| Accessory auricle | |
|---|---|
 | |
| Specialty | Dermatology |
An accessory auricle is a congenital anomaly typically seen as a skin coloured nodule, most frequently just to the front of the ear. [1] [2]
| Accessory auricle | |
|---|---|
| | |
| Specialty | Dermatology |
An accessory auricle is a congenital anomaly typically seen as a skin coloured nodule, most frequently just to the front of the ear. [1] [2]

The general presentation is of a skin-covered nodule, papule, or nodule of the skin surface, usually immediately anterior to the auricle. [2] However, it may be anywhere within the periauricular tissues. [2] Bilateral presentation can be seen. [2]
A study of a family with 11 affected showed the accessory auricle were inherited in an autosomal dominant manner. [3]
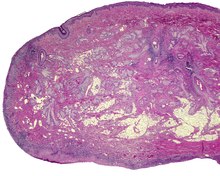
The lesions presents as a nodule or papule, either sessile or pedunculated. They may be soft or have a cartilaginous structure. By histologic examination, it is a recapitulation of normal external auricle. There will be skin, cartilaginous structures, and cartilage (although the last is not seen in all variants of this disorder). [4] [5] Some investigators believe that the tragus is the only hillock which is derived from the first branchial arch. This is clearly suggestive that true cases of accessory auricle represent a true duplication of the hillocks that were part of the second branchial arch. [6] The second ear appears as a mirror image folded forward and lying on the posterior cheek.[ citation needed ]
These structures are distinctly different from squamous papilloma and benign teratoma.[ citation needed ]
The several components or degrees of development range from an ear tag, preauricular appendage, preauricular tag, or accessory tragus, to supernumerary ears or polyotia. [7] It is a relatively common congenital anomaly of the first branchial arch or second branchial arches. Other anomalies may be present concurrently, including cleft palate, cleft lip, or mandibular hypoplasia. There is a known association with Goldenhar syndrome (oculo-auriculo-vertebral syndrome) [8] and with Wildervanck syndrome. [9] [10] [11] There may also be an association with congenital cartilaginous rest of the neck.[ citation needed ]
Simple surgical excision is curative. [12] The recommended treatment is that the skin is peeled off the extra-auricular tissue and protruding cartilage remnants are trimmed. [13] Normal appearance is achieved in majority of cases. The reconstruction successful in true cases of accessory auricle, as it also is in individuals with auricular appendages. [14] [15]
These lesions usually present in neonates, although they may not come to clinical attention until adulthood (for cosmetic reasons). There is no gender predilection. They are present in approximately 3–6 per 1000 live births. [16]

The outer ear, external ear, or auris externa is the external part of the ear, which consists of the auricle and the ear canal. It gathers sound energy and focuses it on the eardrum.

Anotia describes a rare congenital deformity that involves the complete absence of the auricle, the outer projected portion of the ear, and narrowing or absence of the ear canal. This contrasts with microtia, in which a small part of the auricle is present. Anotia and microtia may occur unilaterally or bilaterally. This deformity results in conductive hearing loss, deafness.

In vertebrates, an ear is the organ that enables hearing and body balance using the vestibular system. In humans, the ear is described as having three parts: the outer ear, the middle ear and the inner ear. The outer ear consists of the auricle and the ear canal. Since the outer ear is the only visible portion of the ear, the word "ear" often refers to the external part (auricle) alone. The middle ear includes the tympanic cavity and the three ossicles. The inner ear sits in the bony labyrinth, and contains structures which are key to several senses: the semicircular canals, which enable balance and eye tracking when moving; the utricle and saccule, which enable balance when stationary; and the cochlea, which enables hearing. The ear canal is cleaned via earwax, which naturally migrates to the auricle.

The auricle or auricula is the visible part of the ear that is outside the head. It is also called the pinna, a term that is used more in zoology.

Treacher Collins syndrome (TCS) is a genetic disorder characterized by deformities of the ears, eyes, cheekbones, and chin. The degree to which a person is affected, however, may vary from mild to severe. Complications may include breathing problems, problems seeing, cleft palate, and hearing loss. Those affected generally have normal intelligence.
Otoplasty is a procedure for correcting the deformities and defects of the auricle, whether these defects are congenital conditions or caused by trauma. Otoplastic surgeons may reshape, move, or augment the cartilaginous support framework of the auricle to correct these defects.

Microtia is a congenital deformity where the auricle is underdeveloped. A completely undeveloped auricle is referred to as anotia. Because microtia and anotia have the same origin, it can be referred to as microtia-anotia. Microtia can be unilateral or bilateral. Microtia occurs in 1 out of about 8,000–10,000 births. In unilateral microtia, the right ear is most commonly affected. It may occur as a complication of taking Accutane (isotretinoin) during pregnancy.
The tragus is a small pointed eminence of the external ear, situated in front of the concha, and projecting backward over the meatus. It also is the name of hair growing at the entrance of the ear. Its name comes from the Ancient Greek tragos, meaning 'goat', and is descriptive of its general covering on its under surface with a tuft of hair, resembling a goat's beard. The nearby antitragus projects forwards and upwards.

Goldenhar syndrome is a rare congenital defect characterized by incomplete development of the ear, nose, soft palate, lip and mandible on usually one side of the body. Common clinical manifestations include limbal dermoids, preauricular skin tags and strabismus. It is associated with anomalous development of the first branchial arch and second branchial arch.

Cutis marmorata telangiectatica congenita (CMTC) is a rare congenital vascular disorder that usually manifests in affecting the blood vessels of the skin. The condition was first recognized and described in 1922 by Cato van Lohuizen, a Dutch pediatrician whose name was later adopted in the other common name used to describe the condition – Van Lohuizen syndrome. CMTC is also used synonymously with congenital generalized phlebectasia, nevus vascularis reticularis, congenital phlebectasia, livedo telangiectatica, congenital livedo reticularis and Van Lohuizen syndrome.

A branchial cleft cyst or simply branchial cyst is a cyst as a swelling in the upper part of neck anterior to sternocleidomastoid. It can, but does not necessarily, have an opening to the skin surface, called a fistula. The cause is usually a developmental abnormality arising in the early prenatal period, typically failure of obliteration of the second, third, and fourth branchial cleft, i.e. failure of fusion of the second branchial arches and epicardial ridge in lower part of the neck. Branchial cleft cysts account for almost 20% of neck masses in children. Less commonly, the cysts can develop from the first, third, or fourth clefts, and their location and the location of associated fistulas differs accordingly.
Anetoderma is a benign but uncommon disorder that causes localized areas of flaccid or herniated sac-like skin due to a focal reduction of dermal elastic tissue. Anetoderma is subclassified as primary anetoderma, secondary anetoderma, iatrogenic anetoderma of prematurity, congenital anetoderma, familial anetoderma, and drug-induced anetoderma.

Aplasia cutis congenita is a rare disorder characterized by congenital absence of skin. Ilona J. Frieden classified ACC in 1986 into 9 groups on the basis of location of the lesions and associated congenital anomalies. The scalp is the most commonly involved area with lesser involvement of trunk and extremities. Frieden classified ACC with fetus papyraceus as type 5. This type presents as truncal ACC with symmetrical absence of skin in stellate or butterfly pattern with or without involvement of proximal limbs. It is the most common congenital cicatricial alopecia, and is a congenital focal absence of epidermis with or without evidence of other layers of the skin.

Preauricular sinuses and preauricular cysts are two common congenital malformations. Each involves the external ear. The difference between them is that a cyst does not connect with the skin, but a sinus does. Frequency of preauricular sinus differs depending the population: 0.1–0.9% in the US, 0.9% in the UK, and 4–10% in Asia and parts of Africa.
Pigmented hairy epidermal nevus syndrome, also known as Becker's naevus syndrome, is a cutaneous condition characterized by a Becker nevus, ipsilateral hypoplasia of the breast, and skeletal defects such as scoliosis.
Pseudocyst of the auricle, also known as auricular pseudocyst, endochondral pseudocyst, cystic chondromalacia, intracartilaginous auricular seroma cyst, and benign idiopathic cystic chondromalacia, is a cutaneous condition characterized by a fluctuant, tense, noninflammatory swelling on the upper half of the ear, known as the auricle or pinna. Pseudocysts of the auricle are nontender, noninflammatory cystic lesions that progress over a 4- to 12-week period, ranging from 1 to 5 cm in diameter. They are usually unilateral, often on the right ear, but can also present bilaterally.

Congenital cartilaginous rest of the neck (CCRN) is a minor and very rare congenital cutaneous condition characterized by branchial arch remnants that are considered to be the cervical variant of accessory tragus. It resembles a rudimentary pinna that in most cases is located in the lower anterior part of the neck.
Wildervanck syndrome or cervico-oculo-acoustic syndrome comprises a triad of:

Supernumerary nipples–uropathies–Becker's nevus syndrome is a skin condition that may be associated with genitourinary tract abnormalities. Supernumerary nipples, also referred to as polythelia or accessory nipples, is a pigmented lesion of the skin that is present at birth. This pigmentation usually occurs along the milk lines, which are the precursors to breast and nipple development. Clinically, this congenital condition is generally considered benign, but some studies have suggested there may be an association with kidney diseases and cancers of the urogenital system.
Midline cervical clefts are a rare congenital anomaly resulting from incomplete fusion during embryogenesis of the first and second branchial arches in the ventral midline of the neck. The condition presents as a midline cutaneous defect of the anterior neck with a skin projection or sinus, or as a subcutaneous erythematous fibrous cord. Surgical excision is the preferred treatment.