Related Research Articles
Post-traumatic stress disorder (PTSD) is a mental and behavioral disorder that can develop because of exposure to a traumatic event, such as sexual assault, warfare, traffic collisions, child abuse, domestic violence or other threats on a person's life. Symptoms may include disturbing thoughts, feelings, or dreams related to the events, mental or physical distress to trauma-related cues, attempts to avoid trauma-related cues, alterations in the way a person thinks and feels, and an increase in the fight-or-flight response. These symptoms last for more than a month after the event. Young children are less likely to show distress, but instead may express their memories through play. A person with PTSD is at a higher risk of suicide and intentional self-harm.
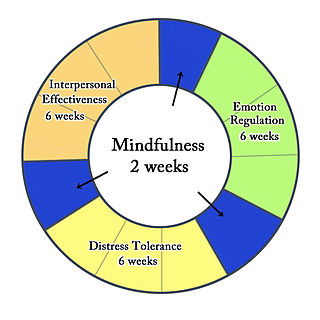
Dialectical behavior therapy (DBT) is an evidence-based psychotherapy that began with efforts to treat personality disorders, and interpersonal conflicts. There is evidence that DBT can be useful in treating mood disorders, suicidal ideation, and for change in behavioral patterns such as self-harm and substance use. DBT evolved into a process in which the therapist and client work with acceptance and change-oriented strategies, and ultimately balance and synthesize them, in a manner comparable to the philosophical dialectical process of hypothesis and antithesis, followed by synthesis.
Nightmare disorder, also known as dream anxiety disorder, is a sleep disorder characterized by frequent nightmares. The nightmares, which often portray the individual in a situation that jeopardizes their life or personal safety, usually occur during the REM stages of sleep. Though most people have experienced at least one nightmare during their life, subjects with nightmare disorder experience them with a greater frequency. The disorder's DSM-IV number is 307.47.
Psychological trauma is damage to a person's mind as a result of one or more events that cause overwhelming amounts of stress that exceed the person's ability to cope or integrate the emotions involved, eventually leading to serious, long-term negative consequences. Trauma is not the same as mental distress or suffering, both of which are universal human experiences.
Eye movement desensitization and reprocessing (EMDR) is a controversial form of psychotherapy in which the person being treated is asked to recall distressing images; the therapist then directs the patient in one type of bilateral stimulation, such as side-to-side eye rapid movement or hand tapping. EMDR was developed by Francine Shapiro starting in 1988. According to the 2013 World Health Organization (WHO) practice guideline: "This therapy [EMDR] is based on the idea that negative thoughts, feelings and behaviours are the result of unprocessed memories. The treatment involves standardized procedures that include focusing simultaneously on (a) spontaneous associations of traumatic images, thoughts, emotions and bodily sensations and (b) bilateral stimulation that is most commonly in the form of repeated eye movements."
Behaviour therapy or behavioural psychotherapy is a broad term referring to clinical psychotherapy that uses techniques derived from behaviourism and/or cognitive psychology. It looks at specific, learned behaviours and how the environment, or other people's mental states, influences those behaviours, and consists of techniques based on learning theory, such as respondent or operant conditioning. Behaviourists who practice these techniques are either behaviour analysts or cognitive-behavioural therapists. They tend to look for treatment outcomes that are objectively measurable. Behaviour therapy does not involve one specific method, but it has a wide range of techniques that can be used to treat a person's psychological problems.
Somatic experiencing is a form of alternative therapy aimed at treating trauma and stressor related disorders like PTSD. The primary goal of SE is to modify the trauma-related stress response. To achieve this, its major interventional strategy builds on bottom-up processing. Clients’ attention is directed to internal sensations,, rather than to primarily cognitive or emotional experiences. It was developed by trauma therapist Peter A. Levine.
Barbara Rothbaum is a psychologist at Emory University School of Medicine in Atlanta, Georgia. She is a professor in the Psychiatry department and a pioneer in the treatment of anxiety-related disorders. Rothbaum is head of the Trauma and Anxiety Recovery Program (TARP) at Emory as well as the Emory Healthcare Veterans Program. In the mid-1990s she founded a virtual exposure therapy company called Virtually Better, Inc. This company treats patients with anxiety disorders, addictions, pain, and the like using virtual reality instead of the actual place or scenario. It also allows the therapist to control the environment. She also played a key role in the development of the treatment of posttraumatic stress disorder (PTSD).
Flooding, sometimes referred to as in vivo exposure therapy, is a form of behavior therapy and desensitization—or exposure therapy—based on the principles of respondent conditioning. As a psychotherapeutic technique, it is used to treat phobia and anxiety disorders including post-traumatic stress disorder. It works by exposing the patient to their painful memories, with the goal of reintegrating their repressed emotions with their current awareness. Flooding was invented by psychologist Thomas Stampfl in 1967. It is still used in behavior therapy today.
Complex post-traumatic stress disorder is a psychological disorder that can develop in response to exposure to an extremely traumatic event or series of events in a context in which the individual perceives little or no chance of escape, and particularly where the exposure is prolonged or repetitive. In addition to the symptoms of post-traumatic stress disorder, an individual with C-PTSD experiences emotional dysregulation, negative self-beliefs and feelings of shame, guilt or failure regarding the trauma, and interpersonal difficulties. C-PTSD relates to the trauma model of mental disorders and is associated with chronic sexual, psychological, and physical abuse or neglect, or chronic intimate partner violence, victims of kidnapping and hostage situations, indentured servants, victims of slavery and human trafficking, sweatshop workers, prisoners of war, concentration camp survivors, residential school survivors, and prisoners kept in solitary confinement for a long period of time. It is most often directed at children and emotionally vulnerable adults, and whilst motivations behind such abuse vary, though mostly being predominantly malicious, it has also been shown that the motivations behind such abuse can be well-intentioned. Situations involving captivity/entrapment can lead to C-PTSD-like symptoms, which can include prolonged feelings of terror, worthlessness, helplessness, and deformation of one's identity and sense of self.
Virtual reality therapy (VRT), also known as virtual reality immersion therapy (VRIT), simulation for therapy (SFT), virtual reality exposure therapy (VRET), and computerized CBT (CCBT), is the use of virtual reality technology for psychological or occupational therapy and in affecting virtual rehabilitation. Patients receiving virtual reality therapy navigate through digitally created environments and complete specially designed tasks often tailored to treat a specific ailment; and is designed to isolate the user from their surrounding sensory inputs and give the illusion of immersion inside a computer-generated, interactive virtual environment. This technology has a demonstrated clinical benefit as an adjunctive analgesic during burn wound dressing and other painful medical procedures. Technology can range from a simple PC and keyboard setup, to a modern virtual reality headset. It is widely used as an alternative form of exposure therapy, in which patients interact with harmless virtual representations of traumatic stimuli in order to reduce fear responses. It has proven to be especially effective at treating PTSD, and shows considerable promise in treating a variety of neurological and physical conditions. Virtual reality therapy has also been used to help stroke patients regain muscle control, to treat other disorders such as body dysmorphia, and to improve social skills in those diagnosed with autism.

Animal-assisted therapy is an alternative or complementary type of therapy that includes the use of animals in a treatment. It falls under the realm of Animal Assisted Intervention, which encompasses any intervention in the studio that includes an animal in a therapeutic context such as emotional support animals, service animals trained to assist with daily activities, and animal assisted activity. Animal-assisted therapy can be classified by the type of animal, the targeted population, and how the animal is incorporated into the therapeutic plan. The most commonly used types of animal-assisted therapy are canine-assisted therapy and equine-assisted therapy. The goal of animal-assisted therapy is to improve a patient's social, emotional, or cognitive functioning and literature reviews state that animals can be useful for educational and motivational effectiveness for participants. Studies have documented some positive effects of the therapy on subjective self-rating scales and on objective physiological measures such as blood pressure and hormone levels.
Exposure therapy is a technique in behavior therapy to treat anxiety disorders. Exposure therapy involves exposing the target patient to the anxiety source or its context without the intention to cause any danger. Doing so is thought to help them overcome their anxiety or distress. Procedurally, it is similar to the fear extinction paradigm developed for studying laboratory rodents. Numerous studies have demonstrated its effectiveness in the treatment of disorders such as generalized anxiety disorder, social anxiety disorder, obsessive-compulsive disorder, post-traumatic stress disorder (PTSD), and specific phobias.
Prolonged exposure therapy (PE) is a form of behavior therapy and cognitive behavioral therapy designed to treat post-traumatic stress disorder. It is characterized by two main treatment procedures – imaginal and in vivo exposures. Imaginal exposure is repeated 'on-purpose' retelling of the trauma memory. In vivo exposure is gradually confronting situations, places, and things that are reminders of the trauma or feel dangerous. Additional procedures include processing of the trauma memory and breathing retraining.

Interoceptive exposure is a cognitive behavioral therapy technique used in the treatment of panic disorder. It refers to carrying out exercises that bring about the physical sensations of a panic attack, such as hyperventilation and high muscle tension, and in the process removing the patient's conditioned response that the physical sensations will cause an attack to happen.
Cognitive processing therapy (CPT) is a manualized therapy used by clinicians to help people recover from posttraumatic stress disorder (PTSD) and related conditions. It includes elements of cognitive behavioral therapy (CBT) treatments, one of the most widely used evidence-based therapies. A typical 12-session run of CPT has proven effective in treating PTSD across a variety of populations, including combat veterans, sexual assault victims, and refugees. CPT can be provided in individual and group treatment formats.
PTSD is a psychiatric disorder characterized by intrusive thoughts and memories, dreams, or flashbacks of the event; avoidance of people, places, and activities that remind the individual of the event; ongoing negative beliefs about oneself or the world, mood changes, and persistent feelings of anger, guilt, or fear; alterations in arousal such as increased irritability, angry outbursts, being hypervigilant, or having difficulty with concentration and sleep. PTSD is commonly treated with various types of psychotherapy and pharmacotherapy.

Professor Richard Allan Bryant is an Australian medical scientist. He is Scientia Professor of Psychology at the University of New South Wales (UNSW) and Director of the UNSW Traumatic Stress Clinic, based at UNSW and Westmead Institute for Medical Research. His main areas of research are Post Traumatic Stress Disorder (PTSD) and Prolonged Grief Disorder. On 13 June 2016 he was appointed a Companion of the Order of Australia (AC), for eminent service to medical research in the field of psychotraumatology, as a psychologist and author, to the study of Indigenous mental health, as an advisor to a range of government and international organisations, and to professional societies.
Internet interventions for posttraumatic stress have grown in popularity due to the limits that many patients face in their ability to seek therapy to treat their symptoms. These limits include lack of resources and residing in small towns or in the countryside. These patients may find it difficult to seek treatment because they do not have geographical access to treatment, and this can also limit the time they have to seek help. Additionally, those who live in rural areas may experience more stigma related to mental health issues. Internet interventions can increase the possibility that those who suffer from PTSD can seek help by eliminating these barriers to treatment.
Post-traumatic stress disorder (PTSD) can affect about 3.6% of the U.S. population each year, and 6.8% of the U.S. population over a lifetime. 8.4% of people in the U.S. are diagnosed with substance use disorders (SUD). Of those with a diagnosis of PTSD, a co-occurring, or comorbid diagnosis of a SUD is present in 20–35% of that clinical population.
References
- ↑ Baschnagel, J.S., Coffey, S.F., and Rash, C.J. (2006). The Treatment of Co-Occurring PTSD and Substance Use Disorders Using Trauma-Focused Exposure Therapy. IJBCT 2(4), 498-508. BAO
- ↑ Katherine Porter, Carole Porcari, Ellen I. Koc, Courtney Fons and C. Richard Spates (2006): In vivo Exposure Treatment For Agoraphobia. The Behavior Analyst Today, 7(3) 434 -445.
- ↑ Afsoon Eftekhari, Lisa R. Stines and Lori A. Zoellner (2005): Do You Need To Talk About It? Prolonged Exposure for the Treatment of Chronic PTSD. The Behavior Analyst Today, 7(1), 70- 84