various tumours, such as those caused by abdominal carcinomatosis and omental metastasis. The treatments depend on the cause, and may range from watchful waiting to radical surgery.

Traube's (semilunar) space is an anatomic space of some clinical importance. It is a crescent-shaped space, encompassed by the lower edge of the left lung, the anterior border of the spleen, the left costal margin and the inferior margin of the left lobe of the liver. Thus, its surface markings are respectively the left sixth rib superiorly, the left mid axillary line laterally, and the left costal margin inferiorly.
Felty's syndrome (FS), also called Felty syndrome, is a rare autoimmune disease characterized by the triad of rheumatoid arthritis, enlargement of the spleen and low neutrophil count. The condition is more common in those aged 50–70 years, specifically more prevalent in females than males, and more so in Caucasians than those of African descent. It is a deforming disease that causes many complications for the individual.
An acute abdomen refers to a sudden, severe abdominal pain. It is in many cases a medical emergency, requiring urgent and specific diagnosis. Several causes need immediate surgical treatment.

Focused assessment with sonography in trauma is a rapid bedside ultrasound examination performed by surgeons, emergency physicians, and paramedics as a screening test for blood around the heart or abdominal organs (hemoperitoneum) after trauma. There is also the extended FAST (eFAST) which includes some additional ultrasound views to assess for pneumothorax.

Abdominal ultrasonography is a form of medical ultrasonography to visualise abdominal anatomical structures. It uses transmission and reflection of ultrasound waves to visualise internal organs through the abdominal wall. For this reason, the procedure is also called a transabdominal ultrasound, in contrast to endoscopic ultrasound, the latter combining ultrasound with endoscopy through visualize internal structures from within hollow organs.

A pelvic examination is the physical examination of the external and internal female pelvic organs. It is frequently used in gynecology for the evaluation of symptoms affecting the female reproductive and urinary tract, such as pain, bleeding, discharge, urinary incontinence, or trauma. It can also be used to assess a woman's anatomy in preparation for procedures. The exam can be done awake in the clinic and emergency department, or under anesthesia in the operating room. The most commonly performed components of the exam are 1) the external exam, to evaluate the external genitalia 2) the internal exam with palpation to examine the uterus, ovaries, and structures adjacent to the uterus (adnexae) and 3) the internal exam using a speculum to visualize the vaginal walls and cervix. During the pelvic exam, sample of cells and fluids may be collected to screen for sexually transmitted infections or cancer.
Pre-test probability and post-test probability are the probabilities of the presence of a condition before and after a diagnostic test, respectively. Post-test probability, in turn, can be positive or negative, depending on whether the test falls out as a positive test or a negative test, respectively. In some cases, it is used for the probability of developing the condition of interest in the future.
The cardiovascular examination is a portion of the physical examination that involves evaluation of the cardiovascular system. The exact contents of the examination will vary depending on the presenting complaint but a complete examination will involve the heart, lungs, belly and the blood vessels.
In medical diagnosis Nixon's sign is an alternative to Castell's sign, useful in identifying splenomegaly.
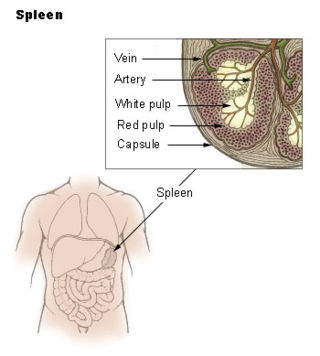
Spleen pain is a pain felt from the left upper quadrant of the abdomen or epigastrium where the human spleen is located or neighboring.
