Related Research Articles

A goitre, or goiter, is a swelling in the neck resulting from an enlarged thyroid gland. A goitre can be associated with a thyroid that is not functioning properly.

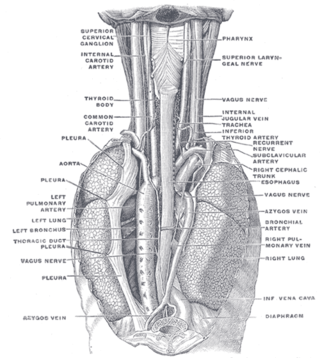
The thoracic cavity is the chamber of the body of vertebrates that is protected by the thoracic wall. The central compartment of the thoracic cavity is the mediastinum. There are two openings of the thoracic cavity, a superior thoracic aperture known as the thoracic inlet and a lower inferior thoracic aperture known as the thoracic outlet.

The superior vena cava (SVC) is the superior of the two venae cavae, the great venous trunks that return deoxygenated blood from the systemic circulation to the right atrium of the heart. It is a large-diameter (24 mm) short length vein that receives venous return from the upper half of the body, above the diaphragm. Venous return from the lower half, below the diaphragm, flows through the inferior vena cava. The SVC is located in the anterior right superior mediastinum. It is the typical site of central venous access via a central venous catheter or a peripherally inserted central catheter. Mentions of "the cava" without further specification usually refer to the SVC.
The azygos vein is a vein running up the right side of the thoracic vertebral column draining itself towards the superior vena cava. It connects the systems of superior vena cava and inferior vena cava and can provide an alternative path for blood to the right atrium when either of the venae cavae is blocked.
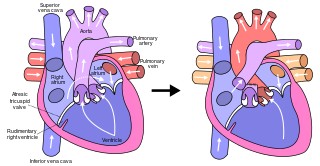
The Fontan procedure or Fontan–Kreutzer procedure is a palliative surgical procedure used in children with univentricular hearts. It involves diverting the venous blood from the inferior vena cava (IVC) and superior vena cava (SVC) to the pulmonary arteries. The procedure varies for differing congenital heart pathologies. For example in tricuspid atresia, the procedure can be done where the blood does not pass through the morphologic right ventricle; i.e., the systemic and pulmonary circulations are placed in series with the functional single ventricle. Whereas in hypoplastic left heart syndrome, the heart is more reliant on the more functional right ventricle to provide blood flow to the systemic circulation. The procedure was initially performed in 1968 by Francis Fontan and Eugene Baudet from Bordeaux, France, published in 1971, simultaneously described in July 1971 by Guillermo Kreutzer from Buenos Aires, Argentina, presented at the Argentinean National Cardilogy meeting of that year and finally published in 1973.

Lymphadenopathy or adenopathy is a disease of the lymph nodes, in which they are abnormal in size or consistency. Lymphadenopathy of an inflammatory type is lymphadenitis, producing swollen or enlarged lymph nodes. In clinical practice, the distinction between lymphadenopathy and lymphadenitis is rarely made and the words are usually treated as synonymous. Inflammation of the lymphatic vessels is known as lymphangitis. Infectious lymphadenitis affecting lymph nodes in the neck is often called scrofula.

A Pancoast tumor is a tumor of the apex of the lung. It is a type of lung cancer defined primarily by its location situated at the top end of either the right or left lung. It typically spreads to nearby tissues such as the ribs and vertebrae. Most Pancoast tumors are non-small-cell lung cancers.

Superior vena cava syndrome (SVCS), is a group of symptoms caused by obstruction of the superior vena cava ("SVC"), a short, wide vessel carrying circulating blood into the heart. The majority of cases are caused by malignant tumors within the mediastinum, most commonly lung cancer and non-Hodgkin's lymphoma, directly compressing or invading the SVC wall. Non-malignant causes are increasing in prevalence due to expanding use of intravascular devices, which can result in thrombosis. Other non-malignant causes include benign mediastinal tumors, aortic aneurysm, infections, and fibrosing mediastinitis.

The mediastinum is the central compartment of the thoracic cavity. Surrounded by loose connective tissue, it is an undelineated region that contains a group of structures within the thorax, namely the heart and its vessels, the esophagus, the trachea, the phrenic and cardiac nerves, the thoracic duct, the thymus and the lymph nodes of the central chest.

A chylothorax is an abnormal accumulation of chyle, a type of lipid-rich lymph, in the space surrounding the lung. The lymphatics of the digestive system normally returns lipids absorbed from the small bowel via the thoracic duct, which ascends behind the esophagus to drain into the left brachiocephalic vein. If normal thoracic duct drainage is disrupted, either due to obstruction or rupture, chyle can leak and accumulate within the negative-pressured pleural space. In people on a normal diet, this fluid collection can sometimes be identified by its turbid, milky white appearance, since chyle contains emulsified triglycerides.

Esophageal rupture is a rupture of the esophageal wall. Iatrogenic causes account for approximately 56% of esophageal perforations, usually due to medical instrumentation such as an endoscopy or paraesophageal surgery. The 10% of esophageal perforations caused specifically by vomiting are termed Boerhaave syndrome.
Mediastinitis is inflammation of the tissues in the mid-chest, or mediastinum. It can be either acute or chronic. It is thought to be due to four different etiologies:

The hemiazygos vein is a vein running superiorly in the lower thoracic region, just to the left side of the vertebral column.

A mediastinal tumor is a tumor in the mediastinum, the cavity that separates the lungs from the rest of the chest. It contains the heart, esophagus, trachea, thymus, and aorta. The most common mediastinal masses are neurogenic tumors, usually found in the posterior mediastinum, followed by thymoma (15–20%) located in the anterior mediastinum. Lung cancer typically spreads to the lymph nodes in the mediastinum.
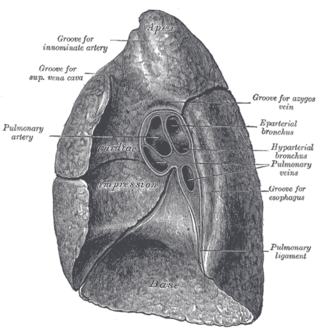
The root of the lung is a group of structures that emerge at the hilum of each lung, just above the middle of the mediastinal surface and behind the cardiac impression of the lung. It is nearer to the back than the front. The root of the lung is connected by the structures that form it to the heart and the trachea. The rib cage is separated from the lung by a two-layered membranous coating, the pleura. The hilum is the large triangular depression where the connection between the parietal pleura and the visceral pleura is made, and this marks the meeting point between the mediastinum and the pleural cavities.

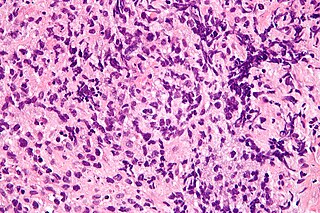
In hematology, hemophagocytic lymphohistiocytosis (HLH), also known as haemophagocytic lymphohistiocytosis, and hemophagocytic or haemophagocytic syndrome, is an uncommon hematologic disorder seen more often in children than in adults. It is a life-threatening disease of severe hyperinflammation caused by uncontrolled proliferation of benign lymphocytes and macrophages that secrete high amounts of inflammatory cytokines. It is classified as one of the cytokine storm syndromes. There are inherited and non-inherited (acquired) causes of HLH.

The bidirectional Glenn (BDG) shunt, or bidirectional cavopulmonary anastomosis, is a surgical technique used in pediatric cardiac surgery procedure used to temporarily improve blood oxygenation for patients with a congenital cardiac defect resulting in a single functional ventricle. Creation of a bidirectional shunt reduces the amount of blood volume that the heart needs to pump at the time of surgical repair with the Fontan procedure.
Mediastinal lymphadenopathy or mediastinal adenopathy is an enlargement of the mediastinal lymph nodes.
Primary mediastinal (thymic) large B-cell lymphoma is a distinct type of diffuse large B-cell lymphoma involving the mediastinum, recognized in the WHO 2008 classification.
In CT scan of the thyroid, focal and diffuse thyroid abnormalities are commonly encountered. These findings can often lead to a diagnostic dilemma, as the CT reflects nonspecific appearances. Ultrasound (US) examination has a superior spatial resolution and is considered the modality of choice for thyroid evaluation. Nevertheless, CT detects incidental thyroid nodules (ITNs) and plays an important role in the evaluation of thyroid cancer.
References
- ↑ Wallace, C; Siminoski K (1996). "The Pemberton sign". Ann Intern Med. 125 (7): 568–569. doi:10.7326/0003-4819-125-7-199610010-00006. PMID 8815756. S2CID 32532890.
- ↑ Pemberton, HS (1946). "Sign of submerged goitre". Lancet. 248 (6423): 509. doi:10.1016/s0140-6736(46)91790-4.
- ↑ Pemberton, HS (1946). "Sign of submerged goitre". Lancet. 248 (6423): 509. doi:10.1016/s0140-6736(46)91790-4.
- ↑ Basaria, S; Salvatori R (2004). "Pemberton's sign". New England Journal of Medicine. 350 (13): 1338. doi:10.1056/nejmicm990287. PMID 15044645.
- ↑ Chow, J; McKim DA; Shennib, H; et al. (1997). "Superior vena cava obstruction secondary to mediastinal lymphadenopathy in a patient with cystic fibrosis". Chest. 112 (5): 1438–1441. doi:10.1378/chest.112.5.1438. PMID 9367491.
- ↑ Tekinbas, C; Erol MM; Ozsu S; et al. (2008). "Giant mass due to Castleman's disease causing superior vena cava syndrome". Thorac Cardiovasc Surg. 56 (5): 303–305. doi:10.1055/s-2008-1038408. PMID 18615381. S2CID 21183690.
- ↑ Park, M; Choi JW; Park HJ; et al. (2012). "Hemophagocytic lymphohistiocytosis can mimic the superior vena cava syndrome". J Pediatr Hematol Oncol. 34 (4): 152–154. doi:10.1097/MPH.0b013e3182422a20. PMID 22395213. S2CID 22479614.