Related Research Articles

Pott's disease, or Pott disease, named for British surgeon Percivall Pott who first described the symptoms in 1799, is tuberculosis of the spine, usually due to haematogenous spread from other sites, often the lungs. The lower thoracic and upper lumbar vertebrae areas of the spine are most often affected.

A laminectomy is a surgical procedure that removes a portion of a vertebra called the lamina, which is the roof of the spinal canal. It is a major spine operation with residual scar tissue and may result in postlaminectomy syndrome. Depending on the problem, more conservative treatments may be viable.

In human anatomy, the spinal canal, vertebral canal or spinal cavity is an elongated body cavity enclosed within the dorsal bony arches of the vertebral column, which contains the spinal cord, spinal roots and dorsal root ganglia. It is a process of the dorsal body cavity formed by alignment of the vertebral foramina. Under the vertebral arches, the spinal canal is also covered anteriorly by the posterior longitudinal ligament and posteriorly by the ligamentum flavum. The potential space between these ligaments and the dura mater covering the spinal cord is known as the epidural space. Spinal nerves exit the spinal canal via the intervertebral foramina under the corresponding vertebral pedicles.

Spondylosis is the degeneration of the vertebral column from any cause. In the more narrow sense it refers to spinal osteoarthritis, the age-related degeneration of the spinal column, which is the most common cause of spondylosis. The degenerative process in osteoarthritis chiefly affects the vertebral bodies, the neural foramina and the facet joints. If severe, it may cause pressure on the spinal cord or nerve roots with subsequent sensory or motor disturbances, such as pain, paresthesia, imbalance, and muscle weakness in the limbs.

Degenerative disc disease (DDD) is a medical condition typically brought on by the aging process in which there are anatomic changes and possibly a loss of function of one or more intervertebral discs of the spine. DDD can take place with or without symptoms, but is typically identified once symptoms arise. The root cause is thought to be loss of soluble proteins within the fluid contained in the disc with resultant reduction of the oncotic pressure, which in turn causes loss of fluid volume. Normal downward forces cause the affected disc to lose height, and the distance between vertebrae is reduced. The anulus fibrosus, the tough outer layers of a disc, also weakens. This loss of height causes laxity of the longitudinal ligaments, which may allow anterior, posterior, or lateral shifting of the vertebral bodies, causing facet joint malalignment and arthritis; scoliosis; cervical hyperlordosis; thoracic hyperkyphosis; lumbar hyperlordosis; narrowing of the space available for the spinal tract within the vertebra ; or narrowing of the space through which a spinal nerve exits with resultant inflammation and impingement of a spinal nerve, causing a radiculopathy.

Cauda equina syndrome (CES) is a condition that occurs when the bundle of nerves below the end of the spinal cord known as the cauda equina is damaged. Signs and symptoms include low back pain, pain that radiates down the leg, numbness around the anus, and loss of bowel or bladder control. Onset may be rapid or gradual.

Spinal fusion, also called spondylodesis or spondylosyndesis, is a surgery performed by orthopaedic surgeons or neurosurgeons that joins two or more vertebrae. This procedure can be performed at any level in the spine and prevents any movement between the fused vertebrae. There are many types of spinal fusion and each technique involves using bone grafting—either from the patient (autograft), donor (allograft), or artificial bone substitutes—to help the bones heal together. Additional hardware is often used to hold the bones in place while the graft fuses the two vertebrae together. The placement of hardware can be guided by fluoroscopy, navigation systems, or robotics.

The anterior longitudinal ligament is a ligament that extends across the anterior/ventral aspect of the vertebral bodies and intervertebral discs the spine.
Congenital vertebral anomalies are a collection of malformations of the spine. Most, around 85%, are not clinically significant, but they can cause compression of the spinal cord by deforming the vertebral canal or causing instability. This condition occurs in the womb. Congenital vertebral anomalies include alterations of the shape and number of vertebrae.
Wobbler disease is a catchall term referring to several possible malformations of the cervical vertebrae that cause an unsteady (wobbly) gait and weakness in dogs and horses. A number of different conditions of the cervical (neck) spinal column cause similar clinical signs. These conditions may include malformation of the vertebrae, intervertebral disc protrusion, and disease of the interspinal ligaments, ligamenta flava, and articular facets of the vertebrae. Wobbler disease is also known as cervical vertebral instability (CVI), cervical spondylomyelopathy (CSM), and cervical vertebral malformation (CVM). In dogs, the disease is most common in large breeds, especially Great Danes and Doberman Pinschers. In horses, it is not linked to a particular breed, though it is most often seen in tall, race-bred horses of Thoroughbred or Standardbred ancestry. It is most likely inherited to at least some extent in dogs and horses.

A spinal disc herniation is an injury to the intervertebral disc between two spinal vertebrae, usually caused by excessive strain or trauma to the spine. It may result in back pain, pain or sensation in different parts of the body, and physical disability. The most conclusive diagnostic tool for disc herniation is MRI, and treatments may range from painkillers to surgery. Protection from disc herniation is best provided by core strength and an awareness of body mechanics including good posture.

Anterior cervical discectomy and fusion (ACDF) is a surgical procedure to treat nerve root or spinal cord compression by decompressing the spinal cord and nerve roots of the cervical spine with a discectomy, followed by inter-vertebral fusion to stabilize the corresponding vertebrae. This procedure is used when other non-surgical treatments have failed.

A laminotomy is an orthopaedic neurosurgical procedure that removes part of the lamina of a vertebral arch in order to relieve pressure in the vertebral canal. A laminotomy is less invasive than conventional vertebral column surgery techniques, such as laminectomy because it leaves more ligaments and muscles attached to the spinous process intact and it requires removing less bone from the vertebra. As a result, laminotomies typically have a faster recovery time and result in fewer postoperative complications. Nevertheless, possible risks can occur during or after the procedure like infection, hematomas, and dural tears. Laminotomies are commonly performed as treatment for lumbar spinal stenosis and herniated disks. MRI and CT scans are often used pre- and post surgery to determine if the procedure was successful.

Laminoplasty is an orthopaedic/neurosurgical surgical procedure for treating spinal stenosis by relieving pressure on the spinal cord. The main purpose of this procedure is to provide relief to patients who may have symptoms of numbness, pain, or weakness in arm movement. The procedure involves cutting the lamina on both sides of the affected vertebrae and then "swinging" the freed flap of bone open thus relieving the pressure on the spinal cord. The spinous process may be removed to allow the lamina bone flap to be swung open. The bone flap is then propped open using small wedges or pieces of bone such that the enlarged spinal canal will remain in place.
The spinal cord is a long, thin, tubular structure made up of nervous tissue that extends from the medulla oblongata in the lower brainstem to the lumbar region of the vertebral column (backbone) of vertebrate animals. The center of the spinal cord is hollow and contains a structure called the central canal, which contains cerebrospinal fluid. The spinal cord is also covered by meninges and enclosed by the neural arches. Together, the brain and spinal cord make up the central nervous system.

Spinal stenosis is an abnormal narrowing of the spinal canal or neural foramen that results in pressure on the spinal cord or nerve roots. Symptoms may include pain, numbness, or weakness in the arms or legs. Symptoms are typically gradual in onset and improve with leaning forward. Severe symptoms may include loss of bladder control, loss of bowel control, or sexual dysfunction.

The vertebral column, also known as the spinal column, spine or backbone, is the core part of the axial skeleton in vertebrate animals. The vertebral column is the defining and eponymous characteristic of the vertebrate endoskeleton, where the notochord found in all chordates has been replaced by a segmented series of mineralized irregular bones called vertebrae, separated by fibrocartilaginous intervertebral discs. The dorsal portion of the vertebral column houses the spinal canal, an elongated cavity formed by alignment of the vertebral neural arches that encloses and protects the spinal cord, with spinal nerves exiting via the intervertebral foramina to innervate each body segments.
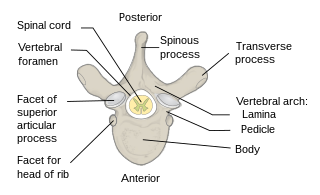
Each vertebra is an irregular bone with a complex structure composed of bone and some hyaline cartilage, that make up the vertebral column or spine, of vertebrates. The proportions of the vertebrae differ according to their spinal segment and the particular species.

Cervicocranial syndrome or is a combination of symptoms that are caused by an abnormality in the cervical vertebrae leading to improper function of cervical spinal nerves. Cervicocranial syndrome is either congenital or acquired. Some examples of diseases that could result in cervicocranial syndrome are Chiari disease, Klippel-Feil malformation osteoarthritis, and trauma. Treatment options include neck braces, pain medication and surgery. The quality of life for individuals suffering from CCJ syndrome can improve through surgery.
Cervical Spondylotic Myelopathy (CSM) is a disorder characterised by the age-related deterioration of the cervical spinal cord. Referred to be a range of different but related terms, a global consensus process selected Degenerative Cervical Myelopathy as the new overarching disease term. It is a neurological disorder related to the spinal cord and nerve roots. The severity of CSM is most commonly associated with factors including age, location and extent of spinal cord compression.
References
- 1 2 3 4 Davis, Emily; Vite, Charles H. (2015). "Spinal Cord Injury". Small Animal Critical Care Medicine. pp. 431–436. doi:10.1016/B978-1-4557-0306-7.00083-0. ISBN 978-1-4557-0306-7.
- 1 2 Vialle, Luiz Roberto; Riew, K. Daniel; Ito, Manabu, eds. (2015). "2 Anterior Cervical Decompression and Fusion Techniques: Anterior Cervical Decompression and Fusion, Corpectomy, and Foraminotomy". AOSpine Masters Series Volume 3: Cervical Degenerative Conditions. doi:10.1055/b-0035-120937. ISBN 978-1-62623-050-7.
- 1 2 Voss, K. (2009). "The spine". Feline Orthopedic Surgery and Musculoskeletal Disease. pp. 407–422. doi:10.1016/B978-070202986-8.00046-X. ISBN 978-070202986-8.
- 1 2 "Intervertebral Disk Disease". cal.vet.upenn.edu. Retrieved 2019-12-02.
- ↑ Cloward, Ralph B. (November 1958). "The Anterior Approach for Removal of Ruptured Cervical Disks". Journal of Neurosurgery. 15 (6): 602–617. doi:10.3171/jns.1958.15.6.0602. PMID 13599052.
- ↑ "Experimental meningococcus meningitis. C. P. Austrian, bull. Johns Hopkins hosp., Aug., 1918". The Laryngoscope. 29 (4): 254–255. April 1919. doi:10.1288/00005537-191904000-00069.
- ↑ Robinson, Robert A. (January 1959). "Fusions of the Cervical Spine". The Journal of Bone & Joint Surgery. 41 (1): 1–6. doi:10.2106/00004623-195941010-00001. PMID 13620682.
- 1 2 Voss, K. (2009). "The spine". Feline Orthopedic Surgery and Musculoskeletal Disease. pp. 407–422. doi:10.1016/B978-070202986-8.00046-X. ISBN 978-070202986-8.
- ↑ Watkins, Robert G. (2003). "Lateral Approach to the Cervical Spine (Verbiest)". Surgical Approaches to the Spine. pp. 54–59. doi:10.1007/978-1-4613-0009-0_8. ISBN 978-1-4612-6508-5.
- 1 2 Johnson, Kenneth A. (2014). "The Vertebral Column". Piermattei's Atlas of Surgical Approaches to the Bones and Joints of the Dog and Cat. pp. 47–115. doi:10.1016/B978-1-4377-1634-4.00003-4. ISBN 978-1-4377-1634-4.
- ↑ Voss, K. (2009). "Preparation for surgery". Feline Orthopedic Surgery and Musculoskeletal Disease. pp. 207–211. doi:10.1016/b978-070202986-8.00029-x. ISBN 978-0-7020-2986-8.
- ↑ Bhangoo, Ranjeev Singh; Crockard, H. Alan (2003). "Ventral Approaches to the Clivus, C1, and C2". Surgical Approaches to the Spine. pp. 19–33. doi:10.1007/978-1-4613-0009-0_4. ISBN 978-1-4612-6508-5.
- ↑ Dyck, Peter (2003). "Cervical Foraminotomy: Indications and Technique". Surgical Approaches to the Spine. pp. 237–244. doi:10.1007/978-1-4613-0009-0_32. ISBN 978-1-4612-6508-5.
- ↑ "Discopathie | Tierklinik am Kaiserberg". Tierklinik Kaiserberg. Retrieved 2019-12-02.