Related Research Articles

Interstitial cystitis (IC), a type of bladder pain syndrome (BPS), is chronic pain in the bladder and pelvic floor of unknown cause. It is the urologic chronic pelvic pain syndrome of women. Symptoms include feeling the need to urinate right away, needing to urinate often, and pain with sex. IC/BPS is associated with depression and lower quality of life. Many of those affected also have irritable bowel syndrome and fibromyalgia.
Vulvodynia is a chronic pain condition that affects the vulvar area and occurs without an identifiable cause. Symptoms typically include a feeling of burning or irritation. It has been established by the ISSVD that for the diagnosis to be made symptoms must last at least three months.
Urinary incontinence (UI), also known as involuntary urination, is any uncontrolled leakage of urine. It is a common and distressing problem, which may have a large impact on quality of life. It has been identified as an important issue in geriatric health care. The term enuresis is often used to refer to urinary incontinence primarily in children, such as nocturnal enuresis. UI is an example of a stigmatized medical condition, which creates barriers to successful management and makes the problem worse. People may be too embarrassed to seek medical help, and attempt to self-manage the symptom in secrecy from others.

The levator ani is a broad, thin muscle group, situated on either side of the pelvis. It is formed from three muscle components: the pubococcygeus, the iliococcygeus, and the puborectalis.

Vaginismus is a condition in which involuntary muscle spasm interferes with vaginal intercourse or other penetration of the vagina. This often results in pain with attempts at sex. Often it begins when vaginal intercourse is first attempted. Vaginismus may be considered an older term for pelvic floor dysfunction.
Dyspareunia is painful sexual intercourse due to medical or psychological causes. The term dyspareunia covers both female dyspareunia and male dyspareunia, but many discussions that use the term without further specification concern the female type, which is more common than the male type. In females, the pain can primarily be on the external surface of the genitalia, or deeper in the pelvis upon deep pressure against the cervix. Medically, dyspareunia is a pelvic floor dysfunction and is frequently underdiagnosed. It can affect a small portion of the vulva or vagina or be felt all over the surface. Understanding the duration, location, and nature of the pain is important in identifying the causes of the pain.

Kegel exercise, also known as pelvic floor exercise, involves repeatedly contracting and relaxing the muscles that form part of the pelvic floor, now sometimes colloquially referred to as the "Kegel muscles". The exercise can be performed many times a day, for several minutes at a time but takes one to three months to begin to have an effect.
Sexual dysfunction is difficulty experienced by an individual or partners during any stage of normal sexual activity, including physical pleasure, desire, preference, arousal, or orgasm. The World Health Organization defines sexual dysfunction as a "person's inability to participate in a sexual relationship as they would wish". This definition is broad and is subject to many interpretations. A diagnosis of sexual dysfunction under the DSM-5 requires a person to feel extreme distress and interpersonal strain for a minimum of six months. Sexual dysfunction can have a profound impact on an individual's perceived quality of sexual life. The term sexual disorder may not only refer to physical sexual dysfunction, but to paraphilias as well; this is sometimes termed disorder of sexual preference.

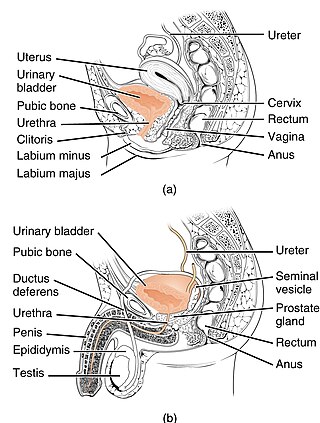
The pelvic floor or pelvic diaphragm is an anatomical location in the human body, which has an important role in urinary and anal continence, sexual function and support of the pelvic organs. The pelvic floor includes muscles, both skeletal and smooth, ligaments and fascia. and separates between the pelvic cavity from above, and the perineum from below. It is formed by the levator ani muscle and coccygeus muscle, and associated connective tissue.

Pelvic floor dysfunction is a term used for a variety of disorders that occur when pelvic floor muscles and ligaments are impaired. The condition affects up to 50 percent of women who have given birth. Although this condition predominantly affects women, up to 16 percent of men are affected as well. Symptoms can include pelvic pain, pressure, pain during sex, urinary incontinence (UI), overactive bladder, bowel incontinence, incomplete emptying of feces, constipation, myofascial pelvic pain and pelvic organ prolapse. When pelvic organ prolapse occurs, there may be visible organ protrusion or a lump felt in the vagina or anus. Research carried out in the UK has shown that symptoms can restrict everyday life for women. However, many people found it difficult to talk about it and to seek care, as they experienced embarrassment and stigma.
Sexual medicine or psychosexual medicine as defined by Masters and Johnsons in their classic Textbook of Sexual Medicine, is "that branch of medicine that focuses on the evaluation and treatment of sexual disorders, which have a high prevalence rate." Examples of disorders treated with sexual medicine are erectile dysfunction, hypogonadism, and prostate cancer. Sexual medicine often uses a multidisciplinary approach involving physicians, mental health professionals, social workers, and sex therapists. Sexual medicine physicians often approach treatment with medicine and surgery, while sex therapists often focus on behavioral treatments.

The cystocele, also known as a prolapsed bladder, is a medical condition in which a woman's bladder bulges into her vagina. Some may have no symptoms. Others may have trouble starting urination, urinary incontinence, or frequent urination. Complications may include recurrent urinary tract infections and urinary retention. Cystocele and a prolapsed urethra often occur together and is called a cystourethrocele. Cystocele can negatively affect quality of life.
Stress incontinence, also known as stress urinary incontinence (SUI) or effort incontinence is a form of urinary incontinence. It is due to inadequate closure of the bladder outlet by the urethral sphincter.
Vulvar vestibulitis syndrome (VVS), vestibulodynia, or simply vulvar vestibulitis, is vulvodynia localized to the vulvar vestibule. It tends to be associated with a highly localized "burning" or "cutting" type of pain. Until recently, "vulvar vestibulitis" was the term used for localized vulvar pain: the suffix "-itis" would normally imply inflammation, but in fact there is little evidence to support an inflammatory process in the condition. "Vestibulodynia" is the term now recognized by the International Society for the Study of Vulvovaginal Disease.
Sacral nerve stimulation, also termed sacral neuromodulation, is a type of medical electrical stimulation therapy.
Chronic prostatitis/chronic pelvic pain syndrome (CP/CPPS), previously known as chronic nonbacterial prostatitis, is long-term pelvic pain and lower urinary tract symptoms (LUTS) without evidence of a bacterial infection. It affects about 2–6% of men. Together with IC/BPS, it makes up urologic chronic pelvic pain syndrome (UCPPS).
Urogynecology or urogynaecology is a surgical sub-specialty of urology and gynecology.
National Association for Continence (NAFC) is a national, private, non-profit organization dedicated to improving the quality of life of people with incontinence, voiding dysfunction, and related pelvic floor disorders.
Urethral hypermobility is a condition of excessive movement of the female urethra due to a weakened urogenital diaphragm. It describes the instability of the urethra in relation to the pelvic floor muscles. A weakened pelvic floor muscle fails to adequately close the urethra and hence can cause stress urinary incontinence. This condition may be diagnosed by primary care providers or urologists. Treatment may include pelvic floor muscle exercises, surgery, or minimally invasive procedures.
References
- 1 2 3 Wallace, Shannon L.; Miller, Lucia D.; Mishra, Kavita (December 2019). "Pelvic floor physical therapy in the treatment of pelvic floor dysfunction in women". Current Opinion in Obstetrics & Gynecology. 31 (6): 485–493. doi:10.1097/GCO.0000000000000584. ISSN 1040-872X. PMID 31609735. S2CID 204703488.
- 1 2 Bradley, Michelle H.; Rawlins, Ashley; Brinker, C. Anna (August 2017). "Physical Therapy Treatment of Pelvic Pain". Physical Medicine and Rehabilitation Clinics of North America. 28 (3): 589–601. doi:10.1016/j.pmr.2017.03.009. PMID 28676366.
- ↑ Ghaderi, Fariba; Bastani, Parvin; Hajebrahimi, Sakineh; Jafarabadi, Mohammad Asghari; Berghmans, Bary (November 2019). "Pelvic floor rehabilitation in the treatment of women with dyspareunia: a randomized controlled clinical trial". International Urogynecology Journal. 30 (11): 1849–1855. doi:10.1007/s00192-019-04019-3. ISSN 0937-3462. PMC 6834927 . PMID 31286158.
- 1 2 Rosenbaum, Talli Yehuda (January 2007). "Reviews: Pelvic Floor Involvement in Male and Female Sexual Dysfunction and the Role of Pelvic Floor Rehabilitation in Treatment: A Literature Review". The Journal of Sexual Medicine. 4 (1): 4–13. doi:10.1111/j.1743-6109.2006.00393.x. PMID 17233772.
- ↑ Wente, Karla; Dolan, Christina (March 2018). "Aging and the Pelvic Floor". Current Geriatrics Reports. 7 (1): 49–58. doi:10.1007/s13670-018-0238-0. ISSN 2196-7865.
- ↑ Physiomobility (2017-05-26). "Urinary incontinence and the role of pelvic health physiotherapist". Physiomobility. Retrieved 2021-04-26.
- ↑ Sigurdardottir, Thorgerdur; Steingrimsdottir, Thora; Geirsson, Reynir T.; Halldorsson, Thorhallur I.; Aspelund, Thor; Bø, Kari (March 2020). "Can postpartum pelvic floor muscle training reduce urinary and anal incontinence?: An assessor-blinded randomized controlled trial". American Journal of Obstetrics and Gynecology. 222 (3): 247.e1–247.e8. doi: 10.1016/j.ajog.2019.09.011 . ISSN 1097-6868. PMID 31526791. S2CID 202674386.
- ↑ García-Sánchez, Esther; Ávila-Gandía, Vicente; López-Román, Javier; Martínez-Rodríguez, Alejandro; Rubio-Arias, Jacobo Á (2019-11-08). "What Pelvic Floor Muscle Training Load is Optimal in Minimizing Urine Loss in Women with Stress Urinary Incontinence? A Systematic Review and Meta-Analysis". International Journal of Environmental Research and Public Health. 16 (22): E4358. doi: 10.3390/ijerph16224358 . ISSN 1660-4601. PMC 6887794 . PMID 31717291.
- ↑ Zhu, Hongmei; Zhang, Di; Gao, Lei; Liu, Huixin; Di, Yonghui; Xie, Bing; Jiao, Wei; Sun, Xiuli (January 2022). "Effect of Pelvic Floor Workout on Pelvic Floor Muscle Function Recovery of Postpartum Women: Protocol for a Randomized Controlled Trial". International Journal of Environmental Research and Public Health. 19 (17): 11073. doi: 10.3390/ijerph191711073 . ISSN 1660-4601. PMC 9517758 . PMID 36078788.
- 1 2 3 Woodley, Stephanie J.; Boyle, Rhianon; Cody, June D.; Mørkved, Siv; Hay-Smith, E. Jean C. (2017-12-22). "Pelvic floor muscle training for prevention and treatment of urinary and faecal incontinence in antenatal and postnatal women". The Cochrane Database of Systematic Reviews. 12 (12): CD007471. doi:10.1002/14651858.CD007471.pub3. ISSN 1469-493X. PMC 6486304 . PMID 29271473.
- 1 2 Kuravska, Yuliia; Aravitska, Mariia; Churpiy, Ihor; Fedorivska, Lesia; Yaniv, Olesia (March 2022). "Efficacy of correction of pelvic floor muscle dysfunction using physical therapy in women who underwent Caesarean section". Journal of Physical Education and Sport. 22 (3): 715–723. doi: 10.7752/jpes.2022.03090 . ProQuest 2648269295.
- ↑ "What is pelvic floor therapy and do I need it?". Worth It PT: Pelvic Health & Physical Therapy. 9 August 2022.