
Asthma is a long-term inflammatory disease of the airways of the lungs. It is characterized by variable and recurring symptoms, reversible airflow obstruction, and easily triggered bronchospasms. Symptoms include episodes of wheezing, coughing, chest tightness, and shortness of breath. These may occur a few times a day or a few times per week. Depending on the person, asthma symptoms may become worse at night or with exercise.

A cough is a sudden expulsion of air through the large breathing passages which can help clear them of fluids, irritants, foreign particles and microbes. As a protective reflex, coughing can be repetitive with the cough reflex following three phases: an inhalation, a forced exhalation against a closed glottis, and a violent release of air from the lungs following opening of the glottis, usually accompanied by a distinctive sound.
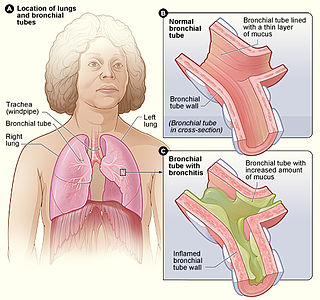
Acute bronchitis, also known as a chest cold, is short-term bronchitis – inflammation of the bronchi of the lungs. The most common symptom is a cough. Other symptoms include coughing up mucus, wheezing, shortness of breath, fever, and chest discomfort. The infection may last from a few to ten days. The cough may persist for several weeks afterward with the total duration of symptoms usually around three weeks. Some have symptoms for up to six weeks.

Bronchiectasis is a disease in which there is permanent enlargement of parts of the airways of the lung. Symptoms typically include a chronic cough with mucus production. Other symptoms include shortness of breath, coughing up blood, and chest pain. Wheezing and nail clubbing may also occur. Those with the disease often get lung infections.
A wheeze is a clinical symptom of a continuous, coarse, whistling sound produced in the respiratory airways during breathing. For wheezes to occur, some part of the respiratory tree must be narrowed or obstructed, or airflow velocity within the respiratory tree must be heightened. Wheezing is commonly experienced by persons with a lung disease; the most common cause of recurrent wheezing is asthma, though it can also be a symptom of lung cancer, congestive heart failure, and certain types of heart diseases.
Eosinophilic pneumonia is a disease in which an eosinophil, a type of white blood cell, accumulates in the lungs. These cells cause disruption of the normal air spaces (alveoli) where oxygen is extracted from the atmosphere. Several different kinds of eosinophilic pneumonia exist and can occur in any age group. The most common symptoms include cough, fever, difficulty breathing, and sweating at night. Eosinophilic pneumonia is diagnosed by a combination of characteristic symptoms, findings on a physical examination by a health provider, and the results of blood tests and X-rays. Prognosis is excellent once most eosinophilic pneumonia is recognized and treatment with corticosteroids is begun.
Acute severe asthma, also known as status asthmaticus, is an acute exacerbation of asthma that does not respond to standard treatments of bronchodilators (inhalers) and corticosteroids. Asthma is caused by multiple genes, some having protective effect, with each gene having its own tendency to be influenced by the environment although a genetic link leading to acute severe asthma is still unknown. Symptoms include chest tightness, rapidly progressive dyspnea, dry cough, use of accessory respiratory muscles, fast and/or labored breathing, and extreme wheezing. It is a life-threatening episode of airway obstruction and is considered a medical emergency. Complications include cardiac and/or respiratory arrest. The increasing prevalence of atopy and asthma remains unexplained but may be due to infection with respiratory viruses.
Exercise-induced asthma (E.I.A.) occurs when the airways narrow as a result of exercise. The preferred term for this condition is exercise-induced bronchoconstriction (EIB). While exercise does not cause asthma, it is frequently an asthma trigger.
Feline asthma is a common allergic respiratory disease in cats, affecting at least one percent of all adult cats worldwide. It is a chronic progressive disease for which there is no cure. Common symptoms include wheezing, coughing, labored breathing and potentially life-threatening bronchoconstriction. There is conjecture that the disease has become more common due to increased exposure to industrial pollutants. Feline asthma can also be attributed to lung damage caused by long-term exposure to second-hand smoke.
A habit cough is a chronic cough that has no underlying organic cause or medical diagnosis, and does not respond to conventional medical treatment. This is sometimes called tic cough,somatic cough syndrome and previously psychogenic cough, but without clinical justification.
The use of podiatry drills, in the absence of engineering controls and personal protective equipment, is an occupational hazard to the healthcare provider. Nail dust collected during foot care procedures performed in office settings has been found to contain keratin, keratin hydrolysates, microbial debris, and viable fungal elements, including dermatophytes and saprotrophs. Exposure to nail dust and the associated risk will vary with the policies and practices in place, the type of podiatry drill used, therapy technique, frequency of procedures, personal protective equipment utilized and the use of ventilation systems.
Occupational asthma is new onset asthma or the recurrence of previously quiescent asthma directly caused by exposure to an agent at workplace. It is an occupational lung disease and a type of work-related asthma. Agents that can induce occupational asthma can be grouped into sensitizers and irritants.

Obstructive lung disease is a category of respiratory disease characterized by airway obstruction. Many obstructive diseases of the lung result from narrowing (obstruction) of the smaller bronchi and larger bronchioles, often because of excessive contraction of the smooth muscle itself. It is generally characterized by inflamed and easily collapsible airways, obstruction to airflow, problems exhaling, and frequent medical clinic visits and hospitalizations. Types of obstructive lung disease include; asthma, bronchiectasis, bronchitis and chronic obstructive pulmonary disease (COPD). Although COPD shares similar characteristics with all other obstructive lung diseases, such as the signs of coughing and wheezing, they are distinct conditions in terms of disease onset, frequency of symptoms, and reversibility of airway obstruction. Cystic fibrosis is also sometimes included in obstructive pulmonary disease.
Vocal cord dysfunction (VCD) is a pathology affecting the vocal folds characterized by full or partial vocal fold closure causing difficulty and distress during respiration, especially during inhalation.

Eosinophilic bronchitis (EB) is a type of airway inflammation due to excessive mast cell recruitment and activation in the superficial airways as opposed to the smooth muscles of the airways as seen in asthma. It often results in a chronic cough. Lung function tests are usually normal. Inhaled corticosteroids are often an effective treatment.
Tropical pulmonary eosinophilia, is characterized by cough, bronchospasm, wheezing, abdominal pain, and an enlarged spleen. Occurring most frequently in the Indian subcontinent and Southeast Asia, TPE is a clinical manifestation of lymphatic filariasis, a parasitic infection caused by filarial roundworms that inhabit the lymphatic vessels, lymph nodes, spleen, and bloodstream. Three species of filarial roundworms, all from the Onchocercidae family, cause human lymphatic filariasis: Wuchereria bancrofti, Brugia malayi, and Brugia timori.
Stuart Merrill Brooks is an American pulmonary doctor who is credited for discovering and researching Reactive Airways Dysfunction Syndrome (RADS) to describe an asthma-like syndrome developing after a single exposure to high levels of an irritating vapor, fume, or smoke. It involves coughing, wheezing, and dyspnea. Dr Brooks received the highest honor in occupational and environmental medicine, the Knudsen Award. This award recognizes an individual who has made outstanding contributions to the field. Dr Brooks was honored for his exemplary efforts in starting the first occupational medicine residency in Florida in 1982.
Diffuse idiopathic pulmonary neuroendocrine cell hyperplasia (DIPNECH) is a diffuse parenchymal lung disease which often presents with symptoms of cough and shortness of breath. The pathological definition published by the World Health Organization is “a generalized proliferation of scattered single cells, small nodules, or linear proliferations of pulmonary neuroendocrine (PNE) cells that may be confined to the bronchial and bronchiolar epithelium.” The true prevalence of this disease is not known. To date, just under 200 cases have been reported in the literature. However, with an increase in recognition of this disease by radiologists and pulmonologists, the number of cases has been increasing. DIPNECH predominantly affects middle-aged women with slowly progressive lung obstruction. DIPNECH is usually discovered in one of two ways: 1) as an unexpected finding following a lung surgery; or 2) by evaluation of a patient in a pulmonary clinic with longstanding, unexplained symptoms.
Plastic bronchitis (PB) is a disorder in which branching casts of the airways are expectorated. PB is not a single disease with a defined mechanism that explains the cast formation in all conditions. Examples of diseases associated with expectoration of casts, and which sometimes are labeled PB include tuberculosis, atypical mycobacterial disease, allergic bronchopulmonary aspergillosis, and asthma.
Chronic cough is long-term coughing, sometimes defined as more than several weeks or months. Generally a cough lasting for more than eight weeks for an adult would meet the clinical definition of a chronic cough; and for children this threshold is lower. The term can be used to describe the different causes related to coughing, the three main ones being upper airway cough syndrome, asthma and gastroesophageal reflux disease. It occurs in the upper airway of the respiratory system. Generally, a cough lasts around one to two weeks; however, chronic cough can persist for an extended period of time defined as six weeks or longer. People with chronic cough often experience more than one cause present. Due to the nature of the syndrome, the treatments used are similar; however, there are a subsequent number of treatments available, and the clinical management of the patients remains a challenge.

