
Broca's area, or the Broca area, is a region in the frontal lobe of the dominant hemisphere, usually the left, of the brain with functions linked to speech production.

Transcranial magnetic stimulation (TMS) is a noninvasive form of brain stimulation in which a changing magnetic field is used to cause electric current at a specific area of the brain through electromagnetic induction. An electric pulse generator, or stimulator, is connected to a magnetic coil, which in turn is connected to the scalp. The stimulator generates a changing electric current within the coil which induces a magnetic field; this field then causes a second inductance of inverted electric charge within the brain itself.
An evoked potential or evoked response is an electrical potential in a specific pattern recorded from a specific part of the nervous system, especially the brain, of a human or other animals following presentation of a stimulus such as a light flash or a pure tone. Different types of potentials result from stimuli of different modalities and types. Evoked potential is distinct from spontaneous potentials as detected by electroencephalography (EEG), electromyography (EMG), or other electrophysiologic recording method. Such potentials are useful for electrodiagnosis and monitoring that include detections of disease and drug-related sensory dysfunction and intraoperative monitoring of sensory pathway integrity.

Deep brain stimulation (DBS) is a neurosurgical procedure involving the placement of a medical device called a neurostimulator, which sends electrical impulses, through implanted electrodes, to specific targets in the brain for the treatment of movement disorders, including Parkinson's disease, essential tremor, dystonia, and other conditions such as obsessive-compulsive disorder (OCD) and epilepsy. While its underlying principles and mechanisms are not fully understood, DBS directly changes brain activity in a controlled manner.

The claustrum is a thin, bilateral collection of neurons and supporting glial cells, that connects to cortical and subcortical regions of the brain. It is located between the insula laterally and the putamen medially, separated by the extreme and external capsules respectively. The blood supply to the claustrum is fulfilled via the middle cerebral artery. It is considered to be the most densely connected structure in the brain, allowing for integration of various cortical inputs into one experience rather than singular events. The claustrum is difficult to study given the limited number of individuals with claustral lesions and the poor resolution of neuroimaging.
Neurotechnology encompasses any method or electronic device which interfaces with the nervous system to monitor or modulate neural activity.

The inferior frontal gyrus(IFG), (gyrus frontalis inferior), is the lowest positioned gyrus of the frontal gyri, of the frontal lobe, and is part of the prefrontal cortex.

The longitudinal fissure is the deep groove that separates the two cerebral hemispheres of the vertebrate brain. Lying within it is a continuation of the dura mater called the falx cerebri. The inner surfaces of the two hemispheres are convoluted by gyri and sulci just as is the outer surface of the brain.
Intraoperative neurophysiological monitoring (IONM) or intraoperative neuromonitoring is the use of electrophysiological methods such as electroencephalography (EEG), electromyography (EMG), and evoked potentials to monitor the functional integrity of certain neural structures during surgery. The purpose of IONM is to reduce the risk to the patient of iatrogenic damage to the nervous system, and/or to provide functional guidance to the surgeon and anesthesiologist.
Frontal lobe epilepsy (FLE) is a neurological disorder which is a subtype of the larger group of epilepsy and then focal epilepsy is characterized by brief, recurring seizures that arise in the frontal lobes of the brain, often while the patient is sleeping. It is the second most common type of focal epilepsy after temporal lobe epilepsy (TLE), and is related to the temporal form by the fact that both forms are characterized by the occurrence of partial (focal) seizures. Partial seizures occurring in the frontal lobes can occur in one of two different forms: either “focal aware”, the old term was simple partial seizures “focal unaware” the old term was complex partial seizures. The symptoms and clinical manifestations of frontal lobe epilepsy can differ depending on which specific area of the frontal lobe is affected.
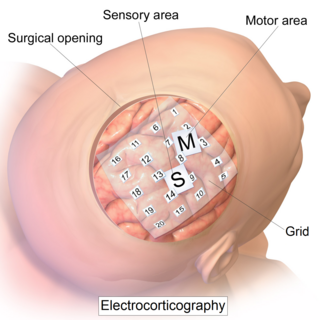
Electrocorticography (ECoG), or intracranial electroencephalography (iEEG), is a type of electrophysiological monitoring that uses electrodes placed directly on the exposed surface of the brain to record electrical activity from the cerebral cortex. In contrast, conventional electroencephalography (EEG) electrodes monitor this activity from outside the skull. ECoG may be performed either in the operating room during surgery or outside of surgery. Because a craniotomy is required to implant the electrode grid, ECoG is an invasive procedure.

Transcranial direct current stimulation (tDCS) is a form of neuromodulation that uses constant, low direct current delivered via electrodes on the head. It was originally developed to help patients with brain injuries or neuropsychiatric conditions such as major depressive disorder. It can be contrasted with cranial electrotherapy stimulation, which generally uses alternating current the same way, as well as transcranial magnetic stimulation.
Central facial palsy is a symptom or finding characterized by paralysis or paresis of the lower half of one side of the face. It usually results from damage to upper motor neurons of the facial nerve.

Electrical brain stimulation (EBS), also referred to as focal brain stimulation (FBS), is a form of electrotherapy used as a technique in research and clinical neurobiology to stimulate a neuron or neural network in the brain through the direct or indirect excitation of its cell membrane by using an electric current. It is used for research or for therapeutic purposes.
Neurostimulation is the purposeful modulation of the nervous system's activity using invasive or non-invasive means. Neurostimulation usually refers to the electromagnetic approaches to neuromodulation.
The temporal dynamics of music and language describes how the brain coordinates its different regions to process musical and vocal sounds. Both music and language feature rhythmic and melodic structure. Both employ a finite set of basic elements that are combined in ordered ways to create complete musical or lingual ideas.
Neuromodulation is "the alteration of nerve activity through targeted delivery of a stimulus, such as electrical stimulation or chemical agents, to specific neurological sites in the body". It is carried out to normalize – or modulate – nervous tissue function. Neuromodulation is an evolving therapy that can involve a range of electromagnetic stimuli such as a magnetic field (rTMS), an electric current, or a drug instilled directly in the subdural space. Emerging applications involve targeted introduction of genes or gene regulators and light (optogenetics), and by 2014, these had been at minimum demonstrated in mammalian models, or first-in-human data had been acquired. The most clinical experience has been with electrical stimulation.
Awake craniotomy is a neurosurgical technique and type of craniotomy that allows a surgeon to remove a brain tumor while the patient is awake to avoid brain damage. During the surgery, the neurosurgeon performs cortical mapping to identify vital areas, called the "eloquent brain", that should not be disturbed while removing the tumor.
Gait variability seen in Parkinson's Disorders arise due to cortical changes induced by pathophysiology of the disease process. Gait rehabilitation is focused to harness the adapted connections involved actively to control these variations during the disease progression. Gait variabilities seen are attributed to the defective inputs from the Basal Ganglia. However, there is altered activation of other cortical areas that support the deficient control to bring about a movement and maintain some functional mobility.

Auditosensory cortex is the part of the auditory system that is associated with the sense of hearing in humans. It occupies the bilateral primary auditory cortex in the temporal lobe of the mammalian brain. The term is used to describe Brodmann area 42 together with the transverse temporal gyri of Heschl. The auditosensory cortex takes part in the reception and processing of auditory nerve impulses, which passes sound information from the thalamus to the brain. Abnormalities in this region are responsible for many disorders in auditory abilities, such as congenital deafness, true cortical deafness, primary progressive aphasia and auditory hallucination.
