Related Research Articles

In vertebrates, the gallbladder, also known as the cholecyst, is a small hollow organ where bile is stored and concentrated before it is released into the small intestine. In humans, the pear-shaped gallbladder lies beneath the liver, although the structure and position of the gallbladder can vary significantly among animal species. It receives bile, produced by the liver, via the common hepatic duct, and stores it. The bile is then released via the common bile duct into the duodenum, where the bile helps in the digestion of fats.

A bile duct is any of a number of long tube-like structures that carry bile, and is present in most vertebrates. The bile duct is separated into three main parts: the fundus (superior), the body (middle), and the neck (inferior).
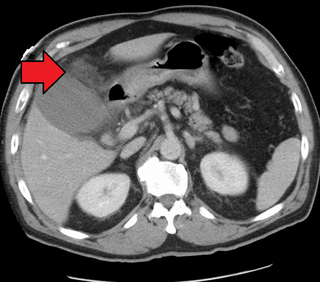
Cholecystitis is inflammation of the gallbladder. Symptoms include right upper abdominal pain, pain in the right shoulder, nausea, vomiting, and occasionally fever. Often gallbladder attacks precede acute cholecystitis. The pain lasts longer in cholecystitis than in a typical gallbladder attack. Without appropriate treatment, recurrent episodes of cholecystitis are common. Complications of acute cholecystitis include gallstone pancreatitis, common bile duct stones, or inflammation of the common bile duct.

In medicine, a stent is a tube usually constructed of a metallic alloy or a polymer. It is inserted into the lumen of an anatomic vessel or duct to keep the passageway open. Stenting refers to the placement of a stent. The word "stent" is also used as a verb to describe the placement of such a device, particularly when a disease such as atherosclerosis has pathologically narrowed a structure such as an artery.

Interventional radiology (IR) is a medical specialty that performs various minimally-invasive procedures using medical imaging guidance, such as x-ray fluoroscopy, computed tomography, magnetic resonance imaging, or ultrasound. IR performs both diagnostic and therapeutic procedures through very small incisions or body orifices. Diagnostic IR procedures are those intended to help make a diagnosis or guide further medical treatment, and include image-guided biopsy of a tumor or injection of an imaging contrast agent into a hollow structure, such as a blood vessel or a duct. By contrast, therapeutic IR procedures provide direct treatment—they include catheter-based medicine delivery, medical device placement, and angioplasty of narrowed structures.

Cholecystectomy is the surgical removal of the gallbladder. Cholecystectomy is a common treatment of symptomatic gallstones and other gallbladder conditions. In 2011, cholecystectomy was the eighth most common operating room procedure performed in hospitals in the United States. Cholecystectomy can be performed either laparoscopically, or via an open surgical technique.

Endoscopic retrograde cholangiopancreatography (ERCP) is a technique that combines the use of endoscopy and fluoroscopy to diagnose and treat certain problems of the biliary or pancreatic ductal systems. It is primarily performed by highly skilled and specialty trained gastroenterologists. Through the endoscope, the physician can see the inside of the stomach and duodenum, and inject a contrast medium into the ducts in the biliary tree and pancreas so they can be seen on radiographs.
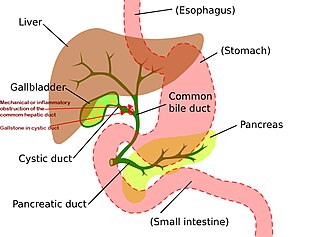
Mirizzi's syndrome is a rare complication in which a gallstone becomes impacted in the cystic duct or neck of the gallbladder causing compression of the common hepatic duct, resulting in obstruction and jaundice. The obstructive jaundice can be caused by direct extrinsic compression by the stone or from fibrosis caused by chronic cholecystitis (inflammation). A cholecystocholedochal fistula can occur.

Common bile duct stone, also known as choledocholithiasis, is the presence of gallstones in the common bile duct (CBD). This condition can cause jaundice and liver cell damage. Treatments include choledocholithotomy and endoscopic retrograde cholangiopancreatography (ERCP).

Gallbladder cancer is a relatively uncommon cancer, with an incidence of fewer than 2 cases per 100,000 people per year in the United States. It is particularly common in central and South America, central and eastern Europe, Japan and northern India; it is also common in certain ethnic groups e.g. Native American Indians and Hispanics. If it is diagnosed early enough, it can be cured by removing the gallbladder, part of the liver and associated lymph nodes. Most often it is found after symptoms such as abdominal pain, jaundice and vomiting occur, and it has spread to other organs such as the liver.

Ascending cholangitis, also known as acute cholangitis or simply cholangitis, is inflammation of the bile duct, usually caused by bacteria ascending from its junction with the duodenum. It tends to occur if the bile duct is already partially obstructed by gallstones.
Biliary colic, also known as symptomatic cholelithiasis, a gallbladder attack or gallstone attack, is when a colic occurs due to a gallstone temporarily blocking the cystic duct. Typically, the pain is in the right upper part of the abdomen, and can be severe. Pain usually lasts from 15 minutes to a few hours. Often, it occurs after eating a heavy meal, or during the night. Repeated attacks are common. Cholecystokinin - a gastrointestinal hormone - plays a role in the colic, as following the consumption of fatty meals, the hormone triggers the gallbladder to contract, which may expel stones into the duct and temporarily block it until being successfully passed.

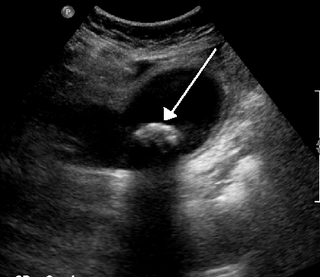
Gallbladder diseases are diseases involving the gallbladder and is closely linked to biliary disease, with the most common cause being gallstones (cholelithiasis).

Percutaneous transhepatic cholangiography, percutaneous hepatic cholangiogram (PTHC) is a radiological technique used to visualize the anatomy of the biliary tract. A contrast medium is injected into a bile duct in the liver, after which X-rays are taken. It allows access to the biliary tree in cases where endoscopic retrograde cholangiopancreatography has been unsuccessful. Initially reported in 1937, the procedure became popular in 1952.
Therapeutic endoscopy is the medical term for an endoscopic procedure during which treatment is carried out via the endoscope. This contrasts with diagnostic endoscopy, where the aim of the procedure is purely to visualize a part of the gastrointestinal, respiratory or urinary tract in order to aid diagnosis. In practice, a procedure which starts as a diagnostic endoscopy may become a therapeutic endoscopy depending on the findings, such as in cases of upper gastrointestinal bleeding, or the finding of polyps during colonoscopy.

Biliary sludge refers to a viscous mixture of small particles derived from bile. These sediments consist of cholesterol crystals, calcium salts, calcium bilirubinate, mucin, and other materials.

Michel Kahaleh is an American gastroenterologist and an expert in therapeutic endoscopy.

A biloma is a circumscribed abdominal collection of bile outside the biliary tree. It occurs when there is excess bile in the abdominal cavity. It can occur during or after a bile leak. There is an increased chance of a person developing biloma after having a gallbladder removal surgery, known as laparoscopic cholecystectomy. This procedure can be complicated by biloma with incidence of 0.3–2%. Other causes are liver biopsy, abdominal trauma, and, rarely, spontaneous perforation. The formation of biloma does not occur frequently. Biliary fistulas are also caused by injury to the bile duct and can result in the formation of bile leaks. Biliary fistulas are abnormal communications between organs and the biliary tract. Once diagnosed, they usually require drainage. The term "biloma" was first coined in 1979 by Gould and Patel. They discovered it in a case with extrahepatic bile leakage. The cause of this was trauma to the upper right quadrant of the abdomen. Originally, biloma was described as an "encapsulated collection" of extrahepatic bile. Biloma is now described as extrabiliary collections of bile that can be either intrahepatic or extrahepatic. The most common cause of biloma is trauma to the liver. There are other causes such as abdominal surgery, endoscopic surgery and percutaneous catheter drainage. Injury and abdominal trauma can cause damage to the biliary tree. The biliary tree is a system of vessels that direct secreations from the liver, gallbladder, and pancreas through a series of ducts into the duodenum. This can result in a bile leak which is a common cause of the formation of biloma. It is possible for biloma to be associated with mortality, though it is not common. Bile leaks occur in about one percent of causes.

Choledochoduodenostomy (CDD) is a surgical procedure to create an anastomosis, a surgical connection, between the common bile duct (CBD) and an alternative portion of the duodenum. In healthy individuals, the CBD meets the pancreatic duct at the ampulla of Vater, which drains via the major duodenal papilla to the second part of duodenum. In cases of benign conditions such as narrowing of the distal CBD or recurrent CBD stones, performing a CDD provides the diseased patient with CBD drainage and decompression. A side-to-side anastomosis is usually performed.
Biliary endoscopic sphincterotomy is a procedure where the sphincter of Oddi and the segment of the common bile duct where it enters the duodenum are cannulated and then cut with a sphincterotome, a device that includes a wire which cuts with an electric current (electrocautery).
References
- ↑ Kelly, Howard A.; Burrage, Walter L. (eds.). . . Baltimore: The Norman, Remington Company.
- ↑ Bulletin of the Johns Hopkins Hospital, Vol. 12. Baltimore: The Johns Hopkins Press. Aug 1901. p. 249.
- 1 2 3 4 Irani, Shayan S.; Sharzehi, Kaveh; Siddiqui, Uzma D. (May 2023). "AGA Clinical Practice Update on Role of EUS-Guided Gallbladder Drainage in Acute Cholecystitis: Commentary". Clinical Gastroenterology and Hepatology. 21 (5): 1141–1147. doi:10.1016/j.cgh.2022.12.039. ISSN 1542-3565.
- ↑ Bakkaloglu H, Yanar H, Guloglu R, et al. (November 2006). "Ultrasound guided percutaneous cholecystostomy in high-risk patients for surgical intervention". World J. Gastroenterol. 12 (44): 7179–82. doi: 10.3748/wjg.v12.i44.7179 . PMC 4087782 . PMID 17131483.
- ↑ Baron TH, Topazian MD, et al. (April 2007). "Endoscopic transduodenal drainage of the gallbladder: implications for endoluminal treatment of gallbladder disease". Gastrointest. Endosc. 65 (4): 735–7. doi:10.1016/j.gie.2006.07.041. PMID 17141230.
- 1 2 3 4 5 6 7 Baron, Todd H.; Grimm, Ian S.; Swanstrom, Lee L. (2015-07-23). Campion, Edward W. (ed.). "Interventional Approaches to Gallbladder Disease". New England Journal of Medicine. 373 (4): 357–365. doi:10.1056/NEJMra1411372. ISSN 0028-4793.
- 1 2 3 4 5 6 Venara, A.; Carretier, V.; Lebigot, J.; Lermite, E. (2014-12-01). "Technique and indications of percutaneous cholecystostomy in the management of cholecystitis in 2014". Journal of Visceral Surgery. 151 (6): 435–439. doi:10.1016/j.jviscsurg.2014.06.003. ISSN 1878-7886.
- 1 2 3 4 5 6 Arkoudis, Nikolaos-Achilleas; Moschovaki-Zeiger, Ornella; Reppas, Lazaros; Grigoriadis, Stavros; Alexopoulou, Efthymia; Brountzos, Elias; Kelekis, Nikolaos; Spiliopoulos, Stavros (2023-10-01). "Percutaneous cholecystostomy: techniques and applications". Abdominal Radiology. 48 (10): 3229–3242. doi:10.1007/s00261-023-03982-2. ISSN 2366-0058.
- 1 2 3 4 5 6 7 8 9 Bashir, Omar. "Percutaneous cholecystostomy | Radiology Reference Article | Radiopaedia.org". Radiopaedia. Retrieved 2023-11-13.
- 1 2 3 Karakas, Hakki (2021). "Percutaneous Cholecystostomy: An Update for the 2020s". Northern Clinics of Istanbul. doi:10.14744/nci.2021.81594. PMC 8630714 . PMID 34909596.
- 1 2 Wise, James N.; Gervais, Debra A.; Akman, Andrew; Harisinghani, Mukesh; Hahn, Peter F.; Mueller, Peter R. (May 2005). "Percutaneous Cholecystostomy Catheter Removal and Incidence of Clinically Significant Bile Leaks: A Clinical Approach to Catheter Management". American Journal of Roentgenology. 184 (5): 1647–1651. doi:10.2214/ajr.184.5.01841647. ISSN 0361-803X.