
Interstitial cystitis (IC), also known as bladder pain syndrome (BPS), is a type of chronic pain that affects the bladder. Symptoms include feeling the need to urinate right away, needing to urinate often, and pain with sex. IC/BPS is associated with depression and lower quality of life. Many of those affected also have irritable bowel syndrome and fibromyalgia.

The pudendal nerve is the main nerve of the perineum. It carries sensation from the external genitalia of both sexes and the skin around the anus and perineum, as well as the motor supply to various pelvic muscles, including the male or female external urethral sphincter and the external anal sphincter. If damaged, most commonly by childbirth, lesions may cause sensory loss or fecal incontinence. The nerve may be temporarily blocked as part of an anaesthetic procedure.
The levator ani is a broad, thin muscle group, situated on either side of the pelvis. It is formed from three muscle components: the pubococcygeus, the iliococcygeus, and the puborectalis.
Persistent genital arousal disorder (PGAD), previously called persistent sexual arousal syndrome, is spontaneous, persistent, unwanted and uncontrollable genital arousal in the absence of sexual stimulation or sexual desire, and is typically not relieved by orgasm. Instead, multiple orgasms over hours or days may be required for relief.

Kegel exercise, also known as pelvic-floor exercise, involves repeatedly contracting and relaxing the muscles that form part of the pelvic floor, now sometimes colloquially referred to as the "Kegel muscles". The exercise can be performed multiple times each day, for several minutes at a time, but takes one to three months to begin to have an effect.

Tullio Levi-Civita, was an Italian mathematician, most famous for his work on absolute differential calculus and its applications to the theory of relativity, but who also made significant contributions in other areas. He was a pupil of Gregorio Ricci-Curbastro, the inventor of tensor calculus. His work included foundational papers in both pure and applied mathematics, celestial mechanics, analytic mechanics and hydrodynamics.
Antenatal perineal massage (APM) or birth canal widening (BCW) is the massage of a pregnant woman's perineum around the opening to the vagina, performed anywhere in the 4 to 6 weeks before childbirth and usually on 4-6 separate occasions. The practice aims to more gently mimic the massaging action of a baby's head on the opening to the birth canal prior to birth, which enables some of the hard work of labour to be done before the start of labour. The intention is to attempt to prevent tearing of the perineum during birth, and reduce the need for an episiotomy or an instrument delivery.

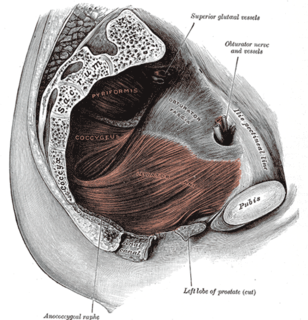
The pelvic floor or pelvic diaphragm is composed of muscle fibers of the levator ani, the coccygeus muscle, and associated connective tissue which span the area underneath the pelvis. The pelvic diaphragm is a muscular partition formed by the levatores ani and coccygei, with which may be included the parietal pelvic fascia on their upper and lower aspects. The pelvic floor separates the pelvic cavity above from the perineal region below. Because, to accommodate the birth canal, a female's pelvic cavity is larger than a male's, the pelvic floor tends to be considered a part of female anatomy, but males have an equivalent pelvic floor.
A rectocele or posterior vaginal wall prolapse results when the rectum herniates into or forms a bulge in the vagina. Two common causes of this defect are: childbirth, and hysterectomy. Rectocele also tends to occur with other forms of pelvic organ prolapse such as enterocele, sigmoidocele and cystocele.
Sexual medicine is a branch of medicine concerning the diagnosis, treatment, and prevention of disorders of sexual function. Examples of disorders treated with sexual medicine are erectile dysfunction, hypogonadism, and prostate cancer. Sexual medicine often uses a multidisciplinary approach involving physicians, mental health professionals, social workers, and sex therapists. Sexual medicine physicians often approfhkdhvbehrbkehbvh3rfehbrehyfbkfhach treatment with medicine and surgery, while sex therapists often focus on behavioral treatments.

A cystocele, also known as a prolapsed bladder, is a medical condition in which a woman's bladder bulges into her vagina. Some may have no symptoms. Other may have trouble starting urination, urinary incontinence, or frequent urination. Complications may include recurrent urinary tract infections and urinary retention. Cystocele and a prolapsed urethra often occur together and is called a cystourethrocele. Cystocele can negatively affect quality of life.
Sex after pregnancy is often delayed for several weeks or months, and may be difficult and painful for women. Injury to the perineum or surgical cuts (episiotomy) to the vagina during childbirth can cause sexual dysfunction. Sexual activity in the postpartum period other than sexual intercourse is possible sooner, but some women experience a prolonged loss of sexual desire after giving birth, which may be associated with postnatal depression. Common issues that may last more than a year after birth are greater desire by the man than the woman, and a worsening of the woman's body image.

A perineal tear is a laceration of the skin and other soft tissue structures which, in women, separate the vagina from the anus. Perineal tears mainly occur in women as a result of vaginal childbirth, which strains the perineum. It is the most common form of obstetric injury. Tears vary widely in severity. The majority are superficial and may require no treatment, but severe tears can cause significant bleeding, long-term pain or dysfunction. A perineal tear is distinct from an episiotomy, in which the perineum is intentionally incised to facilitate delivery. Episiotomy, a very rapid birth, or large fetal size can lead to more severe tears which may require surgical intervention.

The pelvis is either the lower part of the trunk of the human body between the abdomen and the thighs or the skeleton embedded in it.
Descending perineum syndrome refers to a condition where the perineum "balloons" several centimeters below the bony outlet of the pelvis during strain, although this descent may happen without straining. The syndrome was first described in 1966 by Parks et al.
The Pelvic Organ Prolapse Quantifications System (POP-Q) is a system for assessing the degree of prolapse of pelvic organs to help standardize diagnosing, comparing, documenting, and sharing of clinical findings. This assessment is the most frequently used among research publications related to pelvic organ prolapse.
A urogenital fistula is an abnormal tract that exists between the urinary tract and bladder, ureters, or urethra. A urogenital fistula can occur between any of the organs and structures of the pelvic region. A fistula allows urine to continually exit through and out the urogenital tract. This can result in significant disability, interference with sexual activity, and other physical health issues, the effects of which may in turn have a negative impact on mental or emotional state, including an increase in social isolation. Urogenital fistulas vary in etiology. Fistulas are usually caused by injury or surgery, but they can also result from malignancy, infection, prolonged and obstructed labor and deliver in childbirth, hysterectomy, radiation therapy or inflammation. Of the fistulas that develop from difficult childbirth, 97 percent occur in developing countries. Congenital urogenital fistulas are rare; only ten cases have been documented. Abnormal passageways can also exist between the vagina and the organs of the gastrointestinal system, and these may also be termed fistulas.
The pubovaginal muscle is a pelvic floor muscle that attaches to the muscles of lateral walls of the midsection of the vagina and the pubis. It is relatively short compared to the other levator ani muscles and extends between the rectum and the vagina. Other muscles that are part of the levator ani are: the pubovisceral muscle which is made up of the puboperineal; pubovaginal, and puboanal muscles; the puborectal muscle; and the iliococcygeal muscle. The pubovaginal muscle was identified by anatomists as early as 1912.

Critical emergency medicine (CREM) refers to the acute medical care of patients who have medical emergencies that pose an immediate threat to life, irrespective of location. In particular, the term is used to describe the role of anaesthesiologists in providing such care.