
Androgen insensitivity syndrome (AIS) is a difference in sex development involving hormonal resistance due to androgen receptor dysfunction.

Primary hyperparathyroidism is a medical condition where the parathyroid gland produce excess amounts of parathyroid hormone (PTH). The symptoms of the condition relate to the resulting elevated serum calcium (hypercalcemia), which can cause digestive symptoms, kidney stones, psychiatric abnormalities, and bone disease.
Isolated hypogonadotropic hypogonadism (IHH), also called idiopathic or congenital hypogonadotropic hypogonadism (CHH), as well as isolated or congenital gonadotropin-releasing hormone deficiency (IGD), is a condition which results in a small subset of cases of hypogonadotropic hypogonadism (HH) due to deficiency in or insensitivity to gonadotropin-releasing hormone (GnRH) where the function and anatomy of the anterior pituitary is otherwise normal and secondary causes of HH are not present.

Collagen, type I, alpha 1, also known as alpha-1 type I collagen, is a protein that in humans is encoded by the COL1A1 gene. COL1A1 encodes the major component of type I collagen, the fibrillar collagen found in most connective tissues, including cartilage.

The vitamin D receptor (VDR also known as the calcitriol receptor) is a member of the nuclear receptor family of transcription factors. Calcitriol (the active form of vitamin D, 1,25-(OH)2vitamin D3) binds to VDR, which then forms a heterodimer with the retinoid-X receptor. The VDR heterodimer then enters the nucleus and binds to Vitamin D responsive elements (VDRE) in genomic DNA. VDR binding results in expression or transrepression of many specific gene products. VDR is also involved in microRNA-directed post transcriptional mechanisms. In humans, the vitamin D receptor is encoded by the VDR gene located on chromosome 12q13.11.
Glucose transporter 3, also known as solute carrier family 2, facilitated glucose transporter member 3 (SLC2A3) is a protein that in humans is encoded by the SLC2A3 gene. GLUT3 facilitates the transport of glucose across the plasma membranes of mammalian cells. GLUT3 is most known for its specific expression in neurons and has originally been designated as the neuronal GLUT. GLUT3 has been studied in other cell types with specific glucose requirements, including sperm, preimplantation embryos, circulating white blood cells and carcinoma cell lines.

Homeobox expressed in ES cells 1, also known as homeobox protein ANF, is a homeobox protein that in humans is encoded by the HESX1 gene.
Whole body vibration is a generic term used when vibrations of any frequency are transferred to the human body. Humans are exposed to vibration through a contact surface that is in a mechanical vibrating state. Humans are generally exposed to many different forms of vibration in their daily lives. This could be a driver's seat, a moving train platform, through a power tool, a training platform, or one of countless other devices. It is a potential form of occupational hazard, particularly after years of exposure.

The human gene SRD5A2 encodes the 3-oxo-5α-steroid 4-dehydrogenase 2 enzyme, also known as 5α-reductase type 2 (5αR2), one of three isozymes of 5α-reductase.
The Mechanostat is a term describing the way in which mechanical loading influences bone structure by changing the mass and architecture to provide a structure that resists habitual loads with an economical amount of material. As changes in the skeleton are accomplished by the processes of formation and resorption, the mechanostat models the effect of influences on the skeleton by those processes, through their effector cells, osteocytes, osteoblasts, and osteoclasts. The term was invented by Harold Frost: an orthopaedic surgeon and researcher described extensively in articles referring to Frost and Webster Jee's Utah Paradigm of Skeletal Physiology in the 1960s. The Mechanostat is often defined as a practical description of Wolff's law described by Julius Wolff (1836–1902), but this is not completely accurate. Wolff wrote his treatises on bone after images of bone sections were described by Culmann and von Meyer, who suggested that the arrangement of the struts (trabeculae) at the ends of the bones were aligned with the stresses experienced by the bone. It has since been established that the static methods used for those calculations of lines of stress were inappropriate for work on what were, in effect, curved beams, a finding described by Lance Lanyon, a leading researcher in the area as "a triumph of a good idea over mathematics." While Wolff pulled together the work of Culmann and von Meyer, it was the French scientist Roux, who first used the term "functional adaptation" to describe the way that the skeleton optimized itself for its function, though Wolff is credited by many for that.
Calpain-10 is a protein that in humans is encoded by the CAPN10 gene.

Nuclear receptor-interacting protein 1 (NRIP1) also known as receptor-interacting protein 140 (RIP140) is a protein that in humans is encoded by the NRIP1 gene.

Thyroid hormone receptor beta (TR-beta) also known as nuclear receptor subfamily 1, group A, member 2 (NR1A2), is a nuclear receptor protein that in humans is encoded by the THRB gene.

Hydroxyprostaglandin dehydrogenase 15-(NAD), also called 15-hydroxyprostaglandin dehydrogenase [NAD+], is an enzyme that in humans is encoded by the HPGD gene.

Arzoxifene is a selective estrogen receptor modulator (SERM) of the benzothiophene group which was never marketed. It is a potent estrogen antagonist in mammary and uterine tissue while acting as an estrogen agonist to maintain bone density and lower serum cholesterol. Arzoxifene is a highly effective agent for prevention of mammary cancer induced in the rat by the carcinogen nitrosomethylurea and is significantly more potent than raloxifene in this regard. Arzoxifene is devoid of the uterotrophic effects of tamoxifen, suggesting that, in contrast to tamoxifen, it is unlikely that the clinical use of arzoxifene will increase the risk of developing endometrial carcinoma.
Complete androgen insensitivity syndrome (CAIS) is an AIS condition that results in the complete inability of the cell to respond to androgens. As such, the insensitivity to androgens is only clinically significant when it occurs in individuals who are exposed to significant amounts of testosterone at some point in their lives. The unresponsiveness of the cell to the presence of androgenic hormones prevents the masculinization of male genitalia in the developing fetus, as well as the development of male secondary sexual characteristics at puberty, but does allow, without significant impairment, female genital and sexual development in those with the condition.
Cyril Y. Bowers, M.D., Emeritus Professor of Medicine at Tulane University School of Medicine, attended medical school at the University of Oregon and did an internship at the University of Washington. He then studied biochemistry at Cornell University and attended the Postgraduate School of Medicine at the University of Pennsylvania. From 1961-2004 he was the director of the Section of Endocrinology & Metabolism in the Department of Medicine at Tulane University School of Medicine. Dr. Bowers has served on the editorial board of several endocrine journals, was a member of the National Institute of Diabetes and Digestive and Kidney Diseases Study Section for eight years and has written over 400 articles in peer reviewed journals including chapters in books and over 200 abstracts.
Mild androgen insensitivity syndrome (MAIS) is a condition that results in a mild impairment of the cell's ability to respond to androgens. The degree of impairment is sufficient to impair spermatogenesis and / or the development of secondary sexual characteristics at puberty in males, but does not affect genital differentiation or development. Female genital and sexual development is not significantly affected by the insensitivity to androgens; as such, MAIS is only diagnosed in males. The clinical phenotype associated with MAIS is a normal male habitus with mild spermatogenic defect and / or reduced secondary terminal hair.

Michael F. Holick is an American adult endocrinologist, specializing in vitamin D, such as the identification of both calcidiol, the major circulating form of vitamin D, and calcitriol, the active form of vitamin D. His work has been the basis for diagnostic tests and therapies for vitamin D-related diseases. He is a professor of medicine at the Boston University Medical Center and editor-in-chief of the journal Clinical Laboratory.
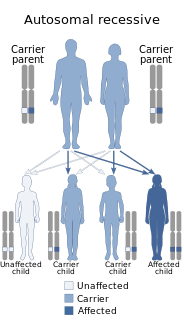
Bruck syndrome is characterized as the combination of arthrogryposis multiplex congenita and osteogenesis imperfecta. Both diseases are uncommon, but concurrence is extremely rare which makes Bruck syndrome very difficult to research. Bruck syndrome is thought to be an atypical variant of osteogenesis imperfecta most resembling type III, if not its own disease. Multiple gene mutations associated with osteogenesis imperfecta are not seen in Bruck syndrome. Many affected individuals are within the same family, and pedigree data supports that the disease is acquired through autosomal recessive inheritance. Bruck syndrome has features of congenital contractures, bone fragility, recurring bone fractures, flexion joint and limb deformities, pterygia, short body height, and progressive kyphoscoliosis. Individuals encounter restricted mobility and pulmonary function. A reduction in bone mineral content and larger hydroxyapatite crystals are also detectable Joint contractures are primarily bilateral and symmetrical, and most prone to ankles. Bruck syndrome has no effect on intelligence, vision, or hearing.