Traumatic brain injury (TBI, physical trauma to the brain) can cause a variety of complications, health effects that are not TBI themselves but that result from it. The risk of complications increases with the severity of the trauma;[1] however even mild traumatic brain injury can result in disabilities that interfere with social interactions, employment, and everyday living.[2] TBI can cause a variety of problems including physical, cognitive, emotional, and behavioral complications.
Stupor is a state of partial or near complete unconsciousness in which the patient is lethargic, immobile, and has a reduced response to stimuli.[3]
Coma is a state in which the patient is totally unconscious and cannot be aroused even with strong stimuli.[4]
Persistent vegetative state is a condition in which awake patients are unconscious and unaware of their surroundings and the cerebral cortex is not functioning.[5] A vegetative state can result from diffuse injury to the cerebral hemispheres of the brain without damage to the lower brain and brainstem. The vegetative state is considered permanent if it persists for 12 months after TBI or 3 months after causes other than trauma.[6]
A minimally conscious state is a condition in which patients have a reduced level of arousal and may appear, on the surface, to be in a persistent vegetative state but are capable of demonstrating the ability to actively process information.
Locked-in syndrome is a condition in which a patient is aware and awake, but cannot move or communicate due to complete paralysis of the body.[7] Voluntary control of eye movements or blinking may be spared, permitting the detection of conscious awareness and enabling the establishment of functional communication.[7]
Brain death is the irreversible loss of measurable brain function, with loss of any integrated activity among distinct areas of the brain.[8] Breathing and heart function must be maintained with assistive devices.[8]
Disorders of consciousness affect a significant number of people with severe TBI; of those with severe TBI discharged from a hospital, 10%-15% are in a vegetative state, and of this number only half regain consciousness within one to three years.[6]
Most patients with severe TBI who recover consciousness experience cognitive disabilities, including the loss of many higher-level mental skills. Cognitive deficits that can follow TBI include impaired attention; disrupted insight, judgement, and thought; reduced processing speed; distractibility; and deficits in executive functions such as abstract reasoning, planning, problem-solving, and multitasking.[9]Memory loss, the most common cognitive impairment among head-injured people, occurs in 20–79% of people with closed head trauma, depending on severity.[10]Post-traumatic amnesia (PTA), a confusional state with impaired memory,[11] is characterized by loss of specific memories or the partial inability to form or store new ones.[12]
Alzheimer's disease (AD) is a progressive, neurodegenerative disease characterized by dementia, memory loss, and deteriorating cognitive abilities. Research suggests an association between head injury in early adulthood and the development of AD later in life; the more severe the head injury, the greater the risk of developing AD.[1] Some evidence indicates that a head injury may interact with other factors to trigger the disease and may hasten the onset of the disease in individuals already at risk. For example, head-injured people who have a particular form of the protein apolipoprotein E (apoE4, a naturally occurring protein that helps transport cholesterol through the bloodstream) fall into this increased risk category.[1]
Patients with moderate to severe TBI have more problems with cognitive deficits than do those with mild TBI, but several mild TBIs may have an additive effect. About one in five career boxers is affected by chronic traumatic brain injury (CTBI), which causes cognitive, behavioral, and physical impairments.[13]Dementia pugilistica, also called chronic traumatic encephalopathy, is the severe form of CTBI.[13] Caused by repetitive blows to the head over a long period, the condition primarily affects career boxers and has recently been linked to other contact sports including American football and ice hockey as well as military service(see Ann McKee). It commonly manifests as dementia, or declining mental ability, memory problems, and parkinsonism (tremors and lack of coordination).[14] Symptoms begin anywhere between 6 and 40years after the start of a boxing career, with an average onset of about 16 years.
Communication problems
Language and communication problems are common disabilities in TBI patients. Some may experience aphasia, difficulty with understanding and producing spoken and written language; or they may have difficulty with the more subtle aspects of communication, such as body language and emotional, non-verbal signals. Some may have problems with intonation or inflection, called prosodic dysfunction. Problems with spoken language may occur if the part of the brain that controls speech muscles is damaged. In this disorder, called dysarthria, the patient can think of the appropriate language, but cannot easily speak the words because they are unable to use the muscles needed to form the words and produce the sounds. Speech is often slow, slurred, and garbled.[1]
Sensory deficits
TBI patients may have sensory problems, especially problems with vision; they may not be able to register what they are seeing or may be slow to recognize objects. Also, TBI patients often have difficulty with hand–eye coordination, causing them to seem clumsy or unsteady. Other sensory deficits include problems with hearing, smell, taste, or touch. Tinnitus, a ringing or roaring in the ears, may occur. A person with damage to the part of the brain that processes taste or smell may perceive a persistent bitter taste or noxious smell. Damage to the part of the brain that controls the sense of touch may cause a TBI patient to develop persistent skin tingling, itching, or pain. These conditions are rare and difficult to treat.[1]
Behavioral symptoms that can follow TBI include disinhibition, inability to control anger, impulsiveness, lack of initiative, inappropriate sexual activity, and changes in personality.[9] Different behavioral problems are characteristic of the location of injury; for instance, frontal lobe injuries often result in disinhibition and inappropriate or childish behavior, and temporal lobe injuries often cause irritability and aggression.[19]
Physical complications
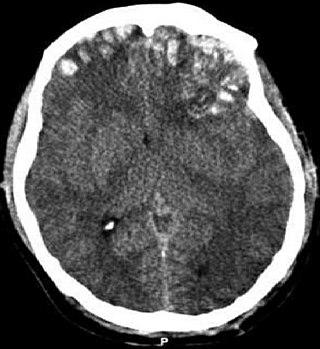
The relative risk of post-traumatic seizures increases with the severity of traumatic brain injury.
The risk of post-traumatic seizures increases with severity of trauma (image at right) and is particularly elevated with certain types of brain trauma such as cerebral contusions or hematomas.[22] As many as 50% of people with penetrating head injuries will develop seizures.[20] People with early seizures, those occurring within a week of injury, have an increased risk of post-traumatic epilepsy (recurrent seizures occurring more than a week after the initial trauma)[23] though seizures can appear a decade or more after the initial injury and the common seizure type may also change over time. Generally, medical professionals use anticonvulsant medications to treat seizures in TBI patients within the first week of injury only[24] and after that only if the seizures persist.
Coagulopathy after a TBI can appear, due to specific biochemical processes, which can in turn lead to further serious complications, such as progressive hemorrhagic injury.[25]
Neurostorms may occur after a severe TBI. The lower the Glasgow Coma Score (GCS), the higher the chance of Neurostorming. Neurostorms occur when the patient's Autonomic Nervous System (ANS), Central Nervous System (CNS), Sympathetic Nervous System (SNS), and Parasympathetic nervous system (PSNS) become severely compromised.[26] This in turn can create the following potential life-threatening symptoms: increased intra-cranial pressure (ICP), tachycardia, tremors, seizures, fevers, increased blood pressure, increased Cerebral Spinal Fluid (CSF), and diaphoresis.[26] A variety of medication may be used to help decrease or control neurostorm episodes.[27]
Parkinson's disease and other motor problems as a result of TBI are rare but can occur. Parkinson's disease, a chronic and progressive disorder, may develop years after TBI as a result of damage to the basal ganglia. Other movement disorders that may develop after TBI include tremor, ataxia (uncoordinated muscle movements), and myoclonus (shock-like contractions of muscles).[1]
Skull fractures can tear the meninges, the membranes that cover the brain, leading to cerebrospinal fluid leaks (CSF leaks). A tear between the dura and the arachnoid membranes, called a CSF fistula, can cause CSF to leak out of the subarachnoid space into the subdural space; this is called a subdural hygroma.[1] CSF can also leak from the nose and the ear. These tears can also allow bacteria into the cavity, potentially causing infections such as meningitis. Pneumocephalus occurs when air enters the intracranial cavity and becomes trapped in the subarachnoid space. Infections within the intracranial cavity are a dangerous complication of TBI. They may occur outside of the dura mater, below the dura, below the arachnoid (meningitis), or within the brain itself (abscess). Most of these injuries develop within a few weeks of the initial trauma and result from skull fractures or penetrating injuries. Standard treatment involves antibiotics and sometimes surgery to remove the infected tissue.[1]
Injuries to the base of the skull can damage nerves that emerge directly from the brain (cranial nerves). Cranial nerve damage may result in:
Hydrocephalus, post-traumatic ventricular enlargement, occurs when CSF accumulates in the brain, resulting in dilation of the cerebral ventricles and an increase in ICP. This condition can develop during the acute stage of TBI or may not appear until later. Generally it occurs within the first year of the injury and is characterized by worsening neurological outcome, impaired consciousness, behavioral changes, ataxia (lack of coordination or balance), incontinence, or signs of elevated ICP.[1]
Any damage to the head or brain usually results in some damage to the vascular system, which provides blood to the cells of the brain. The body can repair small blood vessels, but damage to larger ones can result in serious complications. Damage to one of the major arteries leading to the brain can cause a stroke, either through bleeding from the artery or through the formation of a blood clot at the site of injury, blocking blood flow to the brain. Blood clots also can develop in other parts of the head. Other types of vascular complications include vasospasm, in which blood vessels constrict and restrict blood flow, and the formation of aneurysms, in which the side of a blood vessel weakens and balloons out.[1]
A coma is a deep state of prolonged unconsciousness in which a person cannot be awakened, fails to respond normally to painful stimuli, light, or sound, lacks a normal wake-sleep cycle and does not initiate voluntary actions. The person may experience respiratory and circulatory problems due to the body's inability to maintain normal bodily functions. People in a coma often require extensive medical care to maintain their health and prevent complications such as pneumonia or blood clots. Coma patients exhibit a complete absence of wakefulness and are unable to consciously feel, speak or move. Comas can be derived by natural causes, or can be medically induced.
A head injury is any injury that results in trauma to the skull or brain. The terms traumatic brain injury and head injury are often used interchangeably in the medical literature. Because head injuries cover such a broad scope of injuries, there are many causes—including accidents, falls, physical assault, or traffic accidents—that can cause head injuries.
Neurotrauma, brain damage or brain injury (BI) is the destruction or degeneration of brain cells. Brain injuries occur due to a wide range of internal and external factors. In general, brain damage refers to significant, undiscriminating trauma-induced damage.
A concussion, also known as a mild traumatic brain injury (mTBI), is a head injury that temporarily affects brain functioning. Symptoms may include loss of consciousness; memory loss; headaches; difficulty with thinking, concentration, or balance; nausea; blurred vision; dizziness; sleep disturbances, and mood changes. Any of these symptoms may begin immediately, or appear days after the injury. Concussion should be suspected if a person indirectly or directly hits their head and experiences any of the symptoms of concussion. Symptoms of a concussion may be delayed by 1–2 days after the accident. It is not unusual for symptoms to last 2 weeks in adults and 4 weeks in children. Fewer than 10% of sports-related concussions among children are associated with loss of consciousness.
Intracranial pressure (ICP) is the pressure exerted by fluids such as cerebrospinal fluid (CSF) inside the skull and on the brain tissue. ICP is measured in millimeters of mercury (mmHg) and at rest, is normally 7–15 mmHg for a supine adult. The body has various mechanisms by which it keeps the ICP stable, with CSF pressures varying by about 1 mmHg in normal adults through shifts in production and absorption of CSF.
Intracranial hemorrhage (ICH), also known as intracranial bleed, is bleeding within the skull. Subtypes are intracerebral bleeds, subarachnoid bleeds, epidural bleeds, and subdural bleeds.
A traumatic brain injury (TBI), also known as an intracranial injury, is an injury to the brain caused by an external force. TBI can be classified based on severity ranging from mild traumatic brain injury (mTBI/concussion) to severe traumatic brain injury. TBI can also be characterized based on mechanism or other features. Head injury is a broader category that may involve damage to other structures such as the scalp and skull. TBI can result in physical, cognitive, social, emotional and behavioral symptoms, and outcomes can range from complete recovery to permanent disability or death.
Closed-head injury is a type of traumatic brain injury in which the skull and dura mater remain intact. Closed-head injuries are the leading cause of death in children under 4 years old and the most common cause of physical disability and cognitive impairment in young people. Overall, closed-head injuries and other forms of mild traumatic brain injury account for about 75% of the estimated 1.7 million brain injuries that occur annually in the United States. Brain injuries such as closed-head injuries may result in lifelong physical, cognitive, or psychological impairment and, thus, are of utmost concern with regards to public health.
Cerebral contusion, Latin: contusio cerebri, a form of traumatic brain injury, is a bruise of the brain tissue. Like bruises in other tissues, cerebral contusion can be associated with multiple microhemorrhages, small blood vessel leaks into brain tissue. Contusion occurs in 20–30% of severe head injuries. A cerebral laceration is a similar injury except that, according to their respective definitions, the pia-arachnoid membranes are torn over the site of injury in laceration and are not torn in contusion. The injury can cause a decline in mental function in the long term and in the emergency setting may result in brain herniation, a life-threatening condition in which parts of the brain are squeezed past parts of the skull. Thus treatment aims to prevent dangerous rises in intracranial pressure, the pressure within the skull.
Post-concussion syndrome (PCS), also known as persisting symptoms after concussion, is a set of symptoms that may continue for weeks, months, or years after a concussion. PCS is medically classified as a mild traumatic brain injury (TBI). About 35% of people with concussion experience persistent or prolonged symptoms 3 to 6 months after injury. Prolonged concussion is defined as having concussion symptoms for over four weeks following the first accident in youth and for weeks or months in adults.
Chronic traumatic encephalopathy (CTE) is a neurodegenerative disease linked to repeated trauma to the head. The encephalopathy symptoms can include behavioral problems, mood problems, and problems with thinking. The disease often gets worse over time and can result in dementia.
Intraventricular hemorrhage (IVH), also known as intraventricular bleeding, is a bleeding into the brain's ventricular system, where the cerebrospinal fluid is produced and circulates through towards the subarachnoid space. It can result from physical trauma or from hemorrhagic stroke.
Post-traumatic epilepsy (PTE) is a form of acquired epilepsy that results from brain damage caused by physical trauma to the brain. A person with PTE experiences repeated post-traumatic seizures more than a week after the initial injury. PTE is estimated to constitute 5% of all cases of epilepsy and over 20% of cases of acquired epilepsy.
Post-traumatic amnesia (PTA) is a state of confusion that occurs immediately following a traumatic brain injury (TBI) in which the injured person is disoriented and unable to remember events that occur after the injury. The person may be unable to state their name, where they are, and what time it is. When continuous memory returns, PTA is considered to have resolved. While PTA lasts, new events cannot be stored in the memory. About a third of patients with mild head injury are reported to have "islands of memory", in which the patient can recall only some events. During PTA, the patient's consciousness is "clouded". Because PTA involves confusion in addition to the memory loss typical of amnesia, the term "post-traumatic confusional state" has been proposed as an alternative.
Post-traumatic seizures (PTS) are seizures that result from traumatic brain injury (TBI), brain damage caused by physical trauma. PTS may be a risk factor for post-traumatic epilepsy (PTE), but a person having a seizure or seizures due to traumatic brain injury does not necessarily have PTE, which is a form of epilepsy, a chronic condition in which seizures occur repeatedly. However, "PTS" and "PTE" may be used interchangeably in medical literature.
Primary and secondary brain injury are ways to classify the injury processes that occur in brain injury. In traumatic brain injury (TBI), primary brain injury occurs during the initial insult, and results from displacement of the physical structures of the brain. Secondary brain injury occurs gradually and may involve an array of cellular processes. Secondary injury, which is not caused by mechanical damage, can result from the primary injury or be independent of it. The fact that people sometimes deteriorate after brain injury was originally taken to mean that secondary injury was occurring. It is not well understood how much of a contribution primary and secondary injuries respectively have to the clinical manifestations of TBI.
Disorders of consciousness are medical conditions that inhibit consciousness. Some define disorders of consciousness as any change from complete self-awareness to inhibited or absent self-awareness and arousal. This category generally includes minimally conscious state and persistent vegetative state, but sometimes also includes the less severe locked-in syndrome and more severe but rare chronic coma. Differential diagnosis of these disorders is an active area of biomedical research. Finally, brain death results in an irreversible disruption of consciousness. While other conditions may cause a moderate deterioration or transient interruption of consciousness, they are not included in this category.
A sports-related traumatic brain injury is a serious accident which may lead to significant morbidity or mortality. Traumatic brain injury (TBI) in sports are usually a result of physical contact with another person or stationary object, These sports may include boxing, gridiron football, field/ice hockey, lacrosse, martial arts, rugby, soccer, wrestling, auto racing, cycling, equestrian, rollerblading, skateboarding, skiing or snowboarding.
Childhood acquired brain injury (ABI) is the term given to any injury to the brain that occurs during childhood but after birth and the immediate neonatal period. It excludes injuries sustained as a result of genetic or congenital disorder. It also excludes those resulting from birth traumas such as hypoxia or conditions such as foetal alcohol syndrome. It encompasses both traumatic and non-traumatic injuries.
Sleep disorder is a common repercussion of traumatic brain injury (TBI). It occurs in 30%-70% of patients with TBI. TBI can be distinguished into two categories, primary and secondary damage. Primary damage includes injuries of white matter, focal contusion, cerebral edema and hematomas, mostly occurring at the moment of the trauma. Secondary damage involves the damage of neurotransmitter release, inflammatory responses, mitochondrial dysfunctions and gene activation, occurring minutes to days following the trauma. Patients with sleeping disorders following TBI specifically develop insomnia, sleep apnea, narcolepsy, periodic limb movement disorder and hypersomnia. Furthermore, circadian sleep-wake disorders can occur after TBI.
↑ Valadka AB (2004). "Injury to the cranium". In Moore EJ, Feliciano DV, Mattox KL (eds.). Trauma. New York: McGraw-Hill, Medical Pub. Division. pp.385–406. ISBN0-07-137069-2. Retrieved 2008-08-15.
↑ Oliveros-Juste A, Bertol V, Oliveros-Cid A (2002). "Preventive prophylactic treatment in posttraumatic epilepsy". Revista de Neurología (in Spanish). 34 (5): 448–459. doi:10.33588/rn.3405.2001439. PMID12040514.
This page is based on this Wikipedia article Text is available under the CC BY-SA 4.0 license; additional terms may apply. Images, videos and audio are available under their respective licenses.