In terms of available healthcare and health status Sierra Leone is rated very poorly. Globally, infant and maternal mortality rates remain among the highest. The major causes of illness within the country are preventable with modern technology and medical advances. Most deaths within the country are attributed to nutritional deficiencies, lack of access to clean water, pneumonia, diarrheal diseases, anemia, malaria, tuberculosis and HIV/AIDS.
Health in the Comoros continues to face public health problems characteristic of developing countries. After Comoros's independence in 1975, the French withdrew their medical teams, leaving the three islands' already rudimentary health care system in a state of severe crisis. French assistance was eventually resumed, and other nations also contributed medical assistance to the young republic.

Deficient sanitation systems, poor nutrition, and inadequate health services have pushed Haiti to the bottom of the World Bank’s rankings of health indicators. According to the United Nations World Food Programme, 80 percent of Haiti’s population lives below the poverty line. In fact, 75% of the Haitian population lives off of $2.50 per day. Consequently, malnutrition is a significant problem. Half the population can be categorized as "food insecure," and half of all Haitian children are undersized as a result of malnutrition. Less than half the population has access to clean drinking water, a rate that compares poorly even with other less-developed nations. Haiti's healthy life expectancy at birth is 63 years. The World Health Organization (WHO) estimates that only 43 percent of the target population receives the recommended immunizations.
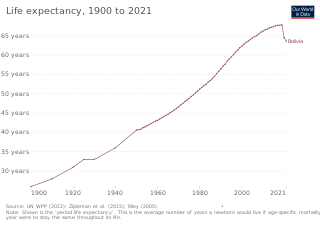
In terms of key indicators, health in Bolivia ranks nearly last among the Western Hemisphere countries. Only Haiti scores consistently lower. Bolivia's child mortality rate of 69 per 1,000 live births is the worst in South America. Proper nourishment is a constant struggle for many Bolivians. Experts estimate that 7 percent of Bolivian children under the age of five and 23 percent of the entire population suffer from malnutrition. Another health factor in Bolivia is sanitation.
Health in Indonesia is affected by a number of factors. Indonesia has over 26,000 health care facilities; 2,000 hospitals, 9,000 community health centres and private clinics, 1,100 dentist clinics and 1,000 opticians. The country lacks doctors with only 0.4 doctors per 1,000 population. In 2018, Indonesia's healthcare spending was US$38.3 billion, 4.18% of their GDP, and is expected to rise to US$51 billion in 2020.
Health in Iraq refers to the country's public healthcare system and the overall health of the country's population. Iraq belongs to WHO health region Eastern Mediterranean and classified as upper middle according to World Bank income classification 2013. The state of health in Iraq has fluctuated during its turbulent recent history and specially during the last 4 decade. The country had one of the highest medical standards in the region during the period of 1980s and up until 1991, the annual total health budget was about $450 million in average. The 1991 Gulf War incurred Iraq's major infrastructures a huge damage. This includes health care system, sanitation, transport, water and electricity supplies. UN economic sanctions aggravated the process of deterioration. The annual total health budget for the country, a decade after the sanctions had fallen to $22 million which is barely 5% of what it was in 1980s. During its last decade, the regime of Saddam Hussein cut public health funding by 90 percent, contributing to a substantial deterioration in health care. During that period, maternal mortality increased nearly threefold, and the salaries of medical personnel decreased drastically. Medical facilities, which in 1980 were among the best in the Middle East, deteriorated. Conditions were especially serious in the south, where malnutrition and water-borne diseases became common in the 1990s. Health indicators deteriorated during the 1990s. In the late 1990s, Iraq's infant mortality rates more than doubled. Because treatment and diagnosis of cancer and diabetes decreased in the 1990s, complications and deaths resulting from those diseases increased drastically in the late 1990s and early 2000s.

In terms of major health indicators, health in Paraguay ranks near the median among South American countries. In 2003 Paraguay had a child mortality rate of 29.5 deaths per 1,000 children, ranking it behind Argentina, Colombia, and Uruguay but ahead of Brazil and Bolivia. The health of Paraguayans living outside urban areas is generally worse than those residing in cities. Many preventable diseases, such as Chagas' disease, run rampant in rural regions. Parasitic and respiratory diseases, which could be controlled with proper medical treatment, drag down Paraguay's overall health. In general, malnutrition, lack of proper health care, and poor sanitation are the root of many health problems in Paraguay.

Niger is a landlocked country located in West Africa and has Libya, Chad, Nigeria, Benin, Mali, Burkina Faso, and Algeria as its neighboring countries. Niger was French territory that got its independence in 1960 and its official language is French. Niger has an area of 1.267 million square kilometres, nevertheless, 80% of its land area spreads through the Sahara Desert.

In precolonial Ghana, infectious diseases were the main cause of morbidity and mortality. The modern history of health in Ghana was heavily influenced by international actors such as Christian missionaries, European colonists, the World Bank, and the International Monetary Fund. In addition, the democratic shift in Ghana spurred healthcare reforms in an attempt to address the presence of infectious and noncommunicable diseases eventually resulting in the formation of the National Health insurance Scheme in place today.

Health problems have been a long-standing issue limiting development in the Democratic Republic of the Congo.

Health in Angola is rated among the worst in the world.

Health in the Central African Republic has been degraded by years of internal conflict and economic turmoil since independence from France in 1960. One sixth of the country's population is in need of acute medical care. Endemic diseases put a high demand on the health infrastructure, which requires outside assistance to sustain itself.

Ivory Coast faces multiple health challenges, caused by factors including malaria, lack of access to medicine, and healthcare staffing shortages.
The Human Rights Measurement Initiative finds that Equatorial Guinea is fulfilling 43.5% of what it should be fulfilling for the right to health based on its level of income. When looking at the right to health with respect to children, Equatorial Guinea achieves 64.4% of what is expected based on its current income. In regards to the right to health amongst the adult population, the country achieves only 58.8% of what is expected based on the nation's level of income. Equatorial Guinea falls into the "very bad" category when evaluating the right to reproductive health because the nation is fulfilling only 7.3% of what the nation is expected to achieve based on the resources (income) it has available.
The WHO's estimate of life expectancy for a female child born in Guinea-Bissau in 2008 was 49 years, and 47 years for a boy. in 2016 life expectancy had improved to 58 for men and 61 for women.

Health in Mozambique has a complex history, influenced by the social, economic, and political changes that the country has experienced. Before the Mozambican Civil War, healthcare was heavily influenced by the Portuguese. After the civil war, the conflict affected the country's health status and ability to provide services to its people, breeding the host of health challenges the country faces in present day.

Expenditure on health in Senegal was 4.7% of GDP in 2014, US$107 per capita.

Health in Peru has changed drastically from pre-colonial times to the modern era. When European conquistadors invaded Peru, they brought with them diseases against which the Inca population had no acquired immunity. Much of the population died, and this marked an important turning point in the nature of Peruvian healthcare. Since Peru gained independence, the country's major healthcare concern has shifted to the disparity in care between the poor and non-poor, as well as between rural and urban populations. Another unique factor is the presence of indigenous health beliefs, which continue to be widespread in modern society.

Life expectancy in Albania was estimated at 77.59 years, in 2014, ranking 51st in the world, and outperforming a number of European Union countries, such as Hungary, Poland and the Czech Republic. In 2016 it was 74 for men and 79 for women. The most common causes of death are circulatory diseases followed by cancerous illnesses. Demographic and Health Surveys completed a survey in April 2009, detailing various health statistics in Albania, including male circumcision, abortion and more.
The Health in Eswatini is poor and four years into the United Nations sustainable development goals, Eswatini seems unlikely to achieve goal on health. As a result of 63% poverty prevalence, 27% HIV prevalence, and poor health systems, maternal mortality rate is a high 389/100,000 live births, and under 5 mortality rate is 70.4/1000 live births resulting in a life expectancy that remains amongst the lowest in the world. Despite significant international aid, the government fails to adequately fund the health sector. Nurses are now and again engaged in demonstrations over poor working conditions, drug stock outs, all of which impairs quality health delivery. Despite tuberculosis and AIDS being major causes of death, diabetes and other non-communicable diseases are on the rise. Primary health care is relatively free in Eswatini save for its poor quality to meet the needs of the people. Road traffic accidents have increased over the years and they form a significant share of deaths in the country.


