
Breast reconstruction is the surgical process of rebuilding the shape and look of a breast, most commonly in women who have had surgery to treat breast cancer. It involves using autologous tissue, prosthetic implants, or a combination of both with the goal of reconstructing a natural-looking breast. This process often also includes the rebuilding of the nipple and areola, known as nipple-areola complex (NAC) reconstruction, as one of the final stages.

Breast cancer is a cancer that develops from breast tissue. Signs of breast cancer may include a lump in the breast, a change in breast shape, dimpling of the skin, milk rejection, fluid coming from the nipple, a newly inverted nipple, or a red or scaly patch of skin. In those with distant spread of the disease, there may be bone pain, swollen lymph nodes, shortness of breath, or yellow skin.
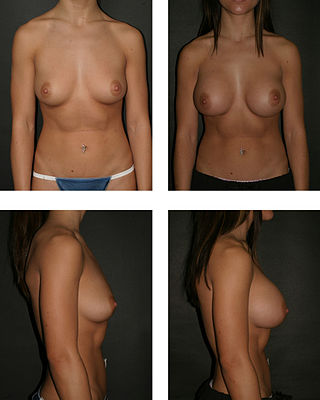
Breast augmentation and augmentation mammoplasty is a cosmetic surgery technique using breast-implants and fat-graft mammoplasty techniques to increase the size, change the shape, and alter the texture of the breasts. Augmentation mammoplasty is applied to correct congenital defects of the breasts and the chest wall. As an elective cosmetic surgery, primary augmentation changes the aesthetics – of size, shape, and texture – of healthy breasts.

Paget's disease of the breast is a rare skin change at the nipple nearly always associated with underlying breast cancer. Paget's disease of the breast was first described by Sir James Paget in 1874. The condition is an uncommon disease accounting for 1 to 4% of all breast cancers cases. 92% to 100% of patients with Paget's disease of the breast have an underlying breast cancer.

Lymphadenectomy, or lymph node dissection, is the surgical removal of one or more groups of lymph nodes. It is almost always performed as part of the surgical management of cancer. In a regional lymph node dissection, some of the lymph nodes in the tumor area are removed; in a radical lymph node dissection, most or all of the lymph nodes in the tumor area are removed.

Lumpectomy is a surgical removal of a discrete portion or "lump" of breast tissue, usually in the treatment of a malignant tumor or breast cancer. It is considered a viable breast conservation therapy, as the amount of tissue removed is limited compared to a full-breast mastectomy, and thus may have physical and emotional advantages over more disfiguring treatment. Sometimes a lumpectomy may be used to either confirm or rule out that cancer has actually been detected. A lumpectomy is usually recommended to patients whose cancer has been detected early and who do not have enlarged tumors. Although a lumpectomy is used to allow for most of the breast to remain intact, the procedure may result in adverse affects that can include sensitivity and result in scar tissue, pain, and possible disfiguration of the breast if the lump taken out is significant. According to National Comprehensive Cancer Network guidelines, lumpectomy may be performed for ductal carcinoma in situ (DCIS), invasive ductal carcinoma, or other conditions.

Invasive carcinoma of no special type, invasive breast carcinoma of no special type (IBC-NST), invasive ductal carcinoma (IDC), infiltrating ductal carcinoma (IDC) or invasive ductal carcinoma, not otherwise specified (NOS) is a disease. For international audiences this article will use "invasive carcinoma NST" because it is the preferred term of the World Health Organization (WHO).

Radical mastectomy is a surgical procedure that treats breast cancer by removing the breast and its underlying chest muscle, and lymph nodes of the axilla (armpit). Breast cancer is the most common cancer among women. During the early twentieth century it was primarily treated by surgery, when the mastectomy was developed. However, with the advancement of technology and surgical skills in recent years, mastectomies have become less invasive. As of 2016, a combination of radiotherapy and breast conserving mastectomy are considered optimal treatment.

A breast implant is a prosthesis used to change the size, shape, and contour of a person's breast. In reconstructive plastic surgery, breast implants can be placed to restore a natural looking breast following a mastectomy, to correct congenital defects and deformities of the chest wall or, cosmetically, to enlarge the appearance of the breast through breast augmentation surgery.

Ductal carcinoma in situ (DCIS), also known as intraductal carcinoma, is a pre-cancerous or non-invasive cancerous lesion of the breast. DCIS is classified as Stage 0. It rarely produces symptoms or a breast lump that can be felt, typically being detected through screening mammography. It has been diagnosed in a significant percentage of men.
Breast cancer management takes different approaches depending on physical and biological characteristics of the disease, as well as the age, over-all health and personal preferences of the patient. Treatment types can be classified into local therapy and systemic treatment. Local therapy is most efficacious in early stage breast cancer, while systemic therapy is generally justified in advanced and metastatic disease, or in diseases with specific phenotypes.
Breast-conserving surgery refers to an operation that aims to remove breast cancer while avoiding a mastectomy. Different forms of this operation include: lumpectomy (tylectomy), wide local excision, segmental resection, and quadrantectomy. Breast-conserving surgery has been increasingly accepted as an alternative to mastectomy in specific patients, as it provides tumor removal while maintaining an acceptable cosmetic outcome. This page reviews the history of this operation, important considerations in decision making and patient selection, and the emerging field of oncoplastic breast conservation surgery.
A DIEP flap is type of breast reconstruction where blood vessels, fat, and skin from the lower belly are relocated to the chest to rebuild breasts after mastectomy. DIEP stands for the deep inferior epigastric perforator artery, which runs through the abdomen. This is a type of autologous reconstruction, meaning one's own tissue is used.

Male breast cancer (MBC) is a cancer in males that originates in their breasts. Males account for less than 1% of new breast cancers with about 20,000 new cases being diagnosed worldwide every year. Its incidence rates in males vs. females are, respectively, 0.4 and 66.7 per 100,000 person-years. The worldwide incidences of male as well as female breast cancers have been increasing over the last few decades. Currently, one of every 800 men are estimated to develop this cancer during their lifetimes.
Bernard Fisher was an American surgeon and a pioneer in the biology and treatment of breast cancer. He was a native of Pittsburgh. He was Chairman of the National Surgical Adjuvant Breast Project at the University of Pittsburgh School of Medicine. His work established definitively that early-stage breast cancer could be more effectively treated by lumpectomy, in combination with radiation therapy, chemotherapy, and/or hormonal therapy, than by radical mastectomy.

Nipple/Areola prostheses are made of silicone by breast prosthesis manufacturers and anaplastologists for breast cancer survivors who were treated for breast cancer with a mastectomy. Prostheses can be worn weeks after a mastectomy, breast reconstruction, or even nipple reconstruction. As an inexpensive and convenient alternative to surgery, patients may choose to wear them anytime during treatment. Patients who ultimately find nipple prostheses thought that they should be informed of them during the consultation prior to mastectomy.
Anne Louise Rosenberg is an American surgical oncologist retired from practice in Cherry Hill, New Jersey.

Armando Elario Giuliano is a surgical oncologist, surgeon scientist and medical professor in Los Angeles, California, United States of America. He is the Linda and Jim Lippman Chair in Surgical Oncology and co-director of Saul and Joyce Brandman Breast Center at Cedars-Sinai Medical Center, Los Angeles.
Mammary secretory carcinoma (MSC), also termed secretory carcinoma of the breast, is a rare form of the breast cancers. MSC usually affects women but in a significant percentage of cases also occurs in men and children. Indeed, McDvitt and Stewart first described MSC in 1966 and termed it juvenile breast carcinoma because an increased number of cases were at that time diagnosed in juvenile females. MSC is the most common form of breast cancer in children, representing 80% of childhood breast cancers, although it accounts for less than 0.15% of all breast cancers.
Papillary carcinomas of the breast (PCB), also termed malignant papillary carcinomas of the breast, are rare forms of the breast cancers. The World Health Organization (2019) classified papillary neoplasms of the breast into 5 types: intraductal papilloma, papillary ductal carcinoma in situ (PDCIS), encapsulated papillary carcinoma (EPC), solid-papillary carcinoma (SPC), and invasive papillary carcinoma (IPC). The latter four carcinomas are considered here; intraductal papilloma is a benign neoplasm. The World Health Organization regarded solid papillary carcinoma as having two subtypes: in situ and invasive SPC.





