Related Research Articles

Agnosia is a neurological disorder characterized by an inability to process sensory information. Often there is a loss of ability to recognize objects, persons, sounds, shapes, or smells while the specific sense is not defective nor is there any significant memory loss. It is usually associated with brain injury or neurological illness, particularly after damage to the occipitotemporal border, which is part of the ventral stream. Agnosia only affects a single modality, such as vision or hearing. More recently, a top-down interruption is considered to cause the disturbance of handling perceptual information.
Agraphia is an acquired neurological disorder causing a loss in the ability to communicate through writing, either due to some form of motor dysfunction or an inability to spell. The loss of writing ability may present with other language or neurological disorders; disorders appearing commonly with agraphia are alexia, aphasia, dysarthria, agnosia, acalculia and apraxia. The study of individuals with agraphia may provide more information about the pathways involved in writing, both language related and motoric. Agraphia cannot be directly treated, but individuals can learn techniques to help regain and rehabilitate some of their previous writing abilities. These techniques differ depending on the type of agraphia.
Anomic aphasia is a mild, fluent type of aphasia where individuals have word retrieval failures and cannot express the words they want to say. By contrast, anomia is a deficit of expressive language, and a symptom of all forms of aphasia, but patients whose primary deficit is word retrieval are diagnosed with anomic aphasia. Individuals with aphasia who display anomia can often describe an object in detail and maybe even use hand gestures to demonstrate how the object is used, but cannot find the appropriate word to name the object. Patients with anomic aphasia have relatively preserved speech fluency, repetition, comprehension, and grammatical speech.

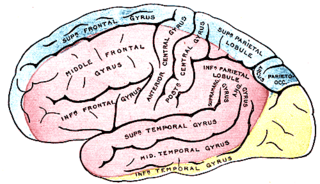
The parietal lobe is one of the four major lobes of the cerebral cortex in the brain of mammals. The parietal lobe is positioned above the temporal lobe and behind the frontal lobe and central sulcus.
The occipital lobe is one of the four major lobes of the cerebral cortex in the brain of mammals. The name derives from its position at the back of the head, from the Latin ob, 'behind', and caput, 'head'.

Visual memory describes the relationship between perceptual processing and the encoding, storage and retrieval of the resulting neural representations. Visual memory occurs over a broad time range spanning from eye movements to years in order to visually navigate to a previously visited location. Visual memory is a form of memory which preserves some characteristics of our senses pertaining to visual experience. We are able to place in memory visual information which resembles objects, places, animals or people in a mental image. The experience of visual memory is also referred to as the mind's eye through which we can retrieve from our memory a mental image of original objects, places, animals or people. Visual memory is one of several cognitive systems, which are all interconnected parts that combine to form the human memory. Types of palinopsia, the persistence or recurrence of a visual image after the stimulus has been removed, is a dysfunction of visual memory.

The angular gyrus is a region of the brain lying mainly in the posteroinferior region of the parietal lobe, occupying the posterior part of the inferior parietal lobule. It represents the Brodmann area 39.
Cortical blindness is the total or partial loss of vision in a normal-appearing eye caused by damage to the brain's occipital cortex. Cortical blindness can be acquired or congenital, and may also be transient in certain instances. Acquired cortical blindness is most often caused by loss of blood flow to the occipital cortex from either unilateral or bilateral posterior cerebral artery blockage and by cardiac surgery. In most cases, the complete loss of vision is not permanent and the patient may recover some of their vision. Congenital cortical blindness is most often caused by perinatal ischemic stroke, encephalitis, and meningitis. Rarely, a patient with acquired cortical blindness may have little or no insight that they have lost vision, a phenomenon known as Anton–Babinski syndrome.
The posterior cerebral artery (PCA) is one of a pair of cerebral arteries that supply oxygenated blood to the occipital lobe, part of the back of the human brain. The two arteries originate from the distal end of the basilar artery, where it bifurcates into the left and right posterior cerebral arteries. These anastomose with the middle cerebral arteries and internal carotid arteries via the posterior communicating arteries.

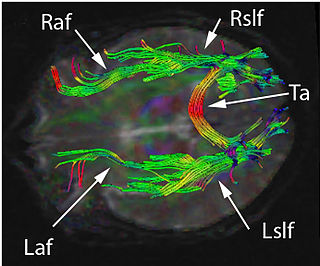
The commissural fibers or transverse fibers are axons that connect the two hemispheres of the brain. In contrast to commissural fibers, association fibers connect regions within the same hemisphere of the brain, and projection fibers connect each region to other parts of the brain or to the spinal cord.

Hemianopsia, or hemianopia, is a visual field loss on the left or right side of the vertical midline. It can affect one eye but usually affects both eyes.
Posterior cerebral artery syndrome is a condition whereby the blood supply from the posterior cerebral artery (PCA) is restricted, leading to a reduction of the function of the portions of the brain supplied by that vessel: the occipital lobe, the inferomedial temporal lobe, a large portion of the thalamus, and the upper brainstem and midbrain.
Deep dyslexia is a form of dyslexia that disrupts reading processes. Deep dyslexia may occur as a result of a head injury, stroke, disease, or operation. This injury results in the occurrence of semantic errors during reading and the impairment of nonword reading.
Auditory agnosia is a form of agnosia that manifests itself primarily in the inability to recognize or differentiate between sounds. It is not a defect of the ear or "hearing", but rather a neurological inability of the brain to process sound meaning. While auditory agnosia impairs the understanding of sounds, other abilities such as reading, writing, and speaking are not hindered. It is caused by bilateral damage to the anterior superior temporal gyrus, which is part of the auditory pathway responsible for sound recognition, the auditory "what" pathway.
The history of dyslexia research spans from the late 1800s to the present.
Phonological dyslexia is a reading disability that is a form of alexia, resulting from brain injury, stroke, or progressive illness and that affects previously acquired reading abilities. The major distinguishing symptom of acquired phonological dyslexia is that a selective impairment of the ability to read pronounceable non-words occurs although the ability to read familiar words is not affected. It has also been found that the ability to read non-words can be improved if the non-words belong to a family of pseudohomophones.

The visual word form area (VWFA) is a functional region of the left fusiform gyrus and surrounding cortex that is hypothesized to be involved in identifying words and letters from lower-level shape images, prior to association with phonology or semantics. Because the alphabet is relatively new in human evolution, it is unlikely that this region developed as a result of selection pressures related to word recognition per se; however, this region may be highly specialized for certain types of shapes that occur naturally in the environment and are therefore likely to surface within written language.
The neuronal recycling hypothesis was proposed by Stanislas Dehaene in the field of cognitive neuroscience in an attempt to explain the underlying neural processes which allow humans to acquire recently invented cognitive capacities. This hypothesis was formulated in response to the 'reading paradox', which states that these cognitive processes are cultural inventions too modern to be the products of evolution. The paradox lies within the fact that cross-cultural evidence suggests specific brain areas are associated with these functions. The concept of neuronal recycling resolves this paradox by suggesting that novel functions actually utilize and 'recycle' existing brain circuitry. Once these cognitive functions find a cortical area devoted to a similar purpose, they can invade the existing circuit. Through plasticity, the cortex can adapt in order to accommodate for these novel functions.
Disconnection syndrome is a general term for a collection of neurological symptoms caused – via lesions to associational or commissural nerve fibres – by damage to the white matter axons of communication pathways in the cerebrum, independent of any lesions to the cortex. The behavioral effects of such disconnections are relatively predictable in adults. Disconnection syndromes usually reflect circumstances where regions A and B still have their functional specializations except in domains that depend on the interconnections between the two regions.
The occipital face area (OFA) is a region of the human cerebral cortex which is specialised for face perception. The OFA is located on the lateral surface of the occipital lobe adjacent to the inferior occipital gyrus. The OFA comprises a network of brain regions including the fusiform face area (FFA) and posterior superior temporal sulcus (STS) which support facial processing.
References
- 1 2 3 Coslett HB (2000). "Acquired dyslexia". Semin Neurol. 20 (4): 419–26. doi:10.1055/s-2000-13174. PMID 11149697. S2CID 36969285.
- ↑ Behrmann M, Shomstein SS, Black SE, Barton JJ (2001). "The eye movements of pure alexic patients during reading and nonreading tasks". Neuropsychologia. 39 (9): 983–1002. doi:10.1016/S0028-3932(01)00021-5. PMID 11516450. S2CID 9526540.
- ↑ Fiset D, Arguin M, Bub D, Humphreys GW, Riddoch MJ (July 2005). "How to make the word-length effect disappear in letter-by-letter dyslexia: implications for an account of the disorder". Psychol Sci. 16 (7): 535–41. doi:10.1111/j.0956-7976.2005.01571.x. PMID 16008786. S2CID 34286805.
- ↑ Warrington EK, Langdon D (February 1994). "Spelling dyslexia: a deficit of the visual word-form". J. Neurol. Neurosurg. Psychiatry. 57 (2): 211–6. doi:10.1136/jnnp.57.2.211. PMC 1072453 . PMID 8126508.
- ↑ Warrington EK, Shallice T (March 1980). "Word-form dyslexia". Brain. 103 (1): 99–112. doi:10.1093/brain/103.1.99. PMID 6244876.
- ↑ Imtiaz KE, Nirodi G, Khaleeli AA (2001). "Alexia without agraphia: a century later". Int. J. Clin. Pract. 55 (3): 225–6. doi:10.1111/j.1742-1241.2001.tb11019.x. PMID 11351780. S2CID 39921061.
- ↑ Temple CM (August 2006). "Developmental and acquired dyslexias". Cortex. 42 (6): 898–910. doi:10.1016/S0010-9452(08)70434-9. PMID 17131596. S2CID 4490916.
- ↑ Carlson, Neil R. (2013). Physiology of behavior (11th ed.). Boston: Pearson. p. 501. ISBN 978-0-205-23939-9.
- 1 2 3 4 5 Kim, E. S., Rising, K., Rapcsak, S. Z., & Beeson, P. M. (2015). "Treatment for Alexia With Agraphia Following Left Ventral Occipito-Temporal Damage: Strengthening Orthographic Representations Common to Reading and Spelling". Journal of Speech, Language, and Hearing Research. 58 (5): 1521–1537. doi:10.1044/2015_JSLHR-L-14-0286. PMC 4686312 . PMID 26110814.
{{cite journal}}: CS1 maint: multiple names: authors list (link) - 1 2 3 4 Petersen, A.; Vangkilde, S.; Fabricius, C.; Iversen, H. K.; Delfi, T. S.; Starrfelt, R. (2016). "Visual attention in posterior stroke and relations to alexia". Neuropsychologia. 92: 79–89. doi:10.1016/j.neuropsychologia.2016.02.029. PMID 26970141. S2CID 8938987.
- 1 2 "Imaging". 30 March 2015.
- ↑ Sundsten, John W.; Nolte, John (2001). The human brain: an introduction to its functional anatomy. St. Louis: Mosby. p. 552. ISBN 978-0-323-01320-8. OCLC 48416194.
- ↑ "Baylor Neurology Case of the Month". Archived from the original on 2007-05-10. Retrieved 2007-06-07.
- ↑ Nolte, John (2009). The human brain: an introduction to its functional anatomy. St. Louis, Mo: Mosby/Elsevier. p. 571. ISBN 978-0-323-04131-7. OCLC 181903953.
- ↑ "Alexia". Cognitive Neuropsychology Laboratory. Center for Aphasia Research and Rehabilitation. Retrieved 30 March 2015.
- ↑ Montant, Marie; Behrmann, Marlene (2000). "Pure Alexia" (PDF). Neurocase. 6 (4): 265–294. doi:10.1080/13554790008402777. S2CID 220357240 . Retrieved 30 March 2015.
- ↑ Epelbaum, S. (2008). "Pure alexia as a disconnection syndrome: New diffusion imaging evidence for an old concept". Cortex. 44 (8): 962–974. doi:10.1016/j.cortex.2008.05.003. PMID 18586235. S2CID 14956468.
- ↑ Roberts, DJ; Woollams, AM; Kim, E; Beeson, PM; Rapcsak, SZ; Lambon Ralph, MA (24 August 2012). "Efficient Visual Object and Word Recognition Relies on High Spatial Frequency Coding in the Left Posterior Fusiform Gyrus: Evidence from a Case-Series of Patients with Ventral Occipito-Temporal Cortex Damage". Cerebral Cortex. 23 (11): 2568–2580. doi:10.1093/cercor/bhs224. PMC 3792736 . PMID 22923086.
- ↑ Roberts, DJ; Lambon Ralph, MA; Kim, ES; Tainturier, MJ; Beeson, PM; Rapcsak, SZ; Woollams, AM (November 2015). "Processing deficits for familiar and novel faces in patients with left posterior fusiform lesions". Cortex. 72: 79–96. doi:10.1016/j.cortex.2015.02.003. PMC 4643682 . PMID 25837867.
- ↑ Cohen, L. (2000). "Calculating Without Reading: Unsuspected Residual Abilities In Pure Alexia". Cognitive Neuropsychology. 17 (6): 563–583. doi:10.1080/02643290050110656. PMID 20945195. S2CID 926892.
- ↑ Roberts, DJ; Lambon Ralph, MA; Woollams, AM (July 2010). "When does less yield more? The impact of severity upon implicit recognition in pure alexia". Neuropsychologia. 48 (9): 2437–2446. doi:10.1016/j.neuropsychologia.2010.04.002. PMID 20406652. S2CID 29783028.
- ↑ Coslett, H.B. (1989). "Evidence For Preserved Reading In 'Pure Alexia'". Brain. 112 (2): 327–359. doi:10.1093/brain/112.2.327. PMID 2706436.
- ↑ Leff, Alexander P.; Schofield, T. M. "Rehabilitation of acquired alexia". International Encyclopedia of Rehabilitation. Center for International Rehabilitation Research Information and Exchange. Retrieved 30 March 2015.