Related Research Articles
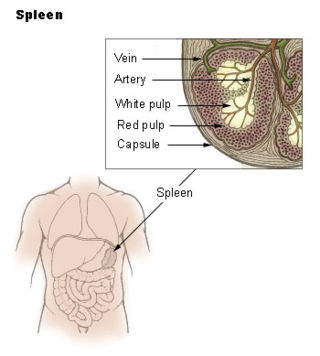
The spleen is an organ found in almost all vertebrates. Similar in structure to a large lymph node, it acts primarily as a blood filter. The word spleen comes from Ancient Greek σπλήν (splḗn).

Waterhouse–Friderichsen syndrome (WFS) is defined as adrenal gland failure due to bleeding into the adrenal glands, commonly caused by severe bacterial infection. Typically, it is caused by Neisseria meningitidis.

Charles Louis Alphonse Laveran was a French physician who won the Nobel Prize in Physiology or Medicine in 1907 for his discoveries of parasitic protozoans as causative agents of infectious diseases such as malaria and trypanosomiasis. Following his father, Louis Théodore Laveran, he took up military medicine as his profession. He obtained his medical degree from University of Strasbourg in 1867.
Asplenia refers to the absence of normal spleen function and is associated with some serious infection risks. Hyposplenism is used to describe reduced ('hypo-') splenic functioning, but not as severely affected as with asplenism.
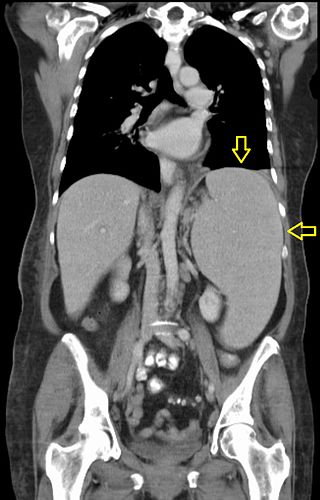
Splenomegaly is an enlargement of the spleen. The spleen usually lies in the left upper quadrant (LUQ) of the human abdomen. Splenomegaly is one of the four cardinal signs of hypersplenism which include: some reduction in number of circulating blood cells affecting granulocytes, erythrocytes or platelets in any combination; a compensatory proliferative response in the bone marrow; and the potential for correction of these abnormalities by splenectomy. Splenomegaly is usually associated with increased workload, which suggests that it is a response to hyperfunction. It is therefore not surprising that splenomegaly is associated with any disease process that involves abnormal red blood cells being destroyed in the spleen. Other common causes include congestion due to portal hypertension and infiltration by leukemias and lymphomas. Thus, the finding of an enlarged spleen, along with caput medusae, is an important sign of portal hypertension.
Hepatosplenomegaly is the simultaneous enlargement of both the liver (hepatomegaly) and the spleen (splenomegaly). Hepatosplenomegaly can occur as the result of acute viral hepatitis, infectious mononucleosis, and histoplasmosis or it can be the sign of a serious and life-threatening lysosomal storage disease. Systemic venous hypertension can also increase the risk for developing hepatosplenomegaly, which may be seen in those patients with right-sided heart failure.
Primary myelofibrosis (PMF) is a rare bone marrow blood cancer. It is classified by the World Health Organization (WHO) as a type of myeloproliferative neoplasm, a group of cancers in which there is activation and growth of mutated cells in the bone marrow. This is most often associated with a somatic mutation in the JAK2, CALR, or MPL genes. In PMF, the bony aspects of bone marrow are remodeled in a process called osteosclerosis; in addition, fibroblast secrete collagen and reticulin proteins that are collectively referred to as (fibrosis). These two pathological processes compromise the normal function of bone marrow resulting in decreased production of blood cells such as erythrocytes, granulocytes and megakaryocytes, the latter cells responsible for the production of platelets.
Pancytopenia is a medical condition in which there is significant reduction in the number of almost all blood cells.

A hamartoma is a mostly benign, local malformation of cells that resembles a neoplasm of local tissue but is usually due to an overgrowth of multiple aberrant cells, with a basis in a systemic genetic condition, rather than a growth descended from a single mutated cell (monoclonality), as would typically define a benign neoplasm/tumor. Despite this, many hamartomas are found to have clonal chromosomal aberrations that are acquired through somatic mutations, and on this basis the term hamartoma is sometimes considered synonymous with neoplasm. Hamartomas are by definition benign, slow-growing or self-limiting, though the underlying condition may still predispose the individual towards malignancies.
Aplasia is a birth defect where an organ or tissue is wholly or largely absent. It is caused by a defect in a developmental process.

Castell's sign is a medical sign assessed to evaluate splenomegaly and typically part of an abdominal examination. It is an alternative physical examination maneuver to percussion over Traube's space.
Fever of unknown origin (FUO) refers to a condition in which the patient has an elevated temperature (fever) but, despite investigations by one or more qualified physicians, no explanation is found.
Felty's syndrome (FS), also called Felty syndrome, is a rare autoimmune disease characterized by the triad of rheumatoid arthritis, enlargement of the spleen and low neutrophil count. The condition is more common in those aged 50–70 years, specifically more prevalent in females than males, and more so in Caucasians than those of African descent. It is a deforming disease that causes many complications for the individual.

Splenic infarction is a condition in which blood flow supply to the spleen is compromised, leading to partial or complete infarction in the organ. Splenic infarction occurs when the splenic artery or one of its branches are occluded, for example by a blood clot.
Juvenile myelomonocytic leukemia (JMML) is a rare form of chronic leukemia that affects children, commonly those aged four and younger. The name JMML now encompasses all diagnoses formerly referred to as juvenile chronic myeloid leukemia (JCML), chronic myelomonocytic leukemia of infancy, and infantile monosomy 7 syndrome. The average age of patients at diagnosis is two (2) years old. The World Health Organization has included JMML as a subcategory of myelodysplastic and myeloproliferative disorders.
Serum sickness in humans is a reaction to proteins in antiserum derived from a non-human animal source, occurring 5–10 days after exposure. Symptoms often include a rash, joint pain, fever, and lymphadenopathy. It is a type of hypersensitivity, specifically immune complex hypersensitivity. The term serum sickness–like reaction (SSLR) is occasionally used to refer to similar illnesses that arise from the introduction of certain non-protein substances, such as penicillin.

Hemoglobin E (HbE) is an abnormal hemoglobin with a single point mutation in the β chain. At position 26 there is a change in the amino acid, from glutamic acid to lysine (E26K). Hemoglobin E is very common among people of Southeast Asian, Northeast Indian, Sri Lankan and Bangladeshi descent.
Congenital hemolytic anemia (CHA) is a diverse group of rare hereditary conditions marked by decreased life expectancy and premature removal of erythrocytes from blood flow. Defects in erythrocyte membrane proteins and red cell enzyme metabolism, as well as changes at the level of erythrocyte precursors, lead to impaired bone marrow erythropoiesis. CAH is distinguished by variable anemia, chronic extravascular hemolysis, decreased erythrocyte life span, splenomegaly, jaundice, biliary lithiasis, and iron overload. Immune-mediated mechanisms may play a role in the pathogenesis of these uncommon diseases, despite the paucity of data regarding the immune system's involvement in CHAs.
Tropical pulmonary eosinophilia, is characterized by cough, bronchospasm, wheezing, abdominal pain, and an enlarged spleen. Occurring most frequently in the Indian subcontinent and Southeast Asia, TPE is a clinical manifestation of lymphatic filariasis, a parasitic infection caused by filarial roundworms that inhabit the lymphatic vessels, lymph nodes, spleen, and bloodstream. Three species of filarial roundworms, all from the Onchocercidae family, cause human lymphatic filariasis: Wuchereria bancrofti, Brugia malayi, and Brugia timori.
Cold autoimmune hemolytic anemia caused by cold-reacting antibodies. Autoantibodies that bind to the erythrocyte membrane leading to premature erythrocyte destruction (hemolysis) characterize autoimmune hemolytic anemia.
References
- Greenwood B, Fakunle Y. The tropical splenomegaly syndrome. In: The role of the spleen in the immunology of parasitic disease. Basel: Schwabe, 1979: 229–251.
- Fakunle Y. Tropical splenomegaly. In: Luzzatto L, ed. Clinics in haematology. London: WB Saunders, 1981: 963–975.
- Neelam Raval, Neela Shah and S. N. Vani: Tropical splenomegaly syndrome, Indian Journal of Pediatrics, Volume 58, Number 5, 679–681, doi : 10.1007/BF02820190
| | This article about a disease, disorder, or medical condition is a stub. You can help Wikipedia by expanding it. |