
Scoliosis is a medical condition in which a person's spine has a sideways curve. The curve is usually "S"- or "C"-shaped over three dimensions. In some, the degree of curve is stable, while in others, it increases over time. Mild scoliosis does not typically cause problems, but more severe cases can affect breathing and movement. Pain is usually present in adults, and can worsen with age.

An intervertebral disc lies between adjacent vertebrae in the vertebral column. Each disc forms a fibrocartilaginous joint, to allow slight movement of the vertebrae, to act as a ligament to hold the vertebrae together, and to function as a shock absorber for the spine.
Bone age is the degree of maturation of a child's bones. As a person grows from fetal life through childhood, puberty, and finishes growth as a young adult, the bones of the skeleton change in size and shape. These changes can be seen by x-ray techniques. The "bone age" of a child is the average age at which children reach various stages of bone maturation. A child's current height and bone age can be used to predict adult height. For most people, their bone age is the same as their biological age but for some individuals, their bone age is a couple of years older or younger. Those with advanced bone ages typically hit a growth spurt early on but stop growing sooner, while those with delayed bone ages hit their growth spurt later than normal. Children who are below average height do not necessarily have a delayed bone age; in fact their bone age could actually be advanced which if left untreated, will stunt their growth.

Endochondral ossification is one of the two essential processes during fetal development of the mammalian skeletal system by which bone tissue is created. Unlike intramembranous ossification, which is the other process by which bone tissue is created, cartilage is present during endochondral ossification. Endochondral ossification is also an essential process during the rudimentary formation of long bones, the growth of the length of long bones, and the natural healing of bone fractures.
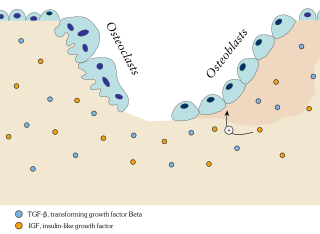
Ossification in bone remodeling is the process of laying down new bone material by cells named osteoblasts. It is synonymous with bone tissue formation. There are two processes resulting in the formation of normal, healthy bone tissue: Intramembranous ossification is the direct laying down of bone into the primitive connective tissue (mesenchyme), while endochondral ossification involves cartilage as a precursor.

Bone grafting is a surgical procedure that replaces missing bone in order to repair bone fractures that are extremely complex, pose a significant health risk to the patient, or fail to heal properly. Some small or acute fractures can be cured without bone grafting, but the risk is greater for large fractures like compound fractures.

Myositis ossificans comprises two syndromes characterized by heterotopic ossification (calcification) of muscle. The World Health Organization, 2020, has grouped myositis ossificans together with fibro-osseous pseudotumor of digits as a single specific entity in the category of fibroblastic and myofibroblastic tumors.

A back brace is a device designed to limit the motion of the spine in cases of bone fracture or in post-operative spinal fusiona, as well as a preventative measure against some progressive conditions or to correct patient posture.

Osteochondritis dissecans is a joint disorder primarily of the subchondral bone in which cracks form in the articular cartilage and the underlying subchondral bone. OCD usually causes pain during and after sports. In later stages of the disorder there will be swelling of the affected joint which catches and locks during movement. Physical examination in the early stages does only show pain as symptom, in later stages there could be an effusion, tenderness, and a crackling sound with joint movement.

The ischium forms the lower and back region of the hip bone.

The epiphyseal plate is a hyaline cartilage plate in the metaphysis at each end of a long bone. It is the part of a long bone where new bone growth takes place; that is, the whole bone is alive, with maintenance remodeling throughout its existing bone tissue, but the growth plate is the place where the long bone grows longer.

A Salter–Harris fracture is a fracture that involves the epiphyseal plate or growth plate of a bone, specifically the zone of provisional calcification. It is thus a form of child bone fracture. It is a common injury found in children, occurring in 15% of childhood long bone fractures. This type of fracture and its classification system is named for Robert B. Salter and William H. Harris who created and published this classification system in the Journal of Bone and Joint Surgery in 1963.

Chondroblastoma is a rare, benign, locally aggressive bone tumor that typically affects the epiphyses or apophyses of long bones. It is thought to arise from an outgrowth of immature cartilage cells (chondroblasts) from secondary ossification centers, originating from the epiphyseal plate or some remnant of it.

Ignacio Ponseti was a Spanish-American physician, specializing in orthopedics. He was born on 3 June 1914 in Menorca, part of the Balearic Islands, Spain, Ponseti was the son of a watchmaker and spent his childhood helping repair watches. This skill was said to eventually contribute to his abilities as an orthopedist. He served three years as a medic during the Spanish Civil War treating orthopedic injuries of wounded soldiers. He left Spain shortly after the end of the war and became a faculty member and practicing physician at the University of Iowa, where he developed his ground-breaking, non-surgical treatment for the clubfoot defect - the Ponseti Method.

Diffuse idiopathic skeletal hyperostosis (DISH) is a condition characterized by abnormal calcification/bone formation (hyperostosis) of the soft tissues surrounding the joints of the spine, and also of the peripheral or appendicular skeleton. In the spine, there is bone formation along the anterior longitudinal ligament and sometimes the posterior longitudinal ligament, which may lead to partial or complete fusion of adjacent vertebrae. The facet and sacroiliac joints tend to be uninvolved. The thoracic spine is the most common level involved. In the peripheral skeleton, DISH manifests as a calcific enthesopathy, with pathologic bone formation at sites where ligaments and tendons attach to bone.

The neuromechanics of idiopathic scoliosis is about the changes in the bones, muscles and joints in cases of spinal deformity consisting of a lateral curvature scoliosis and a rotation of the vertebrae within the curve, that is not explained by either congenital vertebral abnormalities, or neuromuscular disorders such as muscular dystrophy. The idiopathic scoliosis accounts for 80–90% of scoliosis cases. Its pathogenesis is unknown. However, changes in the vestibular system, a lateral shift of the hand representation and abnormal variability of erector spinae motor map location in the motor cortex may be involved in this disease. A short spinal cord and associated nerve tensions has been proposed as a cause and model for idiopathic scoliosis. Besides idiopathic scoliosis being more frequent in certain families, it is suspected to be transmitted via autosomal dominant inheritance. Estrogens could also play a crucial part in the progression of idiopathic scoliosis through their roles in bone formation, growth, maturation and turnover. Finally, collagen, intervertebral disc and muscle abnormalities have been suggested as the cause in idiopathic scoliosis, although these are perhaps results rather than causes.
Fibrocartilaginous mesenchymoma of bone is (FCMB) is an extremely rare tumor first described in 1984. About 26 cases have been reported in literature, with patient ages spanning from 9 to 25 years, though a case in a male infant aged 1 year and 7 months has been reported. Quick growth and bulky size are remarkable features of this tumor.
The management of scoliosis is complex and is determined primarily by the type of scoliosis encountered: syndromic, congenital, neuromuscular, or idiopathic. Treatment options for idiopathic scoliosis are determined in part by the severity of the curvature and skeletal maturity, which together help predict the likelihood of progression. Non-surgical treatment should be pro-active with intervention performed early as "Best results were obtained in 10-25 degrees scoliosis which is a good indication to start therapy before more structural changes within the spine establish." Treatment options have historically been categorized under the following types:
- Observation
- Bracing
- Specialized physical therapy
- Surgery

Ossification of the posterior longitudinal ligament (OPLL) is a process of fibrosis, calcification, and ossification of the posterior longitudinal ligament of the spine, that may involve the spinal dura. Once considered a disorder unique to people of Asian heritage, it is now recognized as an uncommon disorder in a variety of patients with myelopathy.
Anterior vertebral body tethering (AVBT) is a relatively new surgery for the treatment of scoliosis in pediatric patients. Left untreated, severe scoliosis can worsen and eventually affect a person's lungs and heart.

