Related Research Articles

A motor neuron is a neuron whose cell body is located in the motor cortex, brainstem or the spinal cord, and whose axon (fiber) projects to the spinal cord or outside of the spinal cord to directly or indirectly control effector organs, mainly muscles and glands. There are two types of motor neuron – upper motor neurons and lower motor neurons. Axons from upper motor neurons synapse onto interneurons in the spinal cord and occasionally directly onto lower motor neurons. The axons from the lower motor neurons are efferent nerve fibers that carry signals from the spinal cord to the effectors. Types of lower motor neurons are alpha motor neurons, beta motor neurons, and gamma motor neurons.

The autonomic nervous system (ANS), formerly referred to as the vegetative nervous system, is a division of the nervous system that operates internal organs, smooth muscle and glands. The autonomic nervous system is a control system that acts largely unconsciously and regulates bodily functions, such as the heart rate, its force of contraction, digestion, respiratory rate, pupillary response, urination, and sexual arousal. This system is the primary mechanism in control of the fight-or-flight response.
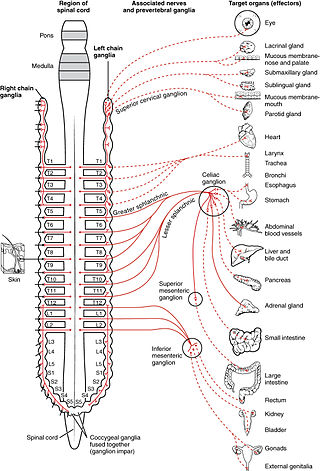
The sympathetic nervous system (SNS) is one of the three divisions of the autonomic nervous system, the others being the parasympathetic nervous system and the enteric nervous system. The enteric nervous system is sometimes considered part of the autonomic nervous system, and sometimes considered an independent system.

The somatic nervous system (SNS), or voluntary nervous system is the part of the peripheral nervous system associated with the voluntary control of body movements via skeletal muscles.

Muscle spindles are stretch receptors within the body of a skeletal muscle that primarily detect changes in the length of the muscle. They convey length information to the central nervous system via afferent nerve fibers. This information can be processed by the brain as proprioception. The responses of muscle spindles to changes in length also play an important role in regulating the contraction of muscles, for example, by activating motor neurons via the stretch reflex to resist muscle stretch.

A reflex arc is a neural pathway that controls a reflex. In vertebrates, most sensory neurons do not pass directly into the brain, but synapse in the spinal cord. This allows for faster reflex actions to occur by activating spinal motor neurons without the delay of routing signals through the brain. The brain will receive the input while the reflex is being carried out and the analysis of the signal takes place after the reflex action.

The patellar reflex, also called the knee reflex or knee-jerk, is a stretch reflex which tests the L2, L3, and L4 segments of the spinal cord. Many animals, most significantly humans, have been seen to have the patellar reflex, including dogs, cats, horses, and other mammalian species.
The withdrawal reflex is a spinal reflex intended to protect the body from damaging stimuli. The reflex rapidly coordinates the contractions of all the flexor muscles and the relaxations of the extensors in that limb causing sudden withdrawal from the potentially damaging stimulus. Spinal reflexes are often monosynaptic and are mediated by a simple reflex arc. A withdrawal reflex is mediated by a polysynaptic reflex resulting in the stimulation of many motor neurons in order to give a quick response.

Neurogenic shock is a distributive type of shock resulting in hypotension, often with bradycardia, caused by disruption of autonomic nervous system pathways. It can occur after damage to the central nervous system, such as spinal cord injury and traumatic brain injury. Low blood pressure occurs due to decreased systemic vascular resistance resulting from loss of sympathetic tone, which in turn causes blood pooling within the extremities rather than being available to circulate throughout the body. The slowed heart rate results from a vagal response unopposed by a sympathetic nervous system (SNS) response. Such cardiovascular instability is exacerbated by hypoxia, or treatment with endotracheal or endobronchial suction used to prevent pulmonary aspiration.

Upper motor neurons (UMNs) is a term introduced by William Gowers in 1886. They are found in the cerebral cortex and brainstem and carry information down to activate interneurons and lower motor neurons, which in turn directly signal muscles to contract or relax. UMNs represent the major origin point for voluntary somatic movement.

The stretch reflex, or more accurately "muscle stretch reflex", is a muscle contraction in response to stretching a muscle. The function of the reflex is generally thought be maintaining the muscle at a constant length but the response is often coordinated across multiple muscles and even joints. The term deep tendon reflex is often wrongfully used by many health workers and students to refer to this reflex. "Tendons have little to do with the response, other than being responsible for mechanically transmitting the sudden stretch from the reflex hammer to the muscle spindle. In addition, some muscles with stretch reflexes have no tendons ".
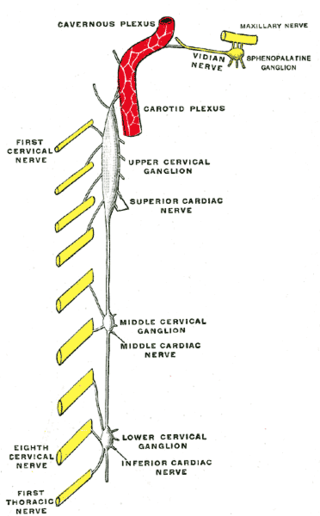
The superior cervical ganglion (SCG) is the upper-most and largest of the cervical sympathetic ganglia of the sympathetic trunk. It probably formed by the union of four sympathetic ganglia of the cervical spinal nerves C1–C4. It is the only ganglion of the sympathetic nervous system that innervates the head and neck. The SCG innervates numerous structures of the head and neck.
Autonomic dysreflexia (AD) is a potentially fatal medical emergency classically characterized by uncontrolled hypertension and cardiac arrhythmia. AD occurs most often in individuals with spinal cord injuries with lesions at or above the T6 spinal cord level, although it has been reported in patients with lesions as low as T10. Guillain–Barré syndrome may also cause autonomic dysreflexia.
Alpha (α) motor neurons (also called alpha motoneurons), are large, multipolar lower motor neurons of the brainstem and spinal cord. They innervate extrafusal muscle fibers of skeletal muscle and are directly responsible for initiating their contraction. Alpha motor neurons are distinct from gamma motor neurons, which innervate intrafusal muscle fibers of muscle spindles.
Hyporeflexia is the reduction or absence of normal bodily reflexes (areflexia). It can be detected through the use of a reflex hammer and is the opposite of hyperreflexia.

The axon reflex is the response stimulated by peripheral nerves of the body that travels away from the nerve cell body and branches to stimulate target organs. Reflexes are single reactions that respond to a stimulus making up the building blocks of the overall signaling in the body's nervous system. Neurons are the excitable cells that process and transmit these reflex signals through their axons, dendrites, and cell bodies. Axons directly facilitate intercellular communication projecting from the neuronal cell body to other neurons, local muscle tissue, glands and arterioles. In the axon reflex, signaling starts in the middle of the axon at the stimulation site and transmits signals directly to the effector organ skipping both an integration center and a chemical synapse present in the spinal cord reflex. The impulse is limited to a single bifurcated axon, or a neuron whose axon branches into two divisions and does not cause a general response to surrounding tissue.
The Golgi tendon reflex (also called inverse stretch reflex, autogenic inhibition, tendon reflex) is an inhibitory effect on the muscle resulting from the muscle tension stimulating Golgi tendon organs (GTO) of the muscle, and hence it is self-induced. The reflex arc is a negative feedback mechanism preventing too much tension on the muscle and tendon. When the tension is extreme, the inhibition can be so great it overcomes the excitatory effects on the muscle's alpha motoneurons causing the muscle to suddenly relax. This reflex is also called the inverse myotatic reflex, because it is the inverse of the stretch reflex.

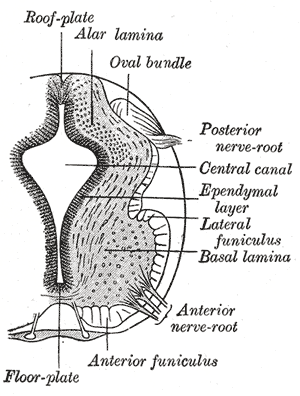
A spinal interneuron, found in the spinal cord, relays signals between (afferent) sensory neurons, and (efferent) motor neurons. Different classes of spinal interneurons are involved in the process of sensory-motor integration. Most interneurons are found in the grey column, a region of grey matter in the spinal cord.

Cutaneous, superficial, or skin reflexes, are activated by skin receptors and play a valuable role in locomotion, providing quick responses to unexpected environmental challenges. They have been shown to be important in responses to obstacles or stumbling, in preparing for visually challenging terrain, and for assistance in making adjustments when instability is introduced. In addition to the role in normal locomotion, cutaneous reflexes are being studied for their potential in enhancing rehabilitation therapy (physiotherapy) for people with gait abnormalities.

Neurogenic bowel dysfunction (NBD) is the inability to control defecation due to a deterioration of or injury to the nervous system, resulting in faecal incontinence or constipation. It is common in people with spinal cord injury (SCI), multiple sclerosis (MS) or spina bifida.
References
- ↑ Atkinson, Patty Pate; Atkinson, John L.D. (April 1996). "Spinal Shock". Mayo Clinic Proceedings. 71 (4): 384–389. doi:10.4065/71.4.384 . Retrieved 3 August 2020.
- ↑ Ditunno, JF; Little, JW; Tessler, A; Burns, AS (1 July 2004). "Spinal shock revisited: a four-phase model". Spinal Cord. 42 (7): 383–95. doi: 10.1038/sj.sc.3101603 . PMID 15037862.
- ↑ B. SCHURCH; P.A. KNAPP; D. JEANMONOD; B. RODIC; A.B. ROSSIER (2010). "Case Study: 10 patients with SCI, traumatic spinal cord injury". The Medical Journal of Urology. Archived from the original on 28 August 2010. Retrieved April 20, 2010.