
General surgery is a surgical specialty that focuses on alimentary canal and abdominal contents including the esophagus, stomach, small intestine, large intestine, liver, pancreas, gallbladder, appendix and bile ducts, and often the thyroid gland. General surgeons also deal with diseases involving the skin, breast, soft tissue, trauma, peripheral artery disease and hernias and perform endoscopic as such as gastroscopy, colonoscopy and laparoscopic procedures.

The pancreas is an organ of the digestive system and endocrine system of vertebrates. In humans, it is located in the abdomen behind the stomach and functions as a gland. The pancreas is a mixed or heterocrine gland, i.e., it has both an endocrine and a digestive exocrine function. 99% of the pancreas is exocrine and 1% is endocrine. As an endocrine gland, it functions mostly to regulate blood sugar levels, secreting the hormones insulin, glucagon, somatostatin and pancreatic polypeptide. As a part of the digestive system, it functions as an exocrine gland secreting pancreatic juice into the duodenum through the pancreatic duct. This juice contains bicarbonate, which neutralizes acid entering the duodenum from the stomach; and digestive enzymes, which break down carbohydrates, proteins and fats in food entering the duodenum from the stomach.

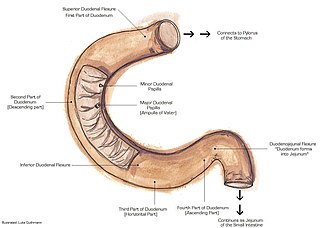
The duodenum is the first section of the small intestine in most higher vertebrates, including mammals, reptiles, and birds. In mammals it may be the principal site for iron absorption. The duodenum precedes the jejunum and ileum and is the shortest part of the small intestine.

The small intestine or small bowel is an organ in the gastrointestinal tract where most of the absorption of nutrients from food takes place. It lies between the stomach and large intestine, and receives bile and pancreatic juice through the pancreatic duct to aid in digestion. The small intestine is about 5.5 metres long and folds many times to fit in the abdomen. Although it is longer than the large intestine, it is called the small intestine because it is narrower in diameter.

Pancreatic cancer arises when cells in the pancreas, a glandular organ behind the stomach, begin to multiply out of control and form a mass. These cancerous cells have the ability to invade other parts of the body. A number of types of pancreatic cancer are known.

Cholecystectomy is the surgical removal of the gallbladder. Cholecystectomy is a common treatment of symptomatic gallstones and other gallbladder conditions. In 2011, cholecystectomy was the eighth most common operating room procedure performed in hospitals in the United States. Cholecystectomy can be performed either laparoscopically, or via an open surgical technique.
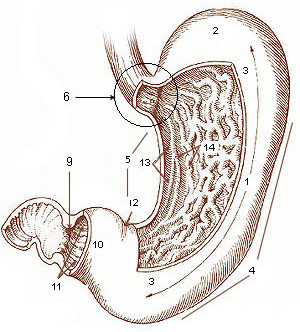
A gastrectomy is a partial or total surgical removal of the stomach.
The suspensory muscle of duodenum is a thin muscle connecting the junction between the duodenum and jejunum, as well as the duodenojejunal flexure to connective tissue surrounding the superior mesenteric and coeliac arteries. The suspensory muscle most often connects to both the third and fourth parts of the duodenum, as well as the duodenojejunal flexure, although the attachment is quite variable.
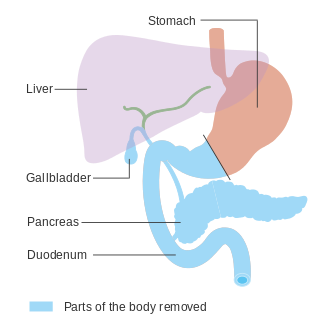
In medicine, a pancreatectomy is the surgical removal of all or part of the pancreas. Several types of pancreatectomy exist, including pancreaticoduodenectomy, distal pancreatectomy, segmental pancreatectomy, and total pancreatectomy. In recent years, the TP-IAT has also gained respectable traction within the medical community. These procedures are used in the management of several conditions involving the pancreas, such as benign pancreatic tumors, pancreatic cancer, and pancreatitis.
The Kocher manoeuvre is a surgical procedure to expose structures in the retroperitoneum behind the duodenum and pancreas. In vascular surgery, it is described as a method to expose the abdominal aorta. It usually has been in contrast to midline laparotomy and right retroperitoneal space dissection. These two procedures have been used for diverse cases, but have approximately equivalent outcomes.
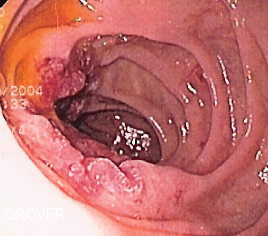
Duodenal cancer is a cancer in the first section of the small intestine known as the duodenum. Cancer of the duodenum is relatively rare compared to stomach cancer and colorectal cancer. Its histology is usually adenocarcinoma.

The inferior pancreaticoduodenal artery is a branch of the superior mesenteric artery. It supplies the head of the pancreas, and the ascending and inferior parts of the duodenum. Rarely, it may have an aneurysm.

Hemosuccus pancreaticus is a rare cause of hemorrhage in the gastrointestinal tract. It is caused by a bleeding source in the pancreas, pancreatic duct, or structures adjacent to the pancreas, such as the splenic artery, that bleed into the pancreatic duct, which is connected with the bowel at the duodenum, the first part of the small intestine. Patients with hemosuccus may develop symptoms of gastrointestinal hemorrhage, such as blood in the stools, maroon stools, or melena, which is a dark, tarry stool caused by digestion of red blood cells. They may also develop abdominal pain. It is associated with pancreatitis, pancreatic cancer and aneurysms of the splenic artery. Hemosuccus may be identified with endoscopy (esophagogastroduodenoscopy), where fresh blood may be seen from the pancreatic duct. Alternatively, angiography may be used to inject the celiac axis to determine the blood vessel that is bleeding. This may also be used to treat hemosuccus, as embolization of the end vessel may terminate the hemorrhage. However, a distal pancreatectomy—surgery to remove of the tail of the pancreas—may be required to stop the hemorrhage.
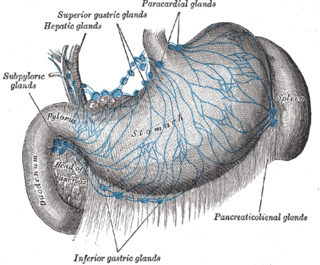
The hepatic lymph nodes consist of the following groups:

In general surgery, a Roux-en-Y anastomosis, or Roux-en-Y, is an end-to-side surgical anastomosis of bowel used to reconstruct the gastrointestinal tract. Typically, it is between stomach and small bowel that is distal from the cut end.

Periampullary cancer is a cancer that forms near the ampulla of Vater, an enlargement of the ducts from the liver and pancreas where they join and enter the small intestine. It consists of:
- ampullary tumour from ampulla of Vater
- cancer of lower common bile duct
- duodenal cancer adjacent to ampulla
- carcinoma head of pancreas
An exploratory laparotomy is a general surgical operation where the abdomen is opened and the abdominal organs are examined for injury or disease. It is the standard of care in various blunt and penetrating trauma situations in which there may be life-threatening internal injuries. It is also used in certain diagnostic situations, in which the operation is undertaken in search of a unifying cause for multiple signs and symptoms of disease, and in the staging of some cancers.
A pancreatic injury is some form of trauma sustained by the pancreas. The injury can be sustained through either blunt forces, such as a motor vehicle accident, or penetrative forces, such as that of a gunshot wound. The pancreas is one of the least commonly injured organs in abdominal trauma.

Choledochoduodenostomy (CDD) is a surgical procedure to create an anastomosis, a surgical connection, between the common bile duct (CBD) and an alternative portion of the duodenum. In healthy individuals, the CBD meets the pancreatic duct at the ampulla of Vater, which drains via the major duodenal papilla to the second part of duodenum. In cases of benign conditions such as narrowing of the distal CBD or recurrent CBD stones, performing a CDD provides the diseased patient with CBD drainage and decompression. A side-to-side anastomosis is usually performed.

Antrectomy, also called distal gastrectomy, is a type of gastric resection surgery that involves the removal of the stomach antrum to treat gastric diseases causing the damage, bleeding, or blockage of the stomach. This is performed using either the Billroth I (BI) or Billroth II (BII) reconstruction method. Quite often, antrectomy is used alongside vagotomy to maximise its safety and effectiveness. Modern antrectomies typically have a high success rate and low mortality rate, but the exact numbers depend on the specific conditions being treated.


