Related Research Articles
A hernia is the abnormal exit of tissue or an organ, such as the bowel, through the wall of the cavity in which it normally resides. The term is also used for the normal development of the intestinal tract, referring to the retraction of the intestine from the extra-embryonal navel coelom into the abdomen in the healthy embryo at about 7½ weeks. Various types of hernias can occur, most commonly involving the abdomen, and specifically the groin. Groin hernias are most commonly inguinal hernias but may also be femoral hernias. Other types of hernias include hiatus, incisional, and umbilical hernias. Symptoms are present in about 66% of people with groin hernias. This may include pain or discomfort in the lower abdomen, especially with coughing, exercise, or urinating or defecating. Often, it gets worse throughout the day and improves when lying down. A bulge may appear at the site of hernia, that becomes larger when bending down. Groin hernias occur more often on the right than left side. The main concern is bowel strangulation, where the blood supply to part of the bowel is blocked. This usually produces severe pain and tenderness in the area. Hiatus, or hiatal hernias often result in heartburn but may also cause chest pain or pain while eating.
An inguinal hernia or groin hernia, is a hernia (protrusion) of abdominal cavity contents through the inguinal canal. Symptoms, which may include pain or discomfort especially with or following coughing, exercise, or bowel movements, are absent in about a third of patients. Symptoms often get worse throughout the day and improve when lying down. A bulging area may occur that becomes larger when bearing down. Inguinal hernias occur more often on the right than left side. The main concern is strangulation, where the blood supply to part of the intestine is blocked. This usually produces severe pain and tenderness of the area.

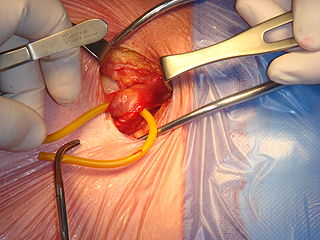
Hernia repair is a surgical operation for the correction of a hernia—a bulging of internal organs or tissues through the wall that contains it. It can be of two different types: herniorrhaphy; or hernioplasty. This operation may be performed to correct hernias of the abdomen, groin, diaphragm, brain, or at the site of a previous operation. Hernia repair is often performed as an ambulatory procedure.

Nerve block or regional nerve blockade is any deliberate interruption of signals traveling along a nerve, often for the purpose of pain relief. Local anesthetic nerve block is a short-term block, usually lasting hours or days, involving the injection of an anesthetic, a corticosteroid, and other agents onto or near a nerve. Neurolytic block, the deliberate temporary degeneration of nerve fibers through the application of chemicals, heat, or freezing, produces a block that may persist for weeks, months, or indefinitely. Neurectomy, the cutting through or removal of a nerve or a section of a nerve, usually produces a permanent block. Because neurectomy of a sensory nerve is often followed, months later, by the emergence of new, more intense pain, sensory nerve neurectomy is rarely performed.
Meralgia paresthetica or meralgia paraesthetica is numbness or pain in the outer thigh not caused by injury to the thigh, but by injury to a nerve that extends from the spinal column to the thigh.

An umbilical hernia is a health condition where the abdominal wall behind the navel is damaged. It may cause the navel to bulge outwards—the bulge consisting of abdominal fat from the greater omentum or occasionally parts of the small intestine. The bulge can often be pressed back through the hole in the abdominal wall, and may "pop out" when coughing or otherwise acting to increase intra-abdominal pressure. Treatment is surgical, and surgery may be performed for cosmetic as well as health-related reasons.
Athletic pubalgia, also called sports hernia, core injury, hockey hernia, hockey groin, Gilmore's groin, or groin disruption, is a medical condition of the pubic joint affecting athletes.

A Spigelian is the type of ventral hernia where aponeurotic fascia pushes through a hole in the junction of the linea semilunaris and the arcuate line creating a bulge. It appears in the abdomen lower quadrant between an area of dense fibrous tissue and abdominal wall muscles causing a.
Femoral hernias occur just below the inguinal ligament, when abdominal contents pass through a naturally occurring weakness in the abdominal wall called the femoral canal. Femoral hernias are a relatively uncommon type, accounting for only 3% of all hernias. While femoral hernias can occur in both males and females, almost all develop in women due to the increased width of the female pelvis. Femoral hernias are more common in adults than in children. Those that do occur in children are more likely to be associated with a connective tissue disorder or with conditions that increase intra-abdominal pressure. Seventy percent of pediatric cases of femoral hernias occur in infants under the age of one.
An incisional hernia is a type of hernia caused by an incompletely-healed surgical wound. Since median incisions in the abdomen are frequent for abdominal exploratory surgery, ventral incisional hernias are often also classified as ventral hernias due to their location. Not all ventral hernias are from incisions, as some may be caused by other trauma or congenital problems.
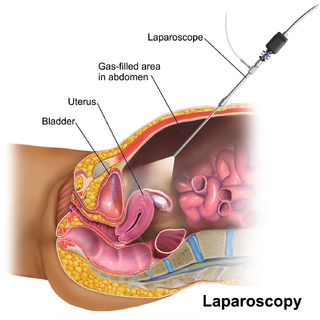
Laparoscopic hernia repair is the repair of a hiatal hernia using a laparoscope, which is a tiny telescope-like instrument. A hiatal hernia is the protrusion of an organ through its wall or cavity. There are several different methods that can be used when performing this procedure. Among them are the Nissen Fundoplication and the general laparoscopic hernia repair.
A neurectomy, or nerve resection is a neurosurgical procedure in which a peripheral nerve is cut or removed to alleviate neuropathic pain or permanently disable some function of a nerve. The nerve is not intended to grow back. For chronic pain it may be an alternative to a failed nerve decompression when the target nerve has no motor function and numbness is acceptable. Neurectomies have also been used to permanently block autonomic function, and special sensory function not related to pain.
Amyand's hernia is a rare form of an inguinal hernia which occurs when the appendix is included in the hernial sac and becomes incarcerated. The condition is an eponymous disease named after a French surgeon, Claudius Amyand (1660–1740), who performed the first successful appendectomy in 1735.
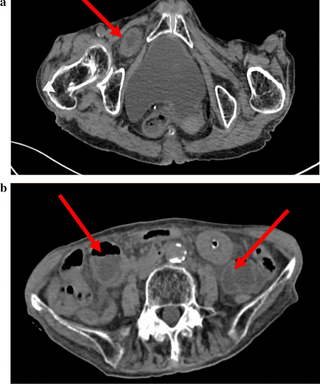
An obturator hernia is a rare type of hernia, encompassing 0.07-1% of all hernias, of the pelvic floor in which pelvic or abdominal contents protrudes through the obturator foramen. The obturator foramen is formed by a branch of the ischial as well as the pubic bone. The canal is typically 2-3 centimeters long and 1 centimeters wide, creating a space for pouches of pre-peritoneal fat.
In medicine, Carnett's sign is a finding on clinical examination in which (acute) abdominal pain remains unchanged or increases when the muscles of the abdominal wall are tensed. For this part of the abdominal examination, the patient can be asked to lift the head and shoulders from the examination table to tense the abdominal muscles. An alternative is to ask the patient to raise both legs with straight knees.
Round ligament pain (RLP) is pain associated with the round ligament of the uterus, usually during pregnancy. RLP is one of the most common discomforts of pregnancy and usually starts at the second trimester of gestation and continues until delivery. It usually resolves completely after delivery although cases of postpartum RLP have been reported. RLP also occurs in nonpregnant women.
Inguinal hernia surgery is an operation to repair a weakness in the abdominal wall that abnormally allows abdominal contents to slip into a narrow tube called the inguinal canal in the groin region.

Surgical mesh is a medical implant made of loosely woven mesh, which is used in surgery as either a permanent or temporary structural support for organs and other tissues. Surgical mesh can be made from both inorganic and biological materials and is used in a variety of surgeries, although hernia repair is the most common application. It can also be used for reconstructive work, such as in pelvic organ prolapse or to repair physical defects created by extensive resections or traumatic tissue loss.

The Triangle of Doom is an anatomical triangle defined by the vas deferens medially, spermatic vessels laterally and peritoneal fold inferiorly. This triangle contains external iliac artery and vein, the deep circumflex iliac vein, the genital branch of genitofemoral nerve and hidden by fascia, the femoral nerve. It bears significance in laparoscopic repair of groin hernia. Surgical staples are avoided here.
Anterior cutaneous nerve entrapment syndrome (ACNES) is a nerve entrapment condition that causes chronic pain of the abdominal wall. It occurs when nerve endings of the lower thoracic intercostal nerves (7–12) are 'entrapped' in abdominal muscles, causing a severe localized nerve (neuropathic) pain that is usually experienced at the front of the abdomen.
References
- ↑ Simons, M. P.; Aufenacker, T.; Bay-Nielsen, M.; Bouillot, J. L.; Campanelli, G.; Conze, J.; Lange, D.; Fortelny, R.; Heikkinen, T. (2009). "European Hernia Society guidelines on the treatment of inguinal hernia in adult patients". Hernia. 13 (4): 343–403. doi:10.1007/s10029-009-0529-7. PMC 2719730 . PMID 19636493.
- ↑ Rosenberg, Jacob; Bisgaard, Thue; Kehlet, Henrik; Wara, Pål; Asmussen, Torsten; Juul, Poul; Strand, Lasse; Andersen, Finn Heidemann; Bay-Nielsen, Morten (2011). "Danish Hernia Database recommendations for the management of inguinal and femoral hernia in adults" (PDF). Danish Medical Bulletin. 58 (2): C4243. PMID 21299930. Archived from the original (PDF) on 2015-01-03.
- 1 2 Alfieri, S.; Amid, P. K.; Campanelli, G.; Izard, G.; Kehlet, H.; Wijsmuller, A. R.; Di Miceli, D.; Doglietto, G. B. (2011). "International guidelines for prevention and management of post-operative chronic pain following inguinal hernia surgery". Hernia. 15 (3): 239–49. doi: 10.1007/s10029-011-0798-9 . PMID 21365287.
- 1 2 Alfieri, Sergio; Rotondi, Fabio; Di Miceli, Dario; Di Giorgio, Andrea; Ridolfini, Marco Pericoli; Fumagalli, Uberto; Salzano, Antonio; Prete, Francesco Paolo; Spadari, Antonio (2006). "Il dolore cronico dopo ernioplastica inguinale con protesi: il possibile ruolo della manipolazione chirurgica dei nervi del canale inguinale" [Chronic pain after inguinal hernia mesh repair: Possible role of surgical manipulation of the inguinal nerves. A prospective multicentre study of 973 cases](PDF). Chirurgia Italiana (in Italian). 58 (1): 23–31. PMID 16729606. Archived from the original (PDF) on 2018-12-01. Retrieved 2012-01-23.
- ↑ Ballert, Erik (2009). "Chronic Postoperative Inguinodynia: A pain in the *&%^". Archived from the original on 2012-02-29. Retrieved 2012-01-08.
- ↑ Picchio, Marcello; Palimento, Domenico; Attanasio, Ugo; Matarazzo, Pietro Filippo; Bambini, Chiara; Caliendo, Angelo (2004). "Randomized Controlled Trial of Preservation or Elective Division of Ilioinguinal Nerve on Open Inguinal Hernia Repair with Polypropylene Mesh". Archives of Surgery. 139 (7): 755–8, discussion 759. doi:10.1001/archsurg.139.7.755. PMID 15249409. S2CID 25278706.
- ↑ Al-dabbagh, A. K. R. (2002). "Anatomical variations of the inguinal nerves and risks of injury in 110 hernia repairs". Surgical and Radiologic Anatomy. 24 (2): 102–7. doi:10.1007/s00276-002-0006-9. PMID 12197017. S2CID 22788426.
- ↑ Ansaloni, Luca; Catena, Fausto; Coccolini, Federico; Gazzotti, Filippo; d'Alessandro, Luigi; Pinna, Antonio Daniele (2009). "Inguinal hernia repair with porcine small intestine submucosa: 3-year follow-up results of a randomized controlled trial of Lichtenstein's repair with polypropylene mesh versus Surgisis Inguinal Hernia Matrix". The American Journal of Surgery. 198 (3): 303–12. doi:10.1016/j.amjsurg.2008.09.021. PMID 19285658.
- ↑ Mohammadhosseini, Bijan (2010). "Risk Factors for Persistent Postherniorrhaphy Pain: Unresolved". Anesthesiology. 113 (5): 1243–4, author reply 1244. doi: 10.1097/ALN.0b013e3181f69604 . PMID 20966668.
- ↑ Shulman, AG; Amid, PK; Lichtenstein, IL (1993). "Ligation of hernial sac. A needless step in adult hernioplasty". International Surgery. 78 (2): 152–3. PMID 8354615.
- ↑ Delikoukos, S.; Lavant, L.; Hlias, G.; Palogos, K.; Gikas, D. (2007). "The role of hernia sac ligation in postoperative pain in patients with elective tension-free indirect inguinal hernia repair: A prospective randomized study". Hernia. 11 (5): 425–8. doi:10.1007/s10029-007-0249-9. PMID 17594052. S2CID 10958963.
- ↑ Ferzli, George S.; Edwards, Eric D.; Khoury, George E. (2007). "Chronic Pain after Inguinal Herniorrhaphy". Journal of the American College of Surgeons. 205 (2): 333–41. doi:10.1016/j.jamcollsurg.2007.02.081. PMID 17660082.
- ↑ Palumbo, P.; Minicucci, A.; Nasti, A. G.; Simonelli, I.; Vietri, F.; Angelici, A. M. (2007). "Treatment for persistent chronic neuralgia after inguinal hernioplasty". Hernia. 11 (6): 527–31. doi:10.1007/s10029-007-0268-6. PMID 17668147. S2CID 13018105.
- ↑ Delikoukos, S.; Fafoulakis, F.; Christodoulidis, G.; Theodoropoulos, T.; Hatzitheofilou, C. (2008). "Re-operation due to severe late-onset persisting groin pain following anterior inguinal hernia repair with mesh". Hernia. 12 (6): 593–5. doi:10.1007/s10029-008-0392-y. PMID 18542838. S2CID 19975450.
- ↑ Vuilleumier, Henri; Hübner, Martin; Demartines, Nicolas (2009). "Neuropathy After Herniorrhaphy: Indication for Surgical Treatment and Outcome" (PDF). World Journal of Surgery. 33 (4): 841–5. doi:10.1007/s00268-008-9869-1. PMID 19156462. S2CID 41720538.
- ↑ Aasvang, Eske K.; Kehlet, Henrik (2009). "The Effect of Mesh Removal and Selective Neurectomy on Persistent Postherniotomy Pain". Annals of Surgery. 249 (2): 327–34. doi:10.1097/SLA.0b013e31818eec49. PMID 19212190. S2CID 26342268.
- ↑ Amid, Parviz K.; Hiatt, Jonathan R. (2007). "New Understanding of the Causes and Surgical Treatment of Postherniorrhaphy Inguinodynia and Orchalgia". Journal of the American College of Surgeons. 205 (2): 381–5. doi:10.1016/j.jamcollsurg.2007.04.001. PMID 17660088.
- ↑ Amid, Parviz K.; Chen, David C. (2011). "Surgical Treatment of Chronic Groin and Testicular Pain after Laparoscopic and Open Preperitoneal Inguinal Hernia Repair". Journal of the American College of Surgeons. 213 (4): 531–6. doi:10.1016/j.jamcollsurg.2011.06.424. PMID 21784668.
- ↑ Callesen, T.; Bech, K.; Kehlet, H. (1999). "Prospective study of chronic pain after groin hernia repair". British Journal of Surgery. 86 (12): 1528–31. doi: 10.1046/j.1365-2168.1999.01320.x . PMID 10594500. S2CID 45862680.
- ↑ Courtney, C. A.; Duffy, K.; Serpell, M. G.; O'Dwyer, P. J. (2002). "Outcome of patients with severe chronic pain following repair of groin hernia". British Journal of Surgery. 89 (10): 1310–4. doi:10.1046/j.1365-2168.2002.02206.x. PMID 12296903. S2CID 23810958.
- ↑ Grant, A. M.; Scott, N. W.; O'Dwyer, P. J.; MRC Laparoscopic Groin Hernia Trial Group (2004). "Five-year follow-up of a randomized trial to assess pain and numbness after laparoscopic or open repair of groin hernia". British Journal of Surgery. 91 (12): 1570–4. doi: 10.1002/bjs.4799 . PMID 15515112. S2CID 25971273.
- ↑ Eklund, A.; Montgomery, A.; Bergkvist, L.; Rudberg, C.; Swedish Multicentre Trial of Inguinal Hernia Repair by Laparoscopy (SMIL) study group (2010). "Chronic pain 5 years after randomized comparison of laparoscopic and Lichtenstein inguinal hernia repair". British Journal of Surgery. 97 (4): 600–8. doi: 10.1002/bjs.6904 . PMID 20186889. S2CID 41990146.
- ↑ Wennström, I; Berggren, P; Åkerud, L; Järhult, J (2004). "Equal results with laparoscopic and Shouldice repairs of primary inguinal hernia in men. Report from a prospective randomised study" (PDF). Scandinavian Journal of Surgery. 93 (1): 34–6. doi:10.1177/145749690409300107. PMID 15116817. S2CID 25686860. Archived from the original (PDF) on 2013-10-02.