Gastrointestinal stromal tumors (GISTs) are the most common mesenchymalneoplasms of the gastrointestinal tract. GISTs arise in the smooth muscle pacemaker interstitial cell of Cajal, or similar cells.[2] They are defined as tumors whose behavior is driven by mutations in the KIT gene (85%),[2]PDGFRA gene (10%),[2] or BRAF kinase (rare).[2] 95% of GISTs stain positively for KIT (CD117).[2][3] Most (66%) occur in the stomach and gastric GISTs have a lower malignant potential than tumors found elsewhere in the GI tract.[3]
GIST was introduced as a diagnostic term in 1983.[2]:1060 Until the late 1990s, many non-epithelialtumors of the gastrointestinal tract were called "gastrointestinal stromal tumors". Histopathologists were unable to specifically distinguish among types now known to be dissimilar molecularly. Subsequently, CD34, and later CD117, were identified as markers that could distinguish the various types.[citation needed] Additionally, in the absence of specific therapy, the diagnostic categorization had only a limited influence on prognosis and therapy.
The understanding of GIST biology changed significantly with identification of the molecular basis of GIST,[2]:1065 particularly c-KIT. Historically, literature reviews prior to the molecular definition of GIST, and for a short time thereafter, asserted that 70-80% of GISTs were benign.[4][5][6] The identification of a molecular basis for GIST led to the exclusion of many tumors that had been considered as GIST previously, and also the incorporation of a much larger number of tumors that had been labeled as other types of sarcomas and undifferentiated carcinomas.[2]:1065 For example, some previous diagnoses of stomach and small bowel leiomyosarcomas (malignant tumor of smooth muscle) would be reclassified as GISTs on the basis of immunohistochemical staining. All GIST tumors are now considered to have malignant potential, and no GIST tumor can be definitively classified as "benign".[7] Hence, all GISTs are eligible for cancer staging in the AJCC (7th edition) / UICC.[8] Nonetheless, different GISTs have different risk assessments of their tendency to recur or to metastasize, dependent on their site of origin, size, and number of mitotic figures.
Due to the change in definition, clinical pathways of care before the year 2000 are largely uninformative in the current era.[2]
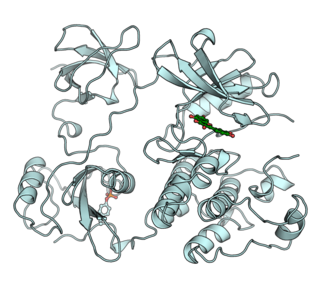
Approximately 85% GISTs are associated with an abnormal c-KIT pathway. c-KIT is a gene that encodes for a transmembrane receptor for a growth factor termed stem cell factor (scf). The abnormal c-KIT pathway most commonly (85%) arises from mutation of the gene itself; a smaller subset of c-KIT-associated GISTs are associated with constitutive activity of the KITenzymatic pathway, found by immunoblotting.[2]:1062 The c-KIT product/CD117 is expressed on ICCs and a large number of other cells, mainly bone marrow cells, mast cells, melanocytes and several others. In the gut, however, a mass staining positive for CD117 is likely to be a GIST, arising from ICC cells.
The c-KIT molecule comprises a long extracellular domain, a transmembrane segment, and an intracellular part. Mutations generally occur in the DNA encoding the intracellular part (exon 11), which acts as a tyrosine kinase to activate other enzymes. Mutations make c-KITfunction independent of activation by scf, leading to a high cell division rate and possibly genomic instability. Additional mutations are likely "required" for a cell with a c-KIT mutation to develop into a GIST, but the c-KIT mutation is probably the first step of this process.
Mutations in the exons 11, 9 and rarely 13 and 17 of the c-KIT gene are known to occur in GIST. The tyrosine kinase function of c-KIT is important in the medical therapy for GISTs, as described below.
KIT-D816V point mutations in c-KIT exon 17 are responsible for resistance to targeted therapy drugs like imatinib mesylate, a tyrosine kinase inhibitor.
KIT-p.D419del (exon 8) — A subset of gastrointestinal stromal tumors previously regarded as wild-type tumors carries somatic activating mutations in KIT exon 8 (p.D419del).[12]
PDGFRA mutations
Most GIST cells with wildtype (i.e. not mutated) c-KIT instead have a mutation in another gene, PDGFR-α (platelet-derived growth factor receptor alpha), which is a related tyrosine kinase. Mutations in c-KIT and PDGFrA are mutually exclusive [dead link].
Wild-type tumors
Lesser numbers of GISTs appear to be associated with neither c-KIT nor PDGFR-α abnormalities.[2]:1062 About 10-15% of gastrointestinal stromal tumors (GISTs) carry wild-type sequences in all hot spots of KIT and platelet-derived growth factor receptor alpha (PDGFRA) (wt-GISTs). These tumors are currently defined by having no mutations in exons 9, 11, 13, and 17 of the KIT gene and exons 12, 14, and 18 of the PDGFRA gene.[12]
Diagnosis
Endoscopic image of GIST in fundus of stomach, seen on retroflexion.Same GIST seen on forward view of the endoscope showing overlying clot.
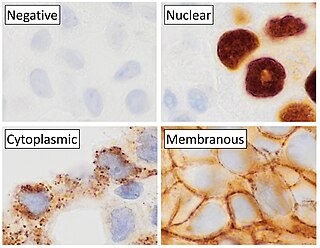
Negative immunohistochemistry staining for β-catenin in cell nuclei is a consistent finding in uterine leiomyomas, and helps in distinguishing such tumors from β-catenin positive spindle cell tumors.[13]
The definitive diagnosis is made with a biopsy, which can be obtained endoscopically, percutaneously with CT or ultrasound guidance or at the time of surgery. A biopsy sample will be investigated under the microscope by a pathologist physician. The pathologist examines the histopathology to identify the characteristics of GISTs (spindle cells in 70-80%, epitheloid aspect in 20-30%). Smaller tumors can usually be confined to the muscularis propria layer of the intestinal wall. Large ones grow, mainly outward, from the bowel wall until the point where they outstrip their blood supply and necrose (die) on the inside, forming a cavity that may eventually come to communicate with the bowel lumen.
When GIST is suspected—as opposed to other causes for similar tumors—the pathologist can use immunohistochemistry (specific antibodies that stain the molecule CD117 [also known as c-KIT] —see below). 95% of all GISTs are CD117-positive (other possible markers include CD34, DOG-1, desmin, and vimentin). Other cells that show CD117 positivity are mast cells.
If the CD117 stain is negative and suspicion remains that the tumor is a GIST, the newer antibody DOG-1 (Discovered On GIST-1) can be used. Also, sequencing of KIT and PDGFRA can be used to prove the diagnosis.
Imaging
The purpose of radiologic imaging is to locate the lesion, evaluate for signs of invasion and detect metastasis. Features of GIST vary depending on tumor size and organ of origin. The diameter can range from a few millimeters to more than 30cm. Larger tumors usually cause symptoms in contrast to those found incidentally which tend to be smaller and have better prognosis.[4][14] Large tumors tend to exhibit malignant behavior but small GISTs may also demonstrate clinically aggressive behavior.[15]
CT image of a GIST in the gastric cardia. The lesion appears submucosal, is hypervascular and protrudes intraluminally. Upper GI bleeding led to endoscopy, finding an ulcerated mass.Non-enhanced CT image of a small GIST in the posterior stomach wall (arrow). The lesion appears subserosal. Incidental finding.
Plain radiographs are not very helpful in the evaluation of GISTs. If an abnormality is seen, it will be an indirect sign due to the tumor mass effect on adjacent organs. On abdominal x-ray, stomach GISTs may appear as a radiopaque mass altering the shape of the gastric air shadow. Intestinal GISTs may displace loops of bowel and larger tumors may obstruct the bowel and films will show an obstructive pattern. If cavitations are present, plain radiographs will show collections of air within the tumor.[16]Calcification is an unusual feature of GIST but if present can be visible on plain films.
Barium fluoroscopic examinations and CT are commonly used to evaluate the patient with abdominal complaints. Barium swallow images show abnormalities in 80% of GIST cases.[15] However, some GISTs may be located entirely outside the lumen of the bowel and will not be appreciated with a barium swallow. Even in cases when the barium swallow is abnormal, an MRI or CT scan must follow since it is impossible to evaluate abdominal cavities and other abdominal organs with a barium swallow alone. In a CT scan, abnormalities may be seen in 87% of patients and it should be made with both oral and intravenous contrast.[15] Among imaging studies, MRI has the best tissue contrast, which aids in the identification of masses within the GI tract (intramural masses). Intravenous contrast material is needed to evaluate lesion vascularity.
Preferred imaging modalities in the evaluation of GISTs are CT and MRI,[17]:20–21 and, in selected situations, endoscopic ultrasound. CT advantages include its ability to demonstrate evidence of nearby organ invasion, ascites, and metastases. The ability of an MRI to produce images in multiple planes is helpful in determining the bowel as the organ of origin (which is difficult when the tumor is very large), facilitating diagnosis.
Immunohistochemistry for β-catenin in GIST, which is negative as there is only staining of cytoplasm but not of cell nuclei. Negative nuclear β-catenin staining is seen in approximately 95% of GIST cases, and helps in distinguishing such tumors from β-catenin positive spindle cell tumors.
Small GISTs
Since GISTs arise from the bowel layer called muscularis propria (which is deeper to the mucosa and submucosa from a luminal perspective), small GIST imaging usually suggest a submucosal process or a mass within the bowel wall. In barium swallow studies, these GISTs most commonly present with smooth borders forming right or obtuse angles with the nearby bowel wall, as seen with any other intramural mass. The mucosal surface is usually intact except for areas of ulceration, which are generally present in 50% of GISTs. Ulcerations fill with barium causing a bull's eye or target lesion appearance. In contrast-enhanced CT, small GISTs are seen as smooth, sharply defined intramural masses with homogeneous attenuation.
Large GISTs
As the tumor grows it may project outside the bowel (exophytic growth) and/or inside the bowel (intraluminal growth), but they most commonly grow exophytically such that the bulk of the tumor projects into the abdominal cavity. If the tumor outstrips its blood supply, it can necrose internally, creating a central fluid-filled cavity with bleeding and cavitations that can eventually ulcerate and communicate into the lumen of the bowel. In that case, barium swallow may show an air, air-fluid levels or oral contrast media accumulation within these areas.[15][19] Mucosal ulcerations may also be present. In contrast-enhanced CT images, large GISTs appear as heterogeneous masses due to areas of living tumor cells surrounding bleeding, necrosis or cysts, which is radiographically seen as a peripheral enhancement pattern with a low attenuation center.[14] In MRI studies, the degree of necrosis and bleeding affects the signal intensity pattern. Areas of bleeding within the tumor will vary its signal intensity depending on how long ago the bleeding occurred. The solid portions of the tumor are typically low signal intensity on T1-weighted images, are high signal intensity on T2-weighted images and enhanced after administration of gadolinium. Signal-intensity voids are present if there is gas within areas of necrotic tumor.[16][20][21]
Features of malignancy
Malignancy is characterized by local invasion and metastases, usually to the liver, omentum and peritoneum. However, cases of metastases to bone, pleura, lungs and retroperitoneum have been seen. In distinction to gastric adenocarcinoma or gastric/small bowel lymphoma, malignant lymphadenopathy (swollen lymph nodes) is uncommon (<10%) and thus imaging usually shows absence of lymph node enlargement.[14] If metastases are not present, other radiologic features suggesting malignancy include: size (>5cm), heterogeneous enhancement after contrast administration, and ulcerations.[4][14][22] Also, overtly malignant behavior (in distinction to malignant potential of lesser degree) is less commonly seen in gastric tumors, with a ratio of behaviorally benign to overtly malignant of 3-5:1.[4] Even if radiographic malignant features are present, these findings may also represent other tumors and definitive diagnosis must be made immunochemically.
Management
Image showing Gastrointestinal Stromal Tumor after surgical removal
For localized, resectable adult GISTs, if anatomically and physiologically feasible, surgery is the primary treatment of choice.[17]:69 Surgery can be potentially curative, but watchful waiting may be considered in small tumors in carefully selected situations.[23] Post-surgical adjuvant treatment may be recommended.[24] Lymph node metastases are rare, and routine removal of lymph nodes is typically not necessary. Laparoscopic surgery, a minimally invasive abdominal surgery using telescopes and specialized instruments, has been shown to be effective for removal of these tumors without needing large incisions.[25] The clinical issues of exact surgical indications for tumor size are controversial. The decision of appropriate laparoscopic surgery is affected by tumor size, location, and growth pattern.[26]
Radiotherapy has not historically been effective for GISTs[27]:1122 and GISTs do not respond to most chemotherapy medications,[27]:1122 with responses in less than 5%.[2]:1065 However, several medications have been identified for clinical benefit in GIST: imatinib, sunitinib, regorafenib, ripretinib and avapritinib.
Imatinib (Glivec/Gleevec), an orally administered drug initially marketed for chronic myelogenous leukemia based on bcr-abl inhibition, also inhibits both c-KITtyrosine kinase mutations and PDGFRA mutations other than D842V, and is useful in treating GISTs in several situations. Imatinib has been used in selected neoadjuvant settings.[28][17]:23 In the adjuvant treatment setting, the majority of GIST tumors are cured by surgery, and do not need adjuvant therapy.[29][30] An exception to this is where the anatomical position of the tumour means that surgery is technically difficult or complex. For example, rectal GIST often requires radical surgery to achieve complete resection, involving abdominoperineal resection and permanent stoma. In these situations, the use of neoadjuvant imatinib can significantly decrease both tumour size and mitotic activity, and permit less radical sphincter-preserving surgery.[28]
A substantial proportion of GIST tumors have a high risk of recurrence as estimated by a number of validated risk stratification schemes, and can be considered for adjuvant therapy.[30][31] The selection criteria underpinning the decision for possible use of imatinib in these settings, including a risk assessment based on pathological factors such as tumor size, mitotic rate and location, can be used to predict the risk of recurrence in GIST patients. Tumors <2cm with a mitotic rate of <5/50 HPF have been shown to have lower risk of recurrence than larger or more aggressive tumors. Following surgical resection of GISTs, adjuvant treatment with imatinib reduces the risk of disease recurrence in higher risk groups.[citation needed] In selected higher risk adjuvant situations, imatinib is recommended for 3 years.[32]
Imatinib was approved for metastatic and unresectable GIST by the US FDA, February 1, 2002. The two-year survival of patients with advanced disease has risen to 75–80% following imatinib treatment.[33]
If resistance to imatinib is encountered, the multiple tyrosine kinase inhibitor sunitinib (marketed as Sutent) can be considered.[17]:26 and 31[34]
The effectiveness of imatinib and sunitinib depend on the genotype.[35] c-KIT- and PDGFRA-mutation negative GIST tumors are usually resistant to treatment with imatinib,[11] as is neurofibromatosis-1-associated wild-type GIST.[30] A specific subtype of PDGFRA mutation, D842V, is also insensitive to imatinib.[30][36] Recently, in PDGFRA-mutated GIST, avapritinib has been approved by FDA.[37] Now there are real-world data coming for avapritinib as well[38]
Regorafenib (Stivarga) was FDA-approved in 2013 for advanced GISTs that cannot be surgically removed and that no longer respond to imatinib (Gleevec) and sunitinib (Sutent).[39]
Epidemiology
GISTs occur in 10-20 per one million people. The true incidence might be higher, as novel laboratory methods are much more sensitive in diagnosing GISTs.[citation needed] The estimated incidence of GIST in the United States is approximately 5000 cases annually.[2]:1063 This makes GIST the most common form of sarcoma, which constitutes more than 70 types of cancer.
The majority of GISTs present at ages 50–70 years. Across most of the age spectrum, the incidence of GIST is similar in men and women.[27]:1122
Adult GISTs are rare before age 40. Pediatric GISTs are considered to be biologically distinct.[40] Unlike GISTs at other ages, pediatric GISTs are more common in girls and young women. They appear to lack oncogenic activating tyrosine kinase mutations in both KIT and PDGFRA.[41] Pediatric GISTs are treated differently from adult GISTs. Although the generally accepted definition of pediatric GIST is a tumor that is diagnosed at the age of 18 years or younger,[40] "pediatric-type" GISTs can be seen in adults, which affects risk assessment, the role of lymph node resection, and choice of therapy.[42]
1 2 3 4 5 6 7 8 9 10 11 12 13 Demetri, G. (2011). "Gastrointestinal Stromal Tumor". In DeVita, L; Lawrence, TS; Rosenberg, SA (eds.). DeVita, Hellman, and Rosenberg's Cancer: Principles and Practice of Oncology (9thed.). Wolters Kluwer Health/Lippincott Williams & Wilkins. ISBN978-1-4511-0545-2.
1 2 3 Miettinen M, Lasota J (2006). "Gastrointestinal stromal tumors: review on morphology, molecular pathology, prognosis, and differential diagnosis". Arch Pathol Lab Med. 130 (10): 1466–78. doi:10.5858/2006-130-1466-GSTROM. PMID17090188.
1 2 3 4 Burkill GJ, Badran M, Al-Muderis O, Meirion Thomas J, Judson IR, Fisher C, Moskovic EC (2003). "Malignant gastrointestinal stromal tumor: distribution, imaging features, and pattern of metastatic spread". Radiology. 226 (2): 527–32. doi:10.1148/radiol.2262011880. PMID12563150.
↑ Nishida T, Hirota S (2000). "Biological and clinical review of stromal tumors in the gastrointestinal tract". Histol Histopathol. 15 (4): 1293–301. PMID11005253.
↑ Raut, Chandrajit; Dematteo, Ronald (March 2008). "Evidence-Guided Surgical Management of GIST: Beyond a Simple Case of Benign and Malignant". Ann. Surg. Oncol. 15 (5): 1542–1543. doi:10.1245/s10434-008-9817-1. S2CID12586147.
1 2 3 4 Pidhorecky I, Cheney RT, Kraybill WG, Gibbs JF (2000). "Gastrointestinal stromal tumors: current diagnosis, biologic behavior, and management". Ann Surg Oncol. 7 (9): 705–12. doi:10.1007/s10434-000-0705-6. PMID11034250. S2CID663887.
1 2 Shojaku H, Futatsuya R, Seto H, etal. (1997). "Malignant gastrointestinal stromal tumor of the small intestine: radiologic-pathologic correlation". Radiat Med. 15 (3): 189–92. PMID9278378.
1 2 3 4 NCCN Clinical Practice Guidelines in Oncology Soft Tissue Sarcomas, version 3.2012. National Comprehensive Cancer Network.
↑ Carlson JW, Fletcher CD (2007). "Immunohistochemistry for beta-catenin in the differential diagnosis of spindle cell lesions: analysis of a series and review of the literature". Histopathology. 51 (4): 509–14. doi:10.1111/j.1365-2559.2007.02794.x. PMID17711447.
↑ Lehnert T (1998). "Gastrointestinal sarcoma (GIST)--a review of surgical management". Ann Chir Gynaecol. 87 (4): 297–305. PMID9891770.
↑ Levine MS, Buck JL, Pantongrag-Brown L, etal. (1996). "Leiomyosarcoma of the esophagus: radiographic findings in 10 patients". AJR Am J Roentgenol. 167 (1): 27–32. doi:10.2214/ajr.167.1.8659399. PMID8659399.
↑ Tervahartiala P, Halavaara J (1998). "Radiology of GIST. Gastrointestinal stromal tumours". Ann Chir Gynaecol. 87 (4): 291–2. PMID9891768.
↑ Lee, Chung-Ho; Hyun, Myung-Han; Kwon, Ye-Ji; Cho, Sung-Il; Park, Sung-Soo (2012). "Deciding Laparoscopic Approaches for Wedge Resection in Gastric Submucosal Tumors: A Suggestive Flow Chart Using Three Major Determinants". Journal of the American College of Surgeons. 215 (6): 831–840. doi:10.1016/j.jamcollsurg.2012.07.009. PMID22951033.
1 2 3 Kantarjian, HM; Wolff, RA; Koller, CA. (2011). The MD Anderson Manual of Medical Oncology (2nded.). McGraw-Hill. ISBN978-0-07-170106-8.
↑ Patel Shreyaskumar R; Wong Patrick (2009). "The Efficacy of Imatinib in Unresectable/Metastatic Gastrointestinal Stromal Tumors". US Oncology. 5 (1): 61–4. doi:10.17925/ohr.2009.05.1.61. S2CID78453531.
A tyrosine kinase is an enzyme that can transfer a phosphate group from ATP to the tyrosine residues of specific proteins inside a cell. It functions as an "on" or "off" switch in many cellular functions.
A sarcoma is a malignant tumor, a type of cancer that arises from cells of mesenchymal origin. Connective tissue is a broad term that includes bone, cartilage, fat, vascular, or other structural tissues, and sarcomas can arise in any of these types of tissues. As a result, there are many subtypes of sarcoma, which are classified based on the specific tissue and type of cell from which the tumor originates.
Imatinib, sold under the brand names Gleevec and Glivec (both marketed worldwide by Novartis) among others, is an oral targeted therapy medication used to treat cancer. Imatinib is a small molecule inhibitor targeting multiple tyrosine kinases such as CSF1R, ABL, c-KIT, FLT3, and PDGFR-β. Specifically, it is used for chronic myelogenous leukemia (CML) and acute lymphocytic leukemia (ALL) that are Philadelphia chromosome–positive (Ph+), certain types of gastrointestinal stromal tumors (GIST), hypereosinophilic syndrome (HES), chronic eosinophilic leukemia (CEL), systemic mastocytosis, and myelodysplastic syndrome.
Immunohistochemistry (IHC) is a form of immunostaining. It involves the process of selectively identifying antigens (proteins) in cells and tissue, by exploiting the principle of antibodies binding specifically to antigens in biological tissues. Albert Hewett Coons, Ernest Berliner, Norman Jones and Hugh J Creech was the first to develop immunofluorescence in 1941. This led to the later development of immunohistochemistry.
Dermatofibrosarcoma protuberans (DFSP) is a rare locally aggressive malignant cutaneous soft-tissue sarcoma. DFSP develops in the connective tissue cells in the middle layer of the skin (dermis). Estimates of the overall occurrence of DFSP in the United States are 0.8 to 4.5 cases per million persons per year. In the United States, DFSP accounts for between 1 and 6 percent of all soft-tissue sarcomas and 18 percent of all cutaneous soft-tissue sarcomas. In the Surveillance, Epidemiology and End Results (SEER) tumor registry from 1992 through 2004, DFSP was second only to Kaposi sarcoma.
Phyllodes tumors, are a rare type of biphasic fibroepithelial mass that form from the periductal stromal and epithelial cells of the breast. They account for less than 1% of all breast neoplasms. They were previously termed cystosarcoma phyllodes, coined by Johannes Müller in 1838, before being renamed to phyllodes tumor by the World Health Organization in 2003. Phullon, which means 'leaf' in Greek, describes the unique papillary projections characteristic of phyllodes tumors on histology. Diagnosis is made via a core-needle biopsy and treatment is typically surgical resection with wide margins (>1 cm), due to their propensity to recur.
Sunitinib, sold under the brand name Sutent, is an anti-cancer medication. It is a small-molecule, multi-targeted receptor tyrosine kinase (RTK) inhibitor that was approved by the FDA for the treatment of renal cell carcinoma (RCC) and imatinib-resistant gastrointestinal stromal tumor (GIST) in January 2006. Sunitinib was the first cancer drug simultaneously approved for two different indications.
Proto-oncogene c-KIT is the gene encoding the receptor tyrosine kinase protein known as tyrosine-protein kinase KIT, CD117 or mast/stem cell growth factor receptor (SCFR). Multiple transcript variants encoding different isoforms have been found for this gene. KIT was first described by the German biochemist Axel Ullrich in 1987 as the cellular homolog of the feline sarcoma viral oncogene v-kit.
Fibroblast growth factor receptor 1 (FGFR1), also known as basic fibroblast growth factor receptor 1, fms-related tyrosine kinase-2 / Pfeiffer syndrome, and CD331, is a receptor tyrosine kinase whose ligands are specific members of the fibroblast growth factor family. FGFR1 has been shown to be associated with Pfeiffer syndrome, and clonal eosinophilias.
Epithelioid sarcoma is a rare soft tissue sarcoma arising from mesenchymal tissue and characterized by epithelioid-like features. It accounts for less than 1% of all soft tissue sarcomas. It was first definitively characterized by F.M. Enzinger in 1970. It commonly presents itself in the distal limbs of young adults as a small, soft mass or a cluster of bumps. A proximal version has also been described, frequently occurring in the upper extremities. Less commonly, cases are reported in the pelvis, vulva, penis, and spine.
Platelet-derived growth factor receptor A, also termed CD140a, is a receptor located on the surface of a wide range of cell types. The protein is encoded in the human by the PDGFRA gene. This receptor binds to certain isoforms of platelet-derived growth factors (PDGFs) and thereby becomes active in stimulating cell signaling pathways that elicit responses such as cellular growth and differentiation. The receptor is critical for the embryonic development of certain tissues and organs, and for their maintenance, particularly hematologic tissues, throughout life. Mutations in PDGFRA, are associated with an array of clinically significant neoplasms, notably ones of the clonal hypereosinophilia class of malignancies, as well as gastrointestinal stromal tumors (GISTs).
Infantile myofibromatosis (IMF) is a rare tumor found in 1 in 150,000 to 1 in 400,000 live births. It is nonetheless the most common tumor derived from fibrous connective tissue that occurs primarily in infants and young children. IMF tumors are benign in the sense that they do not metastasize to distant tissues although when occurring in the viscera, i.e. internal organs, carry guarded to poor prognoses and can be life-threatening, particularly in newborns and young infants. The condition was first described by Arthur Purdy Stout as congenital generalized fibromatosis – in which he coined the word fibromatosis – in 1954.
Carney triad (CT) is characterized by the coexistence of three types of neoplasms, mainly in young women, including gastric gastrointestinal stromal tumor, pulmonary chondroma, and extra-adrenal paraganglioma. The underlying genetic defect remains elusive. CT is distinct from Carney complex, and the Carney-Stratakis syndrome.
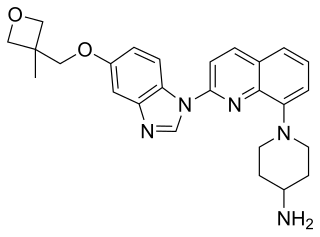
Crenolanib besylate is an investigational inhibitor being developed by AROG Pharmaceuticals, LLC. The compound is currently being evaluated for safety and efficacy in clinical trials for various types of cancer, including acute myeloid leukemia (AML), gastrointestinal stromal tumor (GIST), and glioma. Crenolanib is an orally bioavailable benzimidazole that selectively and potently inhibits signaling of wild-type and mutant isoforms of class III receptor tyrosine kinases (RTK) FLT3, PDGFR α, and PDGFR β. Unlike most RTK inhibitors, crenolanib is a type I mutant-specific inhibitor that preferentially binds to phosphorylated active kinases with the ‘DFG in’ conformation motif.
A cancer biomarker refers to a substance or process that is indicative of the presence of cancer in the body. A biomarker may be a molecule secreted by a tumor or a specific response of the body to the presence of cancer. Genetic, epigenetic, proteomic, glycomic, and imaging biomarkers can be used for cancer diagnosis, prognosis, and epidemiology. Ideally, such biomarkers can be assayed in non-invasively collected biofluids like blood or serum.
Clonal hypereosinophilia, also termed primary hypereosinophilia or clonal eosinophilia, is a grouping of hematological disorders all of which are characterized by the development and growth of a pre-malignant or malignant population of eosinophils, a type of white blood cell that occupies the bone marrow, blood, and other tissues. This population consists of a clone of eosinophils, i.e. a group of genetically identical eosinophils derived from a sufficiently mutated ancestor cell.
Gastroblastoma is a rare cancer that occurs in the stomach. Only six cases have been reported to date (2017).
Plexiform angiomyxoid myofibroblastic tumor (PAMT), also called plexiform angiomyxoma, plexiform angiomyxoid tumor, or myxofibroma, is an extremely rare benign mesenchymal myxoid tumor along the gastrointestinal tract. Most of PAMTs occur in the gastric antral region, but they can be situated anywhere in the stomach. There is one recorded case of PAMT located in duodenum.
Avapritinib, sold under the brand name Ayvakit among others, is a medication used for the treatment of advanced systemic mastocytosis and for the treatment of tumors due to one specific rare mutation: it is specifically intended for adults with unresectable or metastatic gastrointestinal stromal tumor (GIST) that harbor a platelet-derived growth factor receptor alpha (PDGFRA) exon 18 mutation. Avapritinib is a kinase inhibitor.
Ripretinib, sold under the brand name Qinlock, is a medication for the treatment of adults with advanced gastrointestinal stromal tumor (GIST), a type of tumor that originates in the gastrointestinal tract. It is taken by mouth. Ripretinib inhibits the activity of the kinases KIT and PDGFRA, which helps keep cancer cells from growing.
This page is based on this Wikipedia article Text is available under the CC BY-SA 4.0 license; additional terms may apply. Images, videos and audio are available under their respective licenses.