Related Research Articles
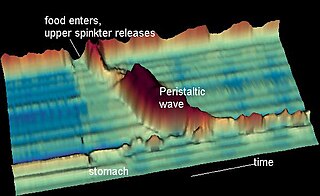
Peristalsis is a type of intestinal motility, characterized by radially symmetrical contraction and relaxation of muscles that propagate in a wave down a tube, in an anterograde direction. Peristalsis is progression of coordinated contraction of involuntary circular muscles, which is preceded by a simultaneous contraction of the longitudinal muscle and relaxation of the circular muscle in the lining of the gut.

The esophagus or oesophagus, colloquially known also as the food pipe, food tube, or gullet, is an organ in vertebrates through which food passes, aided by peristaltic contractions, from the pharynx to the stomach. The esophagus is a fibromuscular tube, about 25 cm (10 in) long in adults, that travels behind the trachea and heart, passes through the diaphragm, and empties into the uppermost region of the stomach. During swallowing, the epiglottis tilts backwards to prevent food from going down the larynx and lungs. The word oesophagus is from Ancient Greek οἰσοφάγος (oisophágos), from οἴσω (oísō), future form of φέρω + ἔφαγον.
Heartburn, also known as pyrosis, cardialgia or acid indigestion, is a burning sensation in the central chest or upper central abdomen. Heartburn is usually due to regurgitation of gastric acid into the esophagus. It is the major symptom of gastroesophageal reflux disease (GERD).

Esophagitis, also spelled oesophagitis, is a disease characterized by inflammation of the esophagus. The esophagus is a tube composed of a mucosal lining, and longitudinal and circular smooth muscle fibers. It connects the pharynx to the stomach; swallowed food and liquids normally pass through it.

The thoracic diaphragm, or simply the diaphragm, is a sheet of internal skeletal muscle in humans and other mammals that extends across the bottom of the thoracic cavity. The diaphragm is the most important muscle of respiration, and separates the thoracic cavity, containing the heart and lungs, from the abdominal cavity: as the diaphragm contracts, the volume of the thoracic cavity increases, creating a negative pressure there, which draws air into the lungs. Its high oxygen consumption is noted by the many mitochondria and capillaries present; more than in any other skeletal muscle.

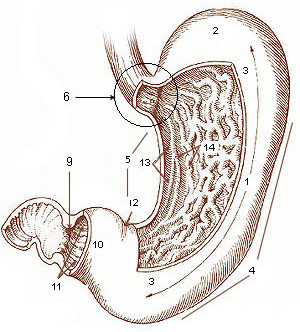
The pylorus connects the stomach to the duodenum. The pylorus is considered as having two parts, the pyloric antrum and the pyloric canal. The pyloric canal ends as the pyloric orifice, which marks the junction between the stomach and the duodenum. The orifice is surrounded by a sphincter, a band of muscle, called the pyloric sphincter. The word pylorus comes from Greek πυλωρός, via Latin. The word pylorus in Greek means "gatekeeper", related to "gate" and is thus linguistically related to the word "pylon".
The pharyngeal reflex or gag reflex is a reflex muscular contraction of the back of the throat, evoked by touching the roof of the mouth, back of the tongue, area around the tonsils, uvula, and back of the throat. It, along with other aerodigestive reflexes such as reflexive pharyngeal swallowing, prevents objects in the oral cavity from entering the throat except as part of normal swallowing and helps prevent choking, and is a form of coughing. The pharyngeal reflex is different from the laryngeal spasm, which is a reflex muscular contraction of the vocal cords.

Esophagogastroduodenoscopy (EGD) or oesophagogastroduodenoscopy (OGD), also called by various other names, is a diagnostic endoscopic procedure that visualizes the upper part of the gastrointestinal tract down to the duodenum. It is considered a minimally invasive procedure since it does not require an incision into one of the major body cavities and does not require any significant recovery after the procedure. However, a sore throat is common.

Mallory–Weiss syndrome is a condition where high intra-abdominal pressures causes laceration and bleeding of the mucosa called Mallory-Weiss tears. Additionally, Mallory–Weiss syndrome is one of the most common causes of acute upper gastrointestinal bleeding, counting of around 1-15% of all cases in adults and less than 5% in children. It has been found that tears are up to 2 to 4 times more prevalent in men than women. The tears can cause upper gastrointestinal bleeding and predominantly occur where the esophagus meets the stomach. However, the tears can happen anywhere from the middle of the esophagus to the cardia of the stomach. Mallory–Weiss syndrome is often caused by constant vomiting and retching from alcoholism or bulimia. Gastroesophageal reflux disease (GERD) is another risk factor that is often linked with Mallory–Weiss syndrome. However, not every individual with Mallory–Weiss syndrome will have these risk factors. Individuals with Mallory–Weiss syndrome will have hematemesis, however the symptoms can vary.
Dumping syndrome occurs when food, especially sugar, moves too quickly from the stomach to the duodenum—the first part of the small intestine—in the upper gastrointestinal (GI) tract. This condition is also called rapid gastric emptying. It is mostly associated with conditions following gastric or esophageal surgery, though it can also arise secondary to diabetes or to the use of certain medications; it is caused by an absent or insufficiently functioning pyloric sphincter, the valve between the stomach and the duodenum.
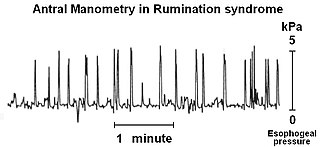
Rumination syndrome, or merycism, is a chronic motility disorder characterized by effortless regurgitation of most meals following consumption, due to the involuntary contraction of the muscles around the abdomen. There is no retching, nausea, heartburn, odour, or abdominal pain associated with the regurgitation as there is with typical vomiting, and the regurgitated food is undigested. The disorder has been historically documented as affecting only infants, young children, and people with cognitive disabilities . It is increasingly being diagnosed in a greater number of otherwise healthy adolescents and adults, though there is a lack of awareness of the condition by doctors, patients, and the general public.
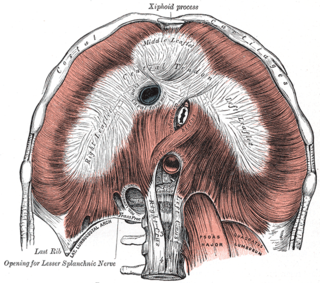
In human anatomy, the esophageal hiatus is an opening in the diaphragm through which the esophagus and the vagus nerve pass.
Retroperistalsis is the reverse of the involuntary smooth muscle contractions of peristalsis. It usually occurs as a precursor to vomiting. Local irritation of the stomach, such as bacteria or food poisoning, activates the emetic center of the brain which in turn signals an imminent vomiting reflex. Retroperistalsis begins in the small intestine and pyloric sphincter. Food then moves in the opposite direction, often from the duodenum into the stomach.

Vomiting is the involuntary, forceful expulsion of the contents of one's stomach through the mouth and sometimes the nose.
Gastric volvulus or volvulus of stomach is a twisting of all or part of the stomach by more than 180 degrees with obstruction of the flow of material through the stomach, variable loss of blood supply and possible tissue death. The twisting can occur around the long axis of the stomach: this is called organoaxial or around the axis perpendicular to this, called mesenteroaxial. Obstruction is more likely in organoaxial twisting than with mesenteroaxial while the latter is more associated with ischemia. About one third of the cases are associated with a hiatus hernia. Treatment is surgical.
The muscles of respiration are the muscles that contribute to inhalation and exhalation, by aiding in the expansion and contraction of the thoracic cavity. The diaphragm and, to a lesser extent, the intercostal muscles drive respiration during quiet breathing. The elasticity of these muscles is crucial to the health of the respiratory system and to maximize its functional capabilities.

Gastroparesis, also called delayed gastric emptying, is a medical disorder consisting of weak muscular contractions (peristalsis) of the stomach, resulting in food and liquid remaining in the stomach for a prolonged period of time. Stomach contents thus exit more slowly into the duodenum of the digestive tract. This can result in irregular absorption of nutrients, inadequate nutrition, and poor glycemic control. The opposite of this, where stomach contents exit quickly into the duodenum, is called dumping syndrome.

Nausea is a diffuse sensation of unease and discomfort, sometimes perceived as an urge to vomit. It can be a debilitating symptom if prolonged and has been described as placing discomfort on the chest, abdomen, or back of the throat.
The nervous system, and endocrine system collaborate in the digestive system to control gastric secretions, and motility associated with the movement of food throughout the gastrointestinal tract, including peristalsis, and segmentation contractions.

The human digestive system consists of the gastrointestinal tract plus the accessory organs of digestion. Digestion involves the breakdown of food into smaller and smaller components, until they can be absorbed and assimilated into the body. The process of digestion has three stages: the cephalic phase, the gastric phase, and the intestinal phase.
References
- ↑ "Vomiting and Nausea". eMedicine . February 12, 2012.
- 1 2 Lang, IM; Dana, N; Medda, BK; Shaker, R (September 2002). "Mechanisms of airway protection during retching, vomiting, and swallowing". American Journal of Physiology. Gastrointestinal and Liver Physiology. 283 (3): G529-36. doi:10.1152/ajpgi.00062.2002. PMID 12181164.
- ↑ Schindler, R (1937). Gastroscopy. Chicago: University of Chicago Press. p. 145.
- ↑ Keet, AD (1998). "Nausea, Retching, and Vomiting". The Pyloric Sphincteric Cylinder in Health and Disease. PLiG. p. 122.
- ↑ Berne, Robert M.; Matthew N. Levy (2004). Physiology. Elsevier Mosby. p. 557. ISBN 0-323-03390-3.
- 1 2 Andrews, PL; Davis, CJ; Bingham, S; Davidson, HI; Hawthorn, J; Maskell, L (February 1990). "The abdominal visceral innervation and the emetic reflex: pathways, pharmacology, and plasticity". Canadian Journal of Physiology and Pharmacology. 68 (2): 325–45. doi:10.1139/y90-047. PMID 2178756.
- ↑ Grelot, L; Miller, AD (1994). "Vomiting - Its Ins and Outs". News in Physiological Sciences. 9 (3): 142–147.
- ↑ Horn, Charles (11 October 2007). "Why is the neurobiology of nausea and vomiting so important?". Appetite. 50 (2–3): 430–434. doi:10.1016/j.appet.2007.09.015. PMC 2274963 . PMID 17996982. nihmsid: NIHMS42868.
- ↑ Porter, Ryan F.; Gyawali, C. Prakash. "Nausea and Vomiting". Patient Education & Resource Center. American College of Gastroenterology.