Related Research Articles

Anaplastic large-cell lymphoma (ALCL) refers to a group of non-Hodgkin lymphomas in which aberrant T cells proliferate uncontrollably. Considered as a single entity, ALCL is the most common type of peripheral lymphoma and represents ~10% of all peripheral lymphomas in children. The incidence of ALCL is estimated to be 0.25 cases per 100,000 people in the United States of America. There are four distinct types of anaplastic large-cell lymphomas that on microscopic examination share certain key histopathological features and tumor marker proteins. However, the four types have very different clinical presentations, gene abnormalities, prognoses, and/or treatments.

Mycosis fungoides, also known as Alibert-Bazin syndrome or granuloma fungoides, is the most common form of cutaneous T-cell lymphoma. It generally affects the skin, but may progress internally over time. Symptoms include rash, tumors, skin lesions, and itchy skin.

Cutaneous T-cell lymphoma (CTCL) is a class of non-Hodgkin lymphoma, which is a type of cancer of the immune system. Unlike most non-Hodgkin lymphomas, CTCL is caused by a mutation of T cells. The cancerous T cells in the body initially migrate to the skin, causing various lesions to appear. These lesions change shape as the disease progresses, typically beginning as what appears to be a rash which can be very itchy and eventually forming plaques and tumors before spreading to other parts of the body.
Follicular lymphoma (FL) is a cancer that involves certain types of white blood cells known as lymphocytes. The cancer originates from the uncontrolled division of specific types of B-cells known as centrocytes and centroblasts. These cells normally occupy the follicles in the germinal centers of lymphoid tissues such as lymph nodes. The cancerous cells in FL typically form follicular or follicle-like structures in the tissues they invade. These structures are usually the dominant histological feature of this cancer.

Sézary disease, or Sézary syndrome, is a type of cutaneous T-cell lymphoma that was first described by Albert Sézary. The affected T cells, known as Sézary's cells or Lutzner cells, have pathological quantities of mucopolysaccharides. Sézary disease is sometimes considered a late stage of mycosis fungoides with lymphadenopathy.
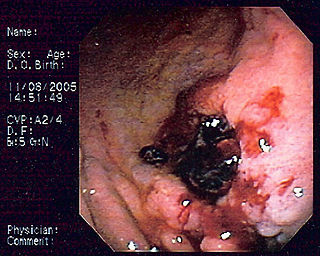
MALT lymphoma is a form of lymphoma involving the mucosa-associated lymphoid tissue (MALT), frequently of the stomach, but virtually any mucosal site can be affected. It is a cancer originating from B cells in the marginal zone of the MALT.

Golfer's vasculitis, also called exercise-induced vasculitis, sport-induced vasculitis, Disney rash, or hiker's rash, is a form of small blood vessel inflammation resulting in a rash. It occurs in the lower legs, and is caused by excessive walking in hot temperatures. It is more common in elderly people.

Intravascular lymphomas (IVL) are rare cancers in which malignant lymphocytes proliferate and accumulate within blood vessels. Almost all other types of lymphoma involve the proliferation and accumulation of malignant lymphocytes in lymph nodes, other parts of the lymphatic system, and various non-lymphatic organs but not in blood vessels.
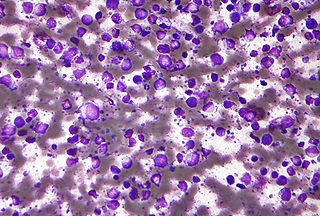
Diffuse large B-cell lymphoma (DLBCL) is a cancer of B cells, a type of lymphocyte that is responsible for producing antibodies. It is the most common form of non-Hodgkin lymphoma among adults, with an annual incidence of 7–8 cases per 100,000 people per year in the US and UK. This cancer occurs primarily in older individuals, with a median age of diagnosis at ~70 years, although it can occur in young adults and, in rare cases, children. DLBCL can arise in virtually any part of the body and, depending on various factors, is often a very aggressive malignancy. The first sign of this illness is typically the observation of a rapidly growing mass or tissue infiltration that is sometimes associated with systemic B symptoms, e.g. fever, weight loss, and night sweats.

Marginal zone lymphomas, also known as marginal zone B-cell lymphomas (MZLs), are a heterogeneous group of lymphomas that derive from the malignant transformation of marginal zone B-cells. Marginal zone B cells are innate lymphoid cells that normally function by rapidly mounting IgM antibody immune responses to antigens such as those presented by infectious agents and damaged tissues. They are lymphocytes of the B-cell line that originate and mature in secondary lymphoid follicles and then move to the marginal zones of mucosa-associated lymphoid tissue (MALT), the spleen, or lymph nodes. Mucosa-associated lymphoid tissue is a diffuse system of small concentrations of lymphoid tissue found in various submucosal membrane sites of the body such as the gastrointestinal tract, mouth, nasal cavity, pharynx, thyroid gland, breast, lung, salivary glands, eye, skin and the human spleen.

Pagetoid reticulosis is a cutaneous condition, an uncommon lymphoproliferative disorder, sometimes considered a form of mycosis fungoides.
Primary cutaneous anaplastic large cell lymphoma belongs to the group of cutaneous processes that are CD30+ lymphoproliferative and are characterized by autoregressive, recurrent, single or multifocal ulcerating nodules. Single or localized nodules, papules, or plaques are present in the majority of patients. However, a patient may have more than one lesion in up to 20% of cases.
Subcutaneous T-cell lymphoma is a cutaneous condition that most commonly presents in young adults, and is characterized by subcutaneous nodules. Common symptoms include fever, fatigue, and pancytopenia.
Cutaneous B-cell lymphomas (CBCL), more recently termed Primary cutaneous B-cell lymphomas and lymphoproliferative disorders (PCBCLPD), are a group of disorders that typically present as skin lesions consisting of proliferating B-cells. B-cells are a type of lymphocyte involved in regulating immune responses. Since its original definition in 1997, CBCL has been considered to have a varying number of subtypes by the European Organisation for Research and Treatment of Cancer, i.e., EORTC, and World Health Organization, i.e., WHO. The latest revised classification of CBCL, which was published by EORTC in 2022, lists the following three main subtypes of CBCL :
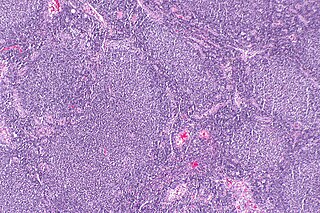
Primary cutaneous marginal zone lymphomas represent a heterogeneous group of diseases characterized by solitary or multiple dermal or subcutaneous nodules. Lymphomas included in this group are:
Primary cutaneous follicle center lymphoma is a type of lymphoma. It was recognized as a distinct disease entity in the 2008 WHO classification. PCFCL had been previously conceived as a variant of follicular lymphoma (FL).
Epstein–Barr virus–associated lymphoproliferative diseases are a group of disorders in which one or more types of lymphoid cells, i.e. B cells, T cells, NK cells, and histiocytic-dendritic cells, are infected with the Epstein–Barr virus (EBV). This causes the infected cells to divide excessively, and is associated with the development of various non-cancerous, pre-cancerous, and cancerous lymphoproliferative disorders (LPDs). These LPDs include the well-known disorder occurring during the initial infection with the EBV, infectious mononucleosis, and the large number of subsequent disorders that may occur thereafter. The virus is usually involved in the development and/or progression of these LPDs although in some cases it may be an "innocent" bystander, i.e. present in, but not contributing to, the disease.
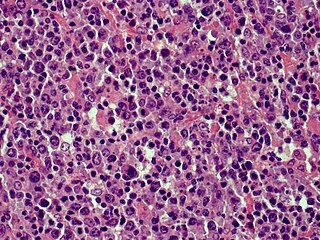
Primary cutaneous diffuse large B-cell lymphoma, leg type (PCDLBCL-LT) is a cutaneous lymphoma skin disease that occurs mostly in elderly females. In this disease, B cells become malignant, accumulate in the dermis and subcutaneous tissue below the dermis to form red and violaceous skin nodules and tumors. These lesions typically occur on the lower extremities but in uncommon cases may develop on the skin at virtually any other site. In ~10% of cases, the disease presents with one or more skin lesions none of which are on the lower extremities; the disease in these cases is sometimes regarded as a variant of PCDLBL, LT termed primary cutaneous diffuse large B-cell lymphoma, other (PCDLBC-O). PCDLBCL, LT is a subtype of the diffuse large B-cell lymphomas (DLBCL) and has been thought of as a cutaneous counterpart to them. Like most variants and subtypes of the DLBCL, PCDLBCL, LT is an aggressive malignancy. It has a 5-year overall survival rate of 40–55%, although the PCDLBCL-O variant has a better prognosis than cases in which the legs are involved.
Cutaneous manifestations of COVID-19 are characteristic signs or symptoms of the Coronavirus disease 2019 that occur in the skin. The American Academy of Dermatology reports that skin lesions such as morbilliform, pernio, urticaria, macular erythema, vesicular purpura, papulosquamous purpura and retiform purpura are seen in people with COVID-19. Pernio-like lesions were more common in mild disease while retiform purpura was seen only in critically ill patients. The major dermatologic patterns identified in individuals with COVID-19 are urticarial rash, confluent erythematous/morbilliform rash, papulovesicular exanthem, chilbain-like acral pattern, livedo reticularis and purpuric "vasculitic" pattern. Chilblains and Multisystem inflammatory syndrome in children are also cutaneous manifestations of COVID-19.
Günter Burg is a German dermatologist. Born in Mayen, Germany, he holds German and Swiss citizenship. He has been married to Dr. Doris Burg-Nicklas, a neurologist, since 1968. They have two sons: Andreas and Thomas.
References
- ↑ Magro CM, Porcu P, Ahmad N, Klinger D, Crowson AN, Nuovo G (September 2004). "Cutaneous immunocytoma: a clinical, histologic, and phenotypic study of 11 cases". Applied Immunohistochemistry & Molecular Morphology : AIMM. 12 (3): 216–24. doi:10.1097/00129039-200409000-00006. PMID 15551734.
- ↑ Rijlaarsdam JU, van der Putte SC, Berti E, Kerl H, Rieger E, Toonstra J, Geerts ML, Meijer CJ, Willemze R (August 1993). "Cutaneous immunocytomas: a clinicopathologic study of 26 cases". Histopathology. 23 (2): 117–25. doi:10.1111/j.1365-2559.1993.tb00469.x. PMID 8406383.
- ↑ Willemze R, Jaffe ES, Burg G, Cerroni L, Berti E, Swerdlow SH, Ralfkiaer E, Chimenti S, Diaz-Perez JL, Duncan LM, Grange F, Harris NL, Kempf W, Kerl H, Kurrer M, Knobler R, Pimpinelli N, Sander C, Santucci M, Sterry W, Vermeer MH, Wechsler J, Whittaker S, Meijer CJ (May 2005). "WHO-EORTC classification for cutaneous lymphomas". Blood. 105 (10): 3768–85. doi:10.1182/blood-2004-09-3502. PMID 15692063.
| | This cutaneous condition article is a stub. You can help Wikipedia by expanding it. |