Related Research Articles
The term abdominal surgery broadly covers surgical procedures that involve opening the abdomen (laparotomy). Surgery of each abdominal organ is dealt with separately in connection with the description of that organ Diseases affecting the abdominal cavity are dealt with generally under their own names.
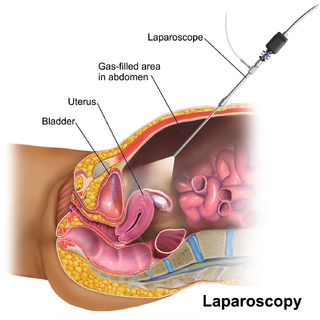
Laparoscopy is an operation performed in the abdomen or pelvis using small incisions with the aid of a camera. The laparoscope aids diagnosis or therapeutic interventions with a few small cuts in the abdomen.

Appendicitis is inflammation of the appendix. Symptoms commonly include right lower abdominal pain, nausea, vomiting, and decreased appetite. However, approximately 40% of people do not have these typical symptoms. Severe complications of a ruptured appendix include widespread, painful inflammation of the inner lining of the abdominal wall and sepsis.

Peritonitis is inflammation of the localized or generalized peritoneum, the lining of the inner wall of the abdomen and cover of the abdominal organs. Symptoms may include severe pain, swelling of the abdomen, fever, or weight loss. One part or the entire abdomen may be tender. Complications may include shock and acute respiratory distress syndrome.

An appendectomy or appendicectomy is a surgical operation in which the vermiform appendix is removed. Appendectomy is normally performed as an urgent or emergency procedure to treat complicated acute appendicitis.

Hysterectomy is the partial or total surgical removal of the uterus. It may also involve removal of the cervix, ovaries (oophorectomy), fallopian tubes (salpingectomy), and other surrounding structures. Partial hysterectomies allow for hormone regulation while total hysterectomies do not.
Perioperative mortality has been defined as any death, regardless of cause, occurring within 30 days after surgery in or out of the hospital. Globally, 4.2 million people are estimated to die within 30 days of surgery each year. An important consideration in the decision to perform any surgical procedure is to weigh the benefits against the risks. Anesthesiologists and surgeons employ various methods in assessing whether a patient is in optimal condition from a medical standpoint prior to undertaking surgery, and various statistical tools are available. ASA score is the most well known of these.

Uterine rupture is when the muscular wall of the uterus tears during pregnancy or childbirth. Symptoms, while classically including increased pain, vaginal bleeding, or a change in contractions, are not always present. Disability or death of the mother or baby may result.
Hemoperitoneum is the presence of blood in the peritoneal cavity. The blood accumulates in the space between the inner lining of the abdominal wall and the internal abdominal organs. Hemoperitoneum is generally classified as a surgical emergency; in most cases, urgent laparotomy is needed to identify and control the source of the bleeding. In selected cases, careful observation may be permissible. The abdominal cavity is highly distensible and may easily hold greater than five liters of blood, or more than the entire circulating blood volume for an average-sized individual. Therefore, large-scale or rapid blood loss into the abdomen will reliably induce hemorrhagic shock and, if untreated, may rapidly lead to death.
Diagnostic peritoneal lavage (DPL) or diagnostic peritoneal aspiration (DPA) is a surgical diagnostic procedure to determine if there is free floating fluid in the abdominal cavity.

Retropubic space is a potential avascular space located between the pubic symphysis and the urinary bladder. The retropubic space is a preperitoneal space, located behind the transversalis fascia and in front of peritoneum.
Tubal reversal, also called tubal sterilization reversal, tubal ligation reversal, or microsurgical tubal reanastomosis, is a surgical procedure that can restore fertility to women after a tubal ligation. By rejoining the separated segments of the fallopian tube, tubal reversal can give women the chance to become pregnant again. In some cases, however, the separated segments cannot actually be reattached to each other. In some cases the remaining segment of tube needs to be re-implanted into the uterus. In other cases, when the end of the tube has been removed, a procedure called a neofimbrioplasty must be performed to recreate a functional end of the tube which can then act like the missing fimbria and retrieve the egg that has been released during ovulation.

A Pfannenstiel incision, Kerr incision, Pfannenstiel-Kerr incision or pubic incision is a type of abdominal surgical incision that allows access to the abdomen. It is used for gynecologic and orthopedics surgeries, and it is the most common method for performing Caesarian sections today. This incision is also used in Stoppa approach for orthopedics surgeries to treat pelvic fractures.
An obturator hernia is a rare type of hernia, encompassing 0.07-1% of all hernias, of the pelvic floor in which pelvic or abdominal contents protrudes through the obturator foramen. The obturator foramen is formed by a branch of the ischial as well as the pubic bone. The canal is typically 2-3 centimeters long and 1 centimeters wide, creating a space for pouches of pre-peritoneal fat.

Abdominal trauma is an injury to the abdomen. Signs and symptoms include abdominal pain, tenderness, rigidity, and bruising of the external abdomen. Complications may include blood loss and infection.
A lower (uterine) segment Caesarean section (LSCS) is the most commonly used type of Caesarean section. Most commonly to deliver the baby a transverse incision is made in the lower uterine segment above the attachment of the urinary bladder to the uterus. This type of incision results in less blood loss and is easier to repair than other types of Caesarean sections.
An exploratory laparotomy is a general surgical operation where the abdomen is opened and the abdominal organs are examined for injury or disease. It is the standard of care in various blunt and penetrating trauma situations in which there may be life-threatening internal injuries. It is also used in certain diagnostic situations, in which the operation is undertaken in search of a unifying cause for multiple signs and symptoms of disease, and in the staging of some cancers.
In surgery, a surgical incision is a cut made through the skin and soft tissue to facilitate an operation or procedure. Often, multiple incisions are possible for an operation. In general, a surgical incision is made as small and unobtrusive as possible to facilitate safe and timely operating conditions.
The Cherney incision is an incision used in gynecologic surgery. It is similar to the Pfannenstiel incision but allows access to the space of Retzius and gives a larger area in which to operate.
Maylard incision is a surgical incision in which a transverse cut is made on rectus abdominis muscle to allow wider access to the pelvic cavity. It is also called Mackenrodt incision. For gynaecological surgery, the skin incision is made 5–8 cm above the pubic symphysis. The site of skin incision is above and parallel to traditional Pfannenstiel incision. The rectus fascia and muscle are cut transversely and the incision is extended as far laterally as needed. The anterior rectus sheath is not separated from the muscle to facilitate easy closure at the end of the surgical procedure. The inferior epigastric vessels which span across more than half of the rectus muscle's width are identified and ligated. In patients with peripheral arterial disease, ligation of inferior epigastric vessels may lead to distal ischemia. Finally, the peritoneum is cut laterally.
References
- ↑ Quebbeman, Frances Elizabeth (1966). "Medicine In Territorial Arizona" (PDF). University of Arizona. Archived (PDF) from the original on 10 December 2013. Retrieved 7 December 2013.
- ↑ "Henry George Liddell, Robert Scott, A Greek-English Lexicon, λ , λα_ο-σεβής , λα^πάρα_". www.perseus.tufts.edu. Retrieved 2018-08-02.
- ↑ synd/1010 at Who Named It?
- ↑ Williams GR (May 1983). "Presidential Address: a history of appendicitis. With anecdotes illustrating its importance" (PDF). Annals of Surgery. 197 (5): 495–506. doi:10.1097/00000658-198305000-00001. PMC 1353017 . PMID 6342553. Archived from the original (PDF) on 2018-09-04. Retrieved 2017-03-01.
- ↑ synd/2500 at Who Named It?
- ↑ Pfannenstiel HJ (1900). "Ueber die Vortheile des suprasymphysären Fascienquerschnitts für die gynäkologischen Koeliotomien" [On the Advantages of the Suprasymphyseal Fascia Cross Section for Gynecological Coeliotomies]. (Volkmann's) Sammlung Klinischer Vorträge (in German). Leipzig. 268 (Gynäk. Nr. 97): 1735–1756.
- ↑ Giacalone PL, Daures JP, Vignal J, Herisson C, Hedon B, Laffargue F (May 2002). "Pfannenstiel versus Maylard incision for cesarean delivery: A randomized controlled trial". Obstetrics and Gynecology. 99 (5 Pt 1): 745–50. doi:10.1016/S0029-7844(02)01957-9. PMID 11978282. S2CID 12855909.
- ↑ Slater SD (June 1994). "Alfred Ernest Maylard, 1855-1947: Glasgow surgeon extraordinaire". Scottish Medical Journal. 39 (3): 86–90. doi:10.1177/003693309403900312. PMID 8720774. S2CID 21365098.
- ↑ Bajpai M, Kumar A, Gupta AK, Pawar DK (June 2004). "Lumbotomy approach for upper urological tract surgery in children--an analysis of 68 consecutive lumbotomies". European Journal of Pediatric Surgery. 14 (3): 163–7. doi:10.1055/s-2004-820903. PMID 15211405.
- ↑ Tizzano AP, Muffly TM (2007). "Historical milestones in female pelvic surgery, gynecology, and female urology." (PDF). Urogynecology and Reconstructive Pelvic Surgery (3rd ed.). pp. 3–15. Archived from the original (PDF) on 2015-05-01. Retrieved 2017-03-02.
- ↑ Javanmard-Emamghissi, Hannah (2023). "Quantitative futility in emergency laparotomy: an exploration of early-postoperative death in the National Emergency Laparotomy Audit". Techniques in Coloproctology. 27 (9): 729–738. doi: 10.1007/s10151-022-02747-1 . PMC 10404199 . PMID 36609892.
- ↑ GlobalSurg Collaborative (July 2016). "Mortality of emergency abdominal surgery in high-, middle- and low-income countries". The British Journal of Surgery. 103 (8): 971–988. doi:10.1002/bjs.10151. hdl: 20.500.11820/7c4589f5-7845-4405-a384-dfb5653e2163 . PMID 27145169. S2CID 20764511.
- ↑ GlobalSurg Collaborative (2016). "Determinants of morbidity and mortality following emergency abdominal surgery in children in low-income and middle-income countries". BMJ Global Health. 1 (4): e000091. doi:10.1136/bmjgh-2016-000091. PMC 5321375 . PMID 28588977.
- ↑ Gershkovich, Pavel; Itin, Constantin; Yacovan, Avihai; Amselem, Shimon; Hoffman, Amnon (2009-03-31). "Effect of abdominal surgery on the intestinal absorption of lipophilic drugs: possible role of the lymphatic transport". Translational Research. 153 (6): 296–300. doi:10.1016/J.TRSL.2009.02.008. PMID 19446284.
- ↑ Gurusamy KS, Cassar Delia E, Davidson BR (July 2013). Cochrane Wounds Group (ed.). "Peritoneal closure versus no peritoneal closure for patients undergoing non-obstetric abdominal operations". The Cochrane Database of Systematic Reviews. 2019 (7): CD010424. doi:10.1002/14651858.CD010424.pub2. PMC 6353057 . PMID 23828487.