
Streptococcal pharyngitis, also known as streptococcal sore throat, is pharyngitis caused by Streptococcus pyogenes, a gram-positive, group A streptococcus. Common symptoms include fever, sore throat, red tonsils, and enlarged lymph nodes in the front of the neck. A headache and nausea or vomiting may also occur. Some develop a sandpaper-like rash which is known as scarlet fever. Symptoms typically begin one to three days after exposure and last seven to ten days.

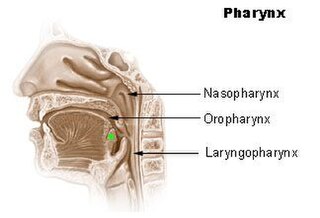
Pharyngitis is inflammation of the back of the throat, known as the pharynx. It typically results in a sore throat and fever. Other symptoms may include a runny nose, cough, headache, difficulty swallowing, swollen lymph nodes, and a hoarse voice. Symptoms usually last 3–5 days, but can be longer depending on cause. Complications can include sinusitis and acute otitis media. Pharyngitis is a type of upper respiratory tract infection.

Necrotizing gingivitis (NG) is a common, non-contagious infection of the gums with sudden onset. The main features are painful, bleeding gums, and ulceration of inter-dental papillae. This disease, along with necrotizing periodontitis (NP) and necrotizing stomatitis, is classified as a necrotizing periodontal disease, one of the three general types of gum disease caused by inflammation of the gums (periodontitis).
Sore throat, also known as throat pain, is pain or irritation of the throat. Usually, causes of sore throat include:

Palatine tonsils, commonly called the tonsils and occasionally called the faucial tonsils, are tonsils located on the left and right sides at the back of the throat, which can often be seen as flesh-colored, pinkish lumps. Tonsils only present as "white lumps" if they are inflamed or infected with symptoms of exudates and severe swelling.

Tonsillectomy is a surgical procedure in which both palatine tonsils are fully removed from the back of the throat. The procedure is mainly performed for recurrent tonsillitis, throat infections and obstructive sleep apnea (OSA). For those with frequent throat infections, surgery results in 0.6 fewer sore throats in the following year, but there is no evidence of long term benefits. In children with OSA, it results in improved quality of life.

Bad breath, also known as halitosis, is a symptom in which a noticeably unpleasant breath odour is present. It can result in anxiety among those affected. It is also associated with depression and symptoms of obsessive compulsive disorder.

Adenoidectomy is the surgical removal of the adenoid for reasons which include impaired breathing through the nose, chronic infections, or recurrent earaches. The effectiveness of removing the adenoids in children to improve recurrent nasal symptoms and/or nasal obstruction has not been well studied. The surgery is less commonly performed in adults in whom the adenoid is much smaller and less active than it is in children. It is most often done on an outpatient basis under general anesthesia. Post-operative pain is generally minimal and reduced by icy or cold foods. The procedure is often combined with tonsillectomy, for which the recovery time is an estimated 10–14 days, sometimes longer, mostly dependent on age.

An upper respiratory tract infection (URTI) is an illness caused by an acute infection, which involves the upper respiratory tract, including the nose, sinuses, pharynx, larynx or trachea. This commonly includes nasal obstruction, sore throat, tonsillitis, pharyngitis, laryngitis, sinusitis, otitis media, and the common cold. Most infections are viral in nature, and in other instances, the cause is bacterial. URTIs can also be fungal or helminthic in origin, but these are less common.
Tonsillitis is inflammation of the tonsils in the upper part of the throat. It can be acute or chronic. Acute tonsillitis typically has a rapid onset. Symptoms may include sore throat, fever, enlargement of the tonsils, trouble swallowing, and enlarged lymph nodes around the neck. Complications include peritonsillar abscess (Quinsy).

Herpangina, also called mouth blisters, is a painful mouth infection caused by coxsackieviruses. Usually, herpangina is produced by one particular strain of coxsackie virus A, but it can also be caused by coxsackievirus B or echoviruses. Most cases of herpangina occur in the summer, affecting mostly children. However, it occasionally occurs in adolescents and adults. It was first characterized in 1920.

Peritonsillar abscess (PTA), also known as quinsy, is an accumulation of pus due to an infection behind the tonsil. Symptoms include fever, throat pain, trouble opening the mouth, and a change to the voice. Pain is usually worse on one side. Complications may include blockage of the airway or aspiration pneumonitis.
Keratosis Pharyngis is a medical condition where keratin grows on the surface of the pharynx, that is the part of the throat at the back of the mouth. Keratin is a protein that normally occurs as the main component of hair and nails. It is characterized by the presence of whitish-yellow dots on the pharyngeal wall, tonsils or lingual tonsils. They are firmly adherent and cannot be wiped off. The surrounding region does not show any sign or inflammation or any other symptoms that make affect the rest of the body.

Sialolithiasis is a crystallopathy where a calcified mass or sialolith forms within a salivary gland, usually in the duct of the submandibular gland. Less commonly the parotid gland or rarely the sublingual gland or a minor salivary gland may develop salivary stones.

The tonsils are a set of lymphoid organs facing into the aerodigestive tract, which is known as Waldeyer's tonsillar ring and consists of the adenoid tonsil, two tubal tonsils, two palatine tonsils, and the lingual tonsils. These organs play an important role in the immune system.
Adenoiditis is the inflammation of the adenoid tissue usually caused by an infection. Adenoiditis is treated using medication or surgical intervention.

The human palatine tonsils (PT) are covered by stratified squamous epithelium that extends into deep and partly branched tonsillar crypts, of which there are about 10 to 30. The crypts greatly increase the contact surface between environmental influences and lymphoid tissue. In an average adult palatine tonsil the estimated epithelial surface area of the crypts is 295 cm2, in addition to the 45 cm2 of epithelium covering the oropharyngeal surface.

Trichomonas tenax, or oral trichomonas, is a species of Trichomonas commonly found in the oral cavity of humans. Routine hygiene is generally not sufficient to eliminate the parasite, hence its Latin name, meaning "tenacious". The parasite is frequently encountered in periodontal infections, affecting more than 50% of the population in some areas, but it is usually considered insignificant. T. tenax is generally not found on the gums of healthy patients. It is known to play a pathogenic role in necrotizing ulcerative gingivitis and necrotizing ulcerative periodontitis, worsening preexisting periodontal disease. This parasite is also implicated in some chronic lung diseases; in such cases, removal of the parasite is sufficient to allow recovery.
Carcinoma of the tonsil is a type of squamous cell carcinoma. The tonsil is the most common site of squamous cell carcinoma in the oropharynx. It comprises 23.1% of all malignancies of the oropharynx. The tumors frequently present at advanced stages, and around 70% of patients present with metastasis to the cervical lymph nodes. . The most reported complaints include sore throat, otalgia or dysphagia. Some patients may complain of feeling the presence of a lump in the throat. Approximately 20% patients present with a node in the neck as the only symptom.

Coblation tonsillectomy is a surgical procedure in which the patient's tonsils are removed by destroying the surrounding tissues that attach them to the pharynx. It was first implemented in 2001. The word coblation is short for ‘controlled ablation’, which means a controlled procedure used to destroy soft tissue.






