Related Research Articles

Hyperthyroidism is the condition that occurs due to excessive production of thyroid hormones by the thyroid gland. Thyrotoxicosis is the condition that occurs due to excessive thyroid hormone of any cause and therefore includes hyperthyroidism. Some, however, use the terms interchangeably. Signs and symptoms vary between people and may include irritability, muscle weakness, sleeping problems, a fast heartbeat, heat intolerance, diarrhea, enlargement of the thyroid, hand tremor, and weight loss. Symptoms are typically less severe in the elderly and during pregnancy. An uncommon but life-threatening complication is thyroid storm in which an event such as an infection results in worsening symptoms such as confusion and a high temperature; this often results in death. The opposite is hypothyroidism, when the thyroid gland does not make enough thyroid hormone.

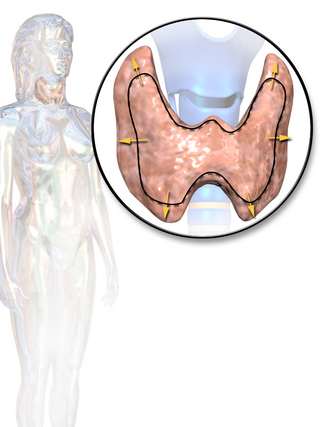
The thyroid, or thyroid gland, is an endocrine gland in vertebrates. In humans, it is in the neck and consists of two connected lobes. The lower two thirds of the lobes are connected by a thin band of tissue called the isthmus (pl.: isthmi). The thyroid gland is a butterfly-shaped gland located in the neck below the Adam's apple. Microscopically, the functional unit of the thyroid gland is the spherical thyroid follicle, lined with follicular cells (thyrocytes), and occasional parafollicular cells that surround a lumen containing colloid. The thyroid gland secretes three hormones: the two thyroid hormones – triiodothyronine (T3) and thyroxine (T4) – and a peptide hormone, calcitonin. The thyroid hormones influence the metabolic rate and protein synthesis and growth and development in children. Calcitonin plays a role in calcium homeostasis. Secretion of the two thyroid hormones is regulated by thyroid-stimulating hormone (TSH), which is secreted from the anterior pituitary gland. TSH is regulated by thyrotropin-releasing hormone (TRH), which is produced by the hypothalamus.

Graves' disease, also known as toxic diffuse goiter, is an autoimmune disease that affects the thyroid. It frequently results in and is the most common cause of hyperthyroidism. It also often results in an enlarged thyroid. Signs and symptoms of hyperthyroidism may include irritability, muscle weakness, sleeping problems, a fast heartbeat, poor tolerance of heat, diarrhea and unintentional weight loss. Other symptoms may include thickening of the skin on the shins, known as pretibial myxedema, and eye bulging, a condition caused by Graves' ophthalmopathy. About 25 to 30% of people with the condition develop eye problems.
Hypothyroidism is a disorder of the endocrine system in which the thyroid gland does not produce enough thyroid hormones. It can cause a number of symptoms, such as poor ability to tolerate cold, extreme fatigue, muscle aches, constipation, slow heart rate, depression, and weight gain. Occasionally there may be swelling of the front part of the neck due to goitre. Untreated cases of hypothyroidism during pregnancy can lead to delays in growth and intellectual development in the baby or congenital iodine deficiency syndrome.

Iodothyronine deiodinases (EC 1.21.99.4 and EC 1.21.99.3) are a subfamily of deiodinase enzymes important in the activation and deactivation of thyroid hormones. Thyroxine (T4), the precursor of 3,5,3'-triiodothyronine (T3) is transformed into T3 by deiodinase activity. T3, through binding a nuclear thyroid hormone receptor, influences the expression of genes in practically every vertebrate cell. Iodothyronine deiodinases are unusual in that these enzymes contain selenium, in the form of an otherwise rare amino acid selenocysteine.

Congenital hypothyroidism (CH) is thyroid hormone deficiency present at birth. If untreated for several months after birth, severe congenital hypothyroidism can lead to growth failure and permanent intellectual disability. Infants born with congenital hypothyroidism may show no effects, or may display mild effects that often go unrecognized as a problem. Significant deficiency may cause excessive sleeping, reduced interest in nursing, poor muscle tone, low or hoarse cry, infrequent bowel movements, significant jaundice, and low body temperature.
Thyroid-stimulating hormone (also known as thyrotropin, thyrotropic hormone, or abbreviated TSH) is a pituitary hormone that stimulates the thyroid gland to produce thyroxine (T4), and then triiodothyronine (T3) which stimulates the metabolism of almost every tissue in the body. It is a glycoprotein hormone produced by thyrotrope cells in the anterior pituitary gland, which regulates the endocrine function of the thyroid.
Triiodothyronine, also known as T3, is a thyroid hormone. It affects almost every physiological process in the body, including growth and development, metabolism, body temperature, and heart rate.

Hashimoto's thyroiditis, also known as chronic lymphocytic thyroiditis and Hashimoto's disease, is an autoimmune disease in which the thyroid gland is gradually destroyed. A slightly broader term is autoimmune thyroiditis, identical other than that it is also used to describe a similar condition without a goiter.

Levothyroxine, also known as L-thyroxine, is a synthetic form of the thyroid hormone thyroxine (T4). It is used to treat thyroid hormone deficiency (hypothyroidism), including a severe form known as myxedema coma. It may also be used to treat and prevent certain types of thyroid tumors. It is not indicated for weight loss. Levothyroxine is taken orally (by mouth) or given by intravenous injection. Levothyroxine has a half-life of 7.5 days when taken daily, so about six weeks is required for it to reach a steady level in the blood.
Thyroid disease is a medical condition that affects the function of the thyroid gland. The thyroid gland is located at the front of the neck and produces thyroid hormones that travel through the blood to help regulate many other organs, meaning that it is an endocrine organ. These hormones normally act in the body to regulate energy use, infant development, and childhood development.
Carbimazole (brand names Neo-Mercazole, Anti-Thyrox, etc.) is used to treat hyperthyroidism. Carbimazole is a pro-drug as after absorption it is converted to the active form, methimazole. Methimazole prevents thyroid peroxidase enzyme from iodinating and coupling the tyrosine residues on thyroglobulin, hence reducing the production of the thyroid hormones T3 and T4 (thyroxine).
Thyroid storm is a rare but severe and life-threatening complication of hyperthyroidism. It occurs when an overactive thyroid leads to hypermetabolism, which can cause death from cardiac arrest or multiple organ failure.
Liothyronine is a manufactured form of the thyroid hormone triiodothyronine (T3). It is most commonly used to treat hypothyroidism and myxedema coma. It can be taken by mouth or by injection into a vein.
Thyroid function tests (TFTs) is a collective term for blood tests used to check the function of the thyroid. TFTs may be requested if a patient is thought to suffer from hyperthyroidism or hypothyroidism, or to monitor the effectiveness of either thyroid-suppression or hormone replacement therapy. It is also requested routinely in conditions linked to thyroid disease, such as atrial fibrillation and anxiety disorder.

The hypothalamic–pituitary–thyroid axis is part of the neuroendocrine system responsible for the regulation of metabolism and also responds to stress.
An antithyroid agent is a hormone inhibitor acting upon thyroid hormones.
Euthyroid sick syndrome (ESS) is a state of adaptation or dysregulation of thyrotropic feedback control wherein the levels of T3 and/or T4 are abnormal, but the thyroid gland does not appear to be dysfunctional. This condition may result from allostatic responses of hypothalamus-pituitary-thyroid feedback control, dyshomeostatic disorders, drug interferences, and impaired assay characteristics in critical illness.
Thyroid hormones are any hormones produced and released by the thyroid gland, namely triiodothyronine (T3) and thyroxine (T4). They are tyrosine-based hormones that are primarily responsible for regulation of metabolism. T3 and T4 are partially composed of iodine, derived from food. A deficiency of iodine leads to decreased production of T3 and T4, enlarges the thyroid tissue and will cause the disease known as simple goitre.
Thyroid disease in pregnancy can affect the health of the mother as well as the child before and after delivery. Thyroid disorders are prevalent in women of child-bearing age and for this reason commonly present as a pre-existing disease in pregnancy, or after childbirth. Uncorrected thyroid dysfunction in pregnancy has adverse effects on fetal and maternal well-being. The deleterious effects of thyroid dysfunction can also extend beyond pregnancy and delivery to affect neurointellectual development in the early life of the child. Due to an increase in thyroxine binding globulin, an increase in placental type 3 deioidinase and the placental transfer of maternal thyroxine to the fetus, the demand for thyroid hormones is increased during pregnancy. The necessary increase in thyroid hormone production is facilitated by high human chorionic gonadotropin (hCG) concentrations, which bind the TSH receptor and stimulate the maternal thyroid to increase maternal thyroid hormone concentrations by roughly 50%. If the necessary increase in thyroid function cannot be met, this may cause a previously unnoticed (mild) thyroid disorder to worsen and become evident as gestational thyroid disease. Currently, there is not enough evidence to suggest that screening for thyroid dysfunction is beneficial, especially since treatment thyroid hormone supplementation may come with a risk of overtreatment. After women give birth, about 5% develop postpartum thyroiditis which can occur up to nine months afterwards. This is characterized by a short period of hyperthyroidism followed by a period of hypothyroidism; 20–40% remain permanently hypothyroid.
References
- 1 2 3 4 5 6 7 8 9 10 11 12 "Thyroid Monograph for Professionals". Drugs.com. American Society of Health-System Pharmacists. Retrieved 8 April 2019.
- ↑ "Thyroid desiccated Use During Pregnancy". Drugs.com. Retrieved 9 April 2019.
- 1 2 Jameson JL, Groot LJ (2010). Endocrinology - E-Book: Adult and Pediatric. Elsevier Health Sciences. p. 1608. ISBN 9781455711260.
- ↑ Thomas JA, Keenan EJ (2012). Principles of Endocrine Pharmacology. Springer Science & Business Media. p. 78. ISBN 9781468450361.
- ↑ "The Top 300 of 2021". ClinCalc. Archived from the original on 15 January 2024. Retrieved 14 January 2024.
- ↑ "Thyroid - Drug Usage Statistics". ClinCalc. Retrieved 14 January 2024.
- ↑ Garber JR, Cobin RH, Gharib H, Hennessey JV, Klein I, Mechanick JI, et al. (December 2012). "Clinical practice guidelines for hypothyroidism in adults: cosponsored by the American Association of Clinical Endocrinologists and the American Thyroid Association" (PDF). Thyroid. 22 (12): 1200–1235. doi:10.1089/thy.2012.0205. PMID 22954017. Archived from the original (PDF) on 14 January 2016. Retrieved 8 November 2014.
- ↑ "Thyroid disorders 'misdiagnosed'". BBC News. 27 March 2009. Retrieved 30 March 2009.
the only accurate way to diagnose a thyroid disorder is via a blood test which measures hormone levels, and the only scientifically proven way of treating the condition is by topping up a patient's natural thyroxine levels with a synthetic form of the hormone.
- 1 2 "Endocrine Today Blog". Endocrinetoday.com. Retrieved 24 July 2014.
- ↑ Repas, Thomas. Desiccated thyroid in the management of hypothyroidism: Part I.
- ↑ Baskin HJ, Cobin RH, Duick DS, Gharib H, Guttler RB, Kaplan MM, Segal RL (2002). "American Association of Clinical Endocrinologists medical guidelines for clinical practice for the evaluation and treatment of hyperthyroidism and hypothyroidism" (PDF). Endocrine Practice. 8 (6): 457–469. doi:10.4158/1934-2403-8.6.457. PMID 15260011. Archived from the original (PDF) on 8 December 2015. Retrieved 3 February 2015.
- ↑ Clyde PW, Harari AE, Getka EJ, Shakir KM (December 2003). "Combined levothyroxine plus liothyronine compared with levothyroxine alone in primary hypothyroidism: a randomized controlled trial". JAMA. 290 (22): 2952–2958. doi:10.1001/jama.290.22.2952. PMID 14665656.
- ↑ "Endocrine Today Blog". Endocrinetoday.com. Retrieved 24 July 2014.
- ↑ "Endocrine Today Blog". Endocrinetoday.com. Retrieved 24 July 2014.
- ↑ US Pharmacopeia Natural Formulary USP 37 N32 2014 Volume 3 May 1, 2014. The United States Pharmacopeial Convention. 2014. ISBN 9781936424221.
- ↑ Tory DB (2006). Remington The Science and Practice of Pharmacy (21st ed.). Philadelphia, PA: Lippincott Williams and Wilkins. pp. 1460, 1461. ISBN 0781763789.
- ↑ Murray GR. The life history of the first case of myxoedema treated by thyroid extract. Br Med J 1920;i:359-60.
- ↑ Burgess AM. Myxedema-- controlled by thyroid extract for fifty-two years: report of a case. Ann Internal Med 1946; 25:146.
- ↑ Means JH, DeGroot LJ, Stanbury JB. The Thyroid and its Diseases. 3rd ed. New York:McGraw Hill, 1963. See chapter 9 for a lengthy discussion of the difficulties of assessing treatment in the era before effective tests, as well as the doctors' impressions of the superiority of the new synthetic thyroxine that had just become available.
- ↑ Macgregor AG (February 1961). "Why does anybody use thyroid B.P.?". Lancet. 1 (7172): 329–332. doi:10.1016/s0140-6736(61)91498-2. PMID 13764789.
- ↑ Catz B, Ginsburg E, Salenger S (January 1962). "Clinically inactive thyroid U.S.P. A preliminary report". The New England Journal of Medicine. 266: 136–137. doi:10.1056/nejm196201182660308. PMID 13877407.
- ↑ Pileggi VJ, Golub OJ, Lee ND (July 1965). "Determination of Thyroxine and Triiodothyronine in Commercial Preparations of Desiccated Thyroid and Thyroid Extract". The Journal of Clinical Endocrinology and Metabolism. 25 (7): 949–956. doi:10.1210/jcem-25-7-949. PMID 14319377.
- ↑ Mangieri CN, Lund MH (January 1970). "Potency of United States Pharmacopeia dessicated thyroid tablets as determined by the antigoitrogenic assay in rats". The Journal of Clinical Endocrinology and Metabolism. 30 (1): 102–104. doi: 10.1210/jcem-30-1-102 . PMID 5409525.
- ↑ Rees-Jones RW, Rolla AR, Larsen PR (February 1980). "Hormonal content of thyroid replacement preparations". JAMA. 243 (6): 549–550. doi:10.1001/jama.1980.03300320041023. PMID 7351788.
- ↑ Braverman LE, Ingbar SH, Sterling K (May 1970). "Conversion of thyroxine (T4) to triiodothyronine (T3) in athyreotic human subjects". The Journal of Clinical Investigation. 49 (5): 855–864. doi: 10.1172/jci106304 . PMC 535757 . PMID 4986007.
- ↑ Saberi M, Utiger RD (November 1974). "Serum thyroid hormone and thyrotropin concentrations during thyroxine and triiodothyronine therapy". The Journal of Clinical Endocrinology and Metabolism. 39 (5): 923–927. doi:10.1210/jcem-39-5-923. PMID 4422006.
- ↑ Penny R, Frasier SD (January 1980). "Elevated serum concentrations of triiodothyronine in hypothyroid patients. Values for patients receiving USP thyroid". American Journal of Diseases of Children. 134 (1): 16–18. doi:10.1001/archpedi.1980.02130130008003. PMID 7350782.
- 1 2 Capiferri R, Evered D (March 1979). "Investigation and treatment of hypothyroidism". Clinics in Endocrinology and Metabolism. 8 (1): 39–48. doi:10.1016/S0300-595X(79)80008-0. PMID 371874.
- ↑ Surks MI, Schadlow AR, Oppenheimer JH (December 1972). "A new radioimmunoassay for plasma L-triiodothyronine: measurements in thyroid disease and in patients maintained on hormonal replacement". The Journal of Clinical Investigation. 51 (12): 3104–3113. doi: 10.1172/jci107137 . PMC 332992 . PMID 4539287.