
The medulla oblongata or simply medulla is a long stem-like structure which makes up the lower part of the brainstem. It is anterior and partially inferior to the cerebellum. It is a cone-shaped neuronal mass responsible for autonomic (involuntary) functions, ranging from vomiting to sneezing. The medulla contains the cardiac, respiratory, vomiting and vasomotor centers, and therefore deals with the autonomic functions of breathing, heart rate and blood pressure as well as the sleep wake cycle.
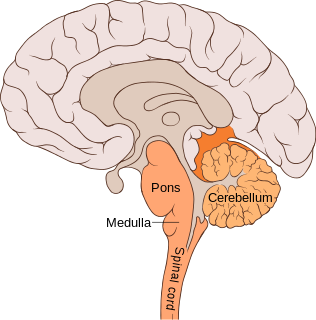
The pons is part of the brainstem that in humans and other bipeds lies inferior to the midbrain, superior to the medulla oblongata and anterior to the cerebellum.
The brainstem is the posterior stalk-like part of the brain that connects the cerebrum with the spinal cord. In the human brain the brainstem is composed of the midbrain, the pons, and the medulla oblongata. The midbrain is continuous with the thalamus of the diencephalon through the tentorial notch, and sometimes the diencephalon is included in the brainstem.

The internal capsule is a white matter structure situated in the inferomedial part of each cerebral hemisphere of the brain. It carries information past the basal ganglia, separating the caudate nucleus and the thalamus from the putamen and the globus pallidus. The internal capsule contains both ascending and descending axons, going to and coming from the cerebral cortex. It also separates the caudate nucleus and the putamen in the dorsal striatum, a brain region involved in motor and reward pathways.

Lateral medullary syndrome is a neurological disorder causing a range of symptoms due to ischemia in the lateral part of the medulla oblongata in the brainstem. The ischemia is a result of a blockage most commonly in the vertebral artery or the posterior inferior cerebellar artery. Lateral medullary syndrome is also called Wallenberg's syndrome, posterior inferior cerebellar artery (PICA) syndrome and vertebral artery syndrome.
Medial medullary syndrome, also known as inferior alternating syndrome, hypoglossal alternating hemiplegia, lower alternating hemiplegia, or Dejerine syndrome, is a type of alternating hemiplegia characterized by a set of clinical features resulting from occlusion of the anterior spinal artery. This results in the infarction of medial part of the medulla oblongata.

Ophthalmoparesis refers to weakness (-paresis) or paralysis (-plegia) of one or more extraocular muscles which are responsible for eye movements. It is a physical finding in certain neurologic, ophthalmologic, and endocrine disease.
Abnormal posturing is an involuntary flexion or extension of the arms and legs, indicating severe brain injury. It occurs when one set of muscles becomes incapacitated while the opposing set is not, and an external stimulus such as pain causes the working set of muscles to contract. The posturing may also occur without a stimulus. Since posturing is an important indicator of the amount of damage that has occurred to the brain, it is used by medical professionals to measure the severity of a coma with the Glasgow Coma Scale and the Pediatric Glasgow Coma Scale.
The posterior cerebral artery (PCA) is one of a pair of arteries that supply oxygenated blood to the occipital lobe, part of the back of the human brain. The two arteries originate from the distal end of the basilar artery, where it bifurcates into the left and right posterior cerebral arteries. These anastomose with the middle cerebral arteries and internal carotid arteries via the posterior communicating arteries.

The posterior inferior cerebellar artery (PICA) is the largest branch of the vertebral artery. It is one of the three main arteries that supply blood to the cerebellum, a part of the brain. Blockage of the posterior inferior cerebellar artery can result in a type of stroke called lateral medullary syndrome.
The anterior inferior cerebellar artery (AICA) is one of three pairs of arteries that supplies blood to the cerebellum.

Cerebellar peduncles connect the cerebellum to the brain stem. There are six cerebellar peduncles in total, three on each side:

Weber's syndrome, also known as midbrain stroke syndrome or superior alternating hemiplegia, is a form of stroke that affects the medial portion of the midbrain. It involves oculomotor fascicles in the interpeduncular cisterns and cerebral peduncle so it characterizes the presence of an ipsilateral lower motor neuron type oculomotor nerve palsy and contralateral hemiparesis or hemiplegia.

Foville's syndrome is caused by the blockage of the perforating branches of the basilar artery in the region of the brainstem known as the pons. It is most frequently caused by vascular disease or tumors involving the dorsal pons.

The medial vestibular nucleus is one of the vestibular nuclei. It is located in the medulla oblongata.
A lateral pontine syndrome is a lesion which is similar to the lateral medullary syndrome, but because it occurs in the pons, it also involves the cranial nerve nuclei of the pons.
A brainstem stroke syndrome falls under the broader category of stroke syndromes, or specific symptoms caused by vascular injury to an area of brain. As the brainstem contains numerous cranial nuclei and white matter tracts, a stroke in this area can have a number of unique symptoms depending on the particular blood vessel that was injured and the group of cranial nerves and tracts that are no longer perfused. Symptoms of a brainstem stroke frequently include sudden vertigo and ataxia, with or without weakness. Brainstem stroke can also cause diplopia, slurred speech and decreased level of consciousness. A more serious outcome is locked-in syndrome.
Alternating hemiplegia is a form of hemiplegia that has an ipsilateral cranial nerve palsies and contralateral hemiplegia or hemiparesis of extremities of the body. The disorder is characterized by recurrent episodes of paralysis on one side of the body. There are multiple forms of alternating hemiplegia, Weber's syndrome, middle alternating hemiplegia, and inferior alternating hemiplegia. This type of syndrome can result from a unilateral lesion in the brainstem affecting both upper motor neurons and lower motor neurons. The muscles that would receive signals from these damaged upper motor neurons result in spastic paralysis. With a lesion in the brainstem, this affects the majority of limb and trunk muscles on the contralateral side due to the upper motor neurons decussation after the brainstem. The cranial nerves and cranial nerve nuclei are also located in the brainstem making them susceptible to damage from a brainstem lesion. Cranial nerves III (Oculomotor), VI (Abducens), and XII (Hypoglossal) are most often associated with this syndrome given their close proximity with the pyramidal tract, the location which upper motor neurons are in on their way to the spinal cord. Damages to these structures produce the ipsilateral presentation of paralysis or palsy due to the lack of cranial nerve decussation before innervating their target muscles. The paralysis may be brief or it may last for several days, many times the episodes will resolve after sleep. Some common symptoms of alternating hemiplegia are mental impairment, gait and balance difficulties, excessive sweating and changes in body temperature.

Raymond–Céstan syndrome is caused by blockage of the long circumferential branches of the basilar artery. It was described by Fulgence Raymond and Étienne Jacques Marie Raymond Céstan. Along with other related syndromes such as Millard–Gubler syndrome, Foville's syndrome, and Weber's syndrome, the description was instrumental in establishing important principles in brain-stem localization.

