Related Research Articles

Cholesteatoma is a destructive and expanding growth consisting of keratinizing squamous epithelium in the middle ear and/or mastoid process. Cholesteatomas are not cancerous as the name may suggest, but can cause significant problems because of their erosive and expansile properties. This can result in the destruction of the bones of the middle ear (ossicles), as well as growth through the base of the skull into the brain. They often become infected and can result in chronically draining ears. Treatment almost always consists of surgical removal.

The parotid gland is a major salivary gland in many animals. In humans, the two parotid glands are present on either side of the mouth and in front of both ears. They are the largest of the salivary glands. Each parotid is wrapped around the mandibular ramus, and secretes serous saliva through the parotid duct into the mouth, to facilitate mastication and swallowing and to begin the digestion of starches. There are also two other types of salivary glands; they are submandibular and sublingual glands. Sometimes accessory parotid glands are found close to the main parotid glands.

Cauliflower ear is an irreversible condition that occurs when the external portion of the ear is hit and develops a blood clot or other collection of fluid under the perichondrium. This separates the cartilage from the overlying perichondrium that supplies its nutrients, causing it to die and resulting in the formation of fibrous tissue in the overlying skin. As a result, the outer ear becomes permanently swollen and deformed, resembling a cauliflower, hence the name.
Otoplasty is a procedure for correcting the deformities and defects of the auricle, whether these defects are congenital conditions or caused by trauma. Otoplastic surgeons may reshape, move, or augment the cartilaginous support framework of the auricle to correct these defects.

A pancreatic pseudocyst is a circumscribed collection of fluid rich in pancreatic enzymes, blood, and non-necrotic tissue, typically located in the lesser sac of the abdomen. Pancreatic pseudocysts are usually complications of pancreatitis, although in children they frequently occur following abdominal trauma. Pancreatic pseudocysts account for approximately 75% of all pancreatic masses.

Pseudocysts are like cysts, but lack epithelial or endothelial cells. Initial management consists of general supportive care. Symptoms and complications caused by pseudocysts require surgery. Computed tomography (CT) scans are used for initial imaging of cysts, and endoscopic ultrasounds are used in differentiating between cysts and pseudocysts. Endoscopic drainage is a popular and effective method of treating pseudocysts.

Relapsing polychondritis is a systemic disease characterized by repeated episodes of inflammation and in some cases deterioration of cartilage. The disease can be life-threatening if the respiratory tract, heart valves, or blood vessels are affected. The exact mechanism is poorly understood.

Lymphangiomas are malformations of the lymphatic system characterized by lesions that are thin-walled cysts; these cysts can be macroscopic, as in a cystic hygroma, or microscopic. The lymphatic system is the network of vessels responsible for returning to the venous system excess fluid from tissues as well as the lymph nodes that filter this fluid for signs of pathogens. These malformations can occur at any age and may involve any part of the body, but 90% occur in children less than 2 years of age and involve the head and neck. These malformations are either congenital or acquired. Congenital lymphangiomas are often associated with chromosomal abnormalities such as Turner syndrome, although they can also exist in isolation. Lymphangiomas are commonly diagnosed before birth using fetal ultrasonography. Acquired lymphangiomas may result from trauma, inflammation, or lymphatic obstruction.

Surfer's ear is the common name for an exostosis or abnormal bone growth within the ear canal. They are otherwise benign hyperplasias (growths) of the tympanic bone thought to be caused by frequent cold-water exposure. Cases are often asymptomatic. Surfer's ear is not the same as swimmer's ear, although infection can result as a side effect.
Subglottic stenosis is a congenital or acquired narrowing of the subglottic airway. It can be congenital, acquired, iatrogenic, or very rarely, idiopathic. It is defined as the narrowing of the portion of the airway that lies between the vocal cords and the lower part of the cricoid cartilage. In a normal infant, the subglottic airway is 4.5-5.5 millimeters wide, while in a premature infant, the normal width is 3.5 millimeters. Subglottic stenosis is defined as a diameter of under 4 millimeters in an infant. Acquired cases are more common than congenital cases due to prolonged intubation being introduced in the 1960s. It is most frequently caused by certain medical procedures or external trauma, although infections and systemic diseases can also cause it.
Fibromatosis colli (FMC), also termed sternocleidomastoid tumor of infancy, pseudotumor of infancy, and infancy sternocleidomastoid pseudotumor, is an uncommon, congenital tumor in one of the two sternocleidomastoid neck muscles although rare cases have presented with a FMC tumor in both sternocleidomastoid muscles. A tumor is here defined as a growth of tissue that is not coordinated with the normal surrounding tissue and persists in growing even if the original trigger for its growth is removed. FMC tumors are benign growths that may cause disfigurements but are not cancers and do not metastasize to distant tissues.

Chondrodermatitis nodularis chronica helicis(CNCH) is a small, nodular, tender, chronic inflammatory lesion occurring on the helix of the ear, most often in men. it often presents as a benign painful erythematous nodule fixed to the cartilage of the helix or antihelix of the external ear. Although the exact cause of the condition is unknown, it has been linked to head pressure on the ear while sleeping. Treatment options include the use of pressure-relieving devices or, in cases where that is not an option, surgery.
A cutaneous myxoma, or superficial angiomyxoma, consists of a multilobulated myxoid mass containing stellate or spindled fibroblasts with pools of mucin forming cleft-like spaces. There is often a proliferation of blood vessels and an inflammatory infiltrate. Staining is positive for vimentin, negative for cytokeratin and desmin, and variable for CD34, Factor VIIIa, SMA, MSA and S-100.
Traumatic anserine folliculosis is a curious gooseflesh-like follicular hyperkeratosis that may result from persistent pressure and lateral friction of one skin surface against another. Traumatic anserine folliculosis is caused by trauma. Topical keratolytics are the treatment of choice.
Idiopathic scrotal calcinosis is a cutaneous condition characterized by calcification of the skin resulting from the deposition of calcium and phosphorus occurring on the scrotum. However, the levels of calcium and phosphate in the blood are normal. Idiopathic scrotal calcinosis typically affects young males, with an onset between adolescence and early adulthood. The scrotal calcinosis appears, without any symptoms, as yellowish nodules that range in size from 1 mm to several centimeters.

An accessory auricle is a congenital anomaly typically seen as a skin coloured nodule, most frequently just to the front of the ear.

Tympanosclerosis is a condition caused by hyalinization and subsequent calcification of subepithelial connective tissue of the tympanic membrane and middle ear, sometimes resulting in a detrimental effect to hearing.
Laryngeal cysts are cysts involving the larynx or more frequently supraglottic locations, such as epiglottis and vallecula. Usually they do not extend to the thyroid cartilage. They may be present congenitally or may develop eventually due to degenerative cause. They often interfere with phonation.
Laryngotracheal reconstruction is a surgical procedure that involves expanding or removing parts of the airway to widen a narrowing within it, called laryngotracheal stenosis or subglottic stenosis.

Intubation granuloma is a benign growth of granulation tissue in the larynx or trachea, which arises from tissue trauma due to endotracheal intubation. This medical condition is described as a common late complication of tracheal intubation, specifically caused by irritation to the mucosal tissue of the airway during insertion or removal of the patient's intubation tube.
References
- 1 2 3 Patel, KrinaB; Agrawal, PriyaU; Chauhan, VasimF; Nagani, SavfeenaM (2020). "Pseudocyst of auricle—An uncommon condition and novel approach for management". Indian Dermatology Online Journal. 11 (5). Medknow: 789–791. doi: 10.4103/idoj.idoj_532_19 . ISSN 2229-5178. PMC 7678522 . PMID 33235847.
- ↑ Rapini, Ronald P.; Bolognia, Jean L.; Jorizzo, Joseph L. (2007). Dermatology: 2-Volume Set. St. Louis: Mosby. ISBN 978-1-4160-2999-1.
- ↑ James, William D.; Berger, Timothy G.; et al. (2006). Andrews' Diseases of the Skin: Clinical Dermatology. Saunders Elsevier. ISBN 978-0-7216-2921-6.
- ↑ Beutler, Bryce D.; Cohen, Philip R. (2015-10-31). "Pseudocyst of the auricle in patients with movement disorders: report of two patients with ataxia-associated auricular pseudocysts". Dermatology Practical & Conceptual. 5 (4). Mattioli1885: 59–64. doi:10.5826/dpc.0504a15. ISSN 2160-9381. PMID 26693094.
- ↑ Khan, NazirA; ul Islam, Mudasir; ur Rehman, Ayaz; Ahmad, Shakeel (2013). "Pseudocyst of pinna and its treatment with surgical Deroofing: An experience at tertiary hospitals". Journal of Surgical Technique and Case Report. 5 (2). CLOCKSS Archive: 72. doi: 10.4103/2006-8808.128728 . ISSN 2006-8808. PMID 24741423.
- ↑ Cohen, P. R.; Grossman, M. E. (1990-10-01). "Pseudocyst of the Auricle: Case Report and World Literature Review". Archives of Otolaryngology — Head and Neck Surgery. 116 (10). American Medical Association (AMA): 1202–1204. doi:10.1001/archotol.1990.01870100096021. ISSN 0886-4470. PMID 2206508.
- ↑ Santos, Vladimir B.; Polisar, Ira A.; Ruffy, Mauro L. (1974). "Bilateral Pseudocysts of the Auricle in a Female". Annals of Otology, Rhinology & Laryngology. 83 (1). SAGE Publications: 9–11. doi:10.1177/000348947408300103. ISSN 0003-4894. PMID 4811583.
- ↑ Abdel Tawab, Hazem; Tabook, Salim (2019-02-06). "Incision and Drainage with Daily Irrigation for the Treatment of Auricular Pseudocyst". International Archives of Otorhinolaryngology. 23 (2). Georg Thieme Verlag KG: 178–183. doi:10.1055/s-0038-1676124. ISSN 1809-9777. PMID 30956702.
- ↑ Ballan, Anthony; Zogheib, Serge; Hanna, Cyril; Daou, Bechara; Nasr, Marwan; Jabbour, Samer (2021-08-04). "Auricular pseudocysts: a systematic review of the literature". International Journal of Dermatology. 61 (1). Wiley: 109–117. doi:10.1111/ijd.15816. ISSN 0011-9059. PMID 34348416.
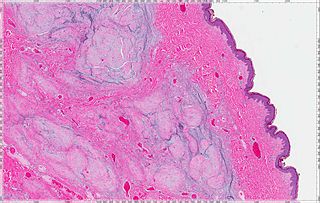
- ↑ Ming, Lim Chwee; Hong, Goh Yau; Shuen, Chao Siew; Lim, Lynne (2004). "Pseudocyst of the Auricle: A Histologic Perspective". The Laryngoscope. 114 (7). Wiley: 1281–1284. doi:10.1097/00005537-200407000-00026. ISSN 0023-852X.
- ↑ Zhu, L.; Wang, X. (1992). "Histological examination of the auricular cartilage and pseudocyst of the auricle". The Journal of Laryngology and Otology. 106 (2): 103–104. doi:10.1017/S002221510011881X. ISSN 0022-2151. PMID 1556479.
- ↑ Juan, Kai-Hui (1994). "Pseudocyst of the Auricle: Steroid Therapy". Auris Nasus Larynx. 21 (1). Elsevier BV: 8–12. doi:10.1016/s0385-8146(12)80003-4. ISSN 0385-8146.
- ↑ Ophir, Dov; Marshak, Gabriel; a, Kfar-Sab (1991). "Needle Aspiration and Pressure Sutures for Auricular Pseudocyst". Plastic and Reconstructive Surgery. 87 (4). Ovid Technologies (Wolters Kluwer Health): 783–784. doi:10.1097/00006534-199104000-00030. ISSN 0032-1052. PMID 2008480.
- ↑ Hegde, Ramesh; Bhargava, Samir; Bhargava, K. B. (1996). "Pseudocyst of the auricle: a new method of treatment". The Journal of Laryngology & Otology. 110 (8): 767–769. doi:10.1017/S0022215100134917. ISSN 0022-2151. PMID 8869613.
- ↑ Harder, Mary K.; Zachary, C. B. (1993). "Pseudocyst of the Ear: Surgical Treatment". The Journal of Dermatologic Surgery and Oncology. 19 (6): 585–588. doi:10.1111/j.1524-4725.1993.tb00394.x. ISSN 0148-0812. PMID 8509521.
- ↑ Schulte, Klaus W.; Neumann, Norbert J.; Ruzicka, Thomas (2001). "Surgical pearl: The close-fitting ear cover cast? a noninvasive treatment for pseudocyst of the ear". Journal of the American Academy of Dermatology. 44 (2). Elsevier BV: 285–287. doi:10.1067/mjd.2001.111616. ISSN 0190-9622. PMID 11174388.