
Demographic features of the population of Cambodia include population density, ethnicity, education level, health of the populace, economic status, religious affiliations and other aspects of the population.

The demographics of North Korea are determined through national censuses and international estimates. The Central Bureau of Statistics of North Korea conducted the most recent census in 2008, where the population reached 24 million inhabitants. The population density is 199.54 inhabitants per square kilometre, and the 2014 estimated life expectancy is 69.81 years. In 1980, the population rose at a near consistent, but low, rate. Since 2000, North Korea's birth rate has exceeded its death rate; the natural growth is positive. In terms of age structure, the population is dominated by the 15–64-year-old segment (68.09%). The median age of the population is 32.9 years, and the gender ratio is 0.95 males to 1.00 female. Since the early 1990s, the birth rate has been fairly stable, with an average of 2 children per woman, down from an average of 3 in the early 1980s.

The current population of Nepal is 29,164,578 as per the 2021 census. The population growth rate is 0.92% per year.

China is the second most populous country in Asia as well as the second most populous country in the world, with a population of 1,425,671,352.

Sex-selective abortion is the practice of terminating a pregnancy based upon the predicted sex of the infant. The selective abortion of female fetuses is most common where male children are valued over female children, especially in parts of East Asia and South Asia, as well as in the Caucasus, Western Balkans, and to a lesser extent North America. Based on the third National Family and Health Survey, results showed that if both partners, mother and father, or just the father, preferred male children, sex-selective abortion was more common. In cases where only the mother prefers sons, this is likely to result in sex-selective neglect in which the child is not likely to survive past infancy.
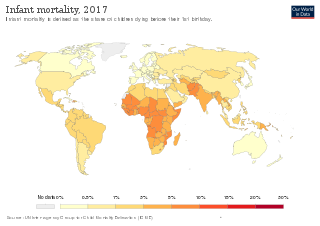
Infant mortality is the death of an infant before the infant's first birthday. The occurrence of infant mortality in a population can be described by the infant mortality rate (IMR), which is the number of deaths of infants under one year of age per 1,000 live births. Similarly, the child mortality rate, also known as the under-five mortality rate, compares the death rate of children up to the age of five.

Family planning is the consideration of the number of children a person wishes to have, including the choice to have no children, and the age at which they wish to have them. Things that may play a role on family planning decisions include marital situation, career or work considerations, financial situations. If sexually active, family planning may involve the use of contraception and other techniques to control the timing of reproduction.
The maternal mortality ratio is a key performance indicator (KPI) for efforts to improve the health and safety of mothers before, during, and after childbirth per country worldwide. Often referred to as MMR, it is the annual number of female deaths per 100,000 live births from any cause related to or aggravated by pregnancy or its management. It is not to be confused with the maternal mortality rate, which is the number of maternal deaths in a given period per 100,000 women of reproductive age during the same time period. The statistics are gathered by WHO, UNICEF, UNFPA, World Bank Group, and the United Nations Population Division. The yearly report started in 1990 and is called Trends in Maternal Mortality. As of the 2015 data published in 2016, the countries that have seen an increase in the maternal mortality ratio since 1990 are the Bahamas, Georgia, Guyana, Jamaica, Dem. People’s Rep. Korea, Serbia, South Africa, St. Lucia, Suriname, Tonga, United States, Venezuela, RB Zimbabwe. But according to Sustainable Development Goals report 2018, the overall maternal mortality ratio has declined by 37 percent since 2002. Nearly 303,000 women died due to complications during pregnancy.
Women's health differs from that of men in many unique ways. Women's health is an example of population health, where health is defined by the World Health Organization as "a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity". Often treated as simply women's reproductive health, many groups argue for a broader definition pertaining to the overall health of women, better expressed as "The health of women". These differences are further exacerbated in developing countries where women, whose health includes both their risks and experiences, are further disadvantaged.
Health equity arises from access to the social determinants of health, specifically from wealth, power and prestige. Individuals who have consistently been deprived of these three determinants are significantly disadvantaged from health inequities, and face worse health outcomes than those who are able to access certain resources. It is not equity to simply provide every individual with the same resources; that would be equality. In order to achieve health equity, resources must be allocated based on an individual need-based principle.
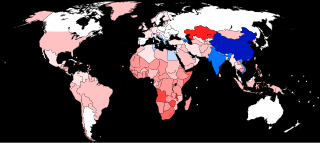
The human sex ratio is the ratio of males to females in a population in the context of anthropology and demography. In humans, the natural sex ratio at birth is slightly biased towards the male sex. It is estimated to be about 1.05 or 1.06 or within a narrow range from 1.03 to 1.06 males per female.

The term "missing women" indicates a shortfall in the number of women relative to the expected number of women in a region or country. It is most often measured through male-to-female sex ratios, and is theorized to be caused by sex-selective abortions, female infanticide, and inadequate healthcare and nutrition for female children. It is argued that technologies that enable prenatal sex selection, which have been commercially available since the 1970s, are a large impetus for missing female children.
Botswana's healthcare system has been steadily improving and expanding its infrastructure to become more accessible. The country's position as an upper middle-income country has allowed them to make strides in universal healthcare access for much of Botswana's population. The majority of the Botswana's 2.3 million inhabitants now live within five kilometers of a healthcare facility. As a result, the infant mortality and maternal mortality rates have been on a steady decline. The country's improving healthcare infrastructure has also been reflected in an increase of the average life expectancy from birth, with nearly all births occurring in healthcare facilities.
Research shows many health disparities among different racial and ethnic groups in the United States. Different outcomes in mental and physical health exist between all U.S. Census-recognized racial groups, but these differences stem from different historical and current factors, including genetics, socioeconomic factors, and racism. Research has demonstrated that numerous health care professionals show implicit bias in the way that they treat patients. Certain diseases have a higher prevalence among specific racial groups, and life expectancy also varies across groups.

The Gender Inequality Index (GII) is an index for the measurement of gender disparity that was introduced in the 2010 Human Development Report 20th anniversary edition by the United Nations Development Programme (UNDP). According to the UNDP, this index is a composite measure to quantify the loss of achievement within a country due to gender inequality. It uses three dimensions to measure opportunity cost: reproductive health, empowerment, and labor market participation. The new index was introduced as an experimental measure to remedy the shortcomings of the previous indicators, the Gender Development Index (GDI) and the Gender Empowerment Measure (GEM), both of which were introduced in the 1995 Human Development Report.
Female foeticide in India is the abortion of a female foetus outside of legal methods. A research by Pew Research Center based on Union government data indicates foeticide of at least 9 million females in the years 2000-2019. The research found that 86.7% of these foeticides were by Hindus, followed by Sikhs with 4.9%, and Muslims with 6.6%. The research also indicated an overall decline in preference for sons in the time period.
The World Health Organization (WHO) has defined health as "a state of complete physical, mental, and social well-being and not merely the absence of disease or infirmity." Identified by the 2012 World Development Report as one of two key human capital endowments, health can influence an individual's ability to reach his or her full potential in society. Yet while gender equality has made the most progress in areas such as education and labor force participation, health inequality between men and women continues to harm many societies to this day.
China has a history of female infanticide which spans 2,000 years. When Christian missionaries arrived in China in the late sixteenth century, they witnessed newborns being thrown into rivers or onto rubbish piles. In the seventeenth century Matteo Ricci documented that the practice occurred in several of China's provinces and said that the primary reason for the practice was poverty. The practice continued into the 19th century and declined precipitously during the Communist era, but has reemerged as an issue since the introduction of the one-child policy in the early 1980s. The 2020 census showed a male-to-female ratio of 105.07 to 100 for mainland China, a record low since the People's Republic of China began conducting censuses. Every year in China and India alone, there are close to two million instances of some form of female infanticide.
Traditional gender roles in Egypt are prevalent and clearly defined. These roles are largely associated with traditional Islamic family structures, wherein women's roles are closely tied to the domestic sphere and men's roles tied to the public sphere. Gender roles are based on assumed biological differences between the sexes and can lead to dramatically different life experiences as well as opportunities and outcomes for individuals. Consequently, when looking at a number of indicators, women often find themselves disadvantaged relative to men.