Related Research Articles
Obstetrics is the field of study concentrated on pregnancy, childbirth and the postpartum period. As a medical specialty, obstetrics is combined with gynecology under the discipline known as obstetrics and gynecology (OB/GYN), which is a surgical field.

Obstetric ultrasonography, or prenatal ultrasound, is the use of medical ultrasonography in pregnancy, in which sound waves are used to create real-time visual images of the developing embryo or fetus in the uterus (womb). The procedure is a standard part of prenatal care in many countries, as it can provide a variety of information about the health of the mother, the timing and progress of the pregnancy, and the health and development of the embryo or fetus.
Fetal distress, also known as non-reassuring fetal status, is a condition during pregnancy or labor in which the fetus shows signs of inadequate oxygenation. Due to its imprecision, the term "fetal distress" has fallen out of use in American obstetrics. The term "non-reassuring fetal status" has largely replaced it. It is characterized by changes in fetal movement, growth, heart rate, and presence of meconium stained fluid.

Placenta praevia is when the placenta attaches inside the uterus but in an abnormal position near or over the cervical opening. Symptoms include vaginal bleeding in the second half of pregnancy. The bleeding is bright red and tends not to be associated with pain. Complications may include placenta accreta, dangerously low blood pressure, or bleeding after delivery. Complications for the baby may include fetal growth restriction.

Umbilical cord prolapse is when the umbilical cord comes out of the uterus with or before the presenting part of the baby. The concern with cord prolapse is that pressure on the cord from the baby will compromise blood flow to the baby. It usually occurs during labor but can occur anytime after the rupture of membranes.

Large for gestational age (LGA) is a term used to describe infants that are born with an abnormally high weight, specifically in the 90th percentile or above, compared to other babies of the same developmental age. Macrosomia is a similar term that describes excessive birth weight, but refers to an absolute measurement, regardless of gestational age. Typically the threshold for diagnosing macrosomia is a body weight of between 4,000 and 4,500 grams, or more, measured at birth, but there are difficulties reaching a universal agreement of this definition.

Obstructed labour, also known as labour dystocia, is when the baby does not exit the pelvis during childbirth due to being physically blocked, despite the uterus contracting normally. Complications for the baby include not getting enough oxygen which may result in death. It increases the risk of the mother getting an infection, having uterine rupture, or having post-partum bleeding. Long-term complications for the mother include obstetrical fistula. Obstructed labour is said to result in prolonged labour, when the active phase of labour is longer than 12 hours.

Shoulder dystocia is when, after vaginal delivery of the head, the baby's anterior shoulder gets caught above the mother's pubic bone. Signs include retraction of the baby's head back into the vagina, known as "turtle sign". Complications for the baby may include brachial plexus injury, or clavicle fracture. Complications for the mother may include vaginal or perineal tears, postpartum bleeding, or uterine rupture.

Complications of pregnancy are health problems that are related to pregnancy. Complications that occur primarily during childbirth are termed obstetric labor complications, and problems that occur primarily after childbirth are termed puerperal disorders. Severe complications of pregnancy, childbirth, and the puerperium are present in 1.6% of mothers in the US, and in 1.5% of mothers in Canada. In the immediate postpartum period (puerperium), 87% to 94% of women report at least one health problem. Long-term health problems are reported by 31% of women.
Postterm pregnancy is when a woman has not yet delivered her baby after 42 weeks of gestation, two weeks beyond the typical 40-week duration of pregnancy. Postmature births carry risks for both the mother and the baby, including fetal malnutrition, meconium aspiration syndrome, and stillbirths. After the 42nd week of gestation, the placenta, which supplies the baby with nutrients and oxygen from the mother, starts aging and will eventually fail. Postterm pregnancy is a reason to induce labor.

Maternal–fetal medicine (MFM), also known as perinatology, is a branch of medicine that focuses on managing health concerns of the mother and fetus prior to, during, and shortly after pregnancy.

The McRoberts maneuver is an obstetrical maneuver used to assist in childbirth. It is named after William A. McRoberts, Jr. It is employed in case of shoulder dystocia during childbirth and involves hyperflexing the mother's legs tightly to her abdomen. It is effective due to the increased mobility at the sacroiliac joint during pregnancy, allowing rotation of the pelvis and facilitating the release of the fetal shoulder. If this maneuver does not succeed, an assistant applies pressure on the lower abdomen. Current guidelines strongly recommend against pulling on the infants head, as this could lead to brachial plexus injury. Instead, support while keeping the neck straight is indicated. The technique is effective in about 42% of cases. Note that suprapubic pressure and McRobert's maneuver together will resolve 90% of cases.
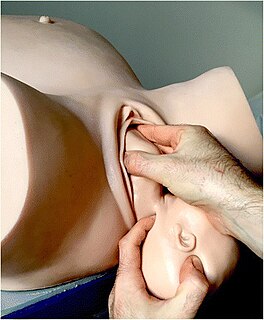
Wood's screw maneuver is practiced in obstetrics when dealing with shoulder dystocia – a condition in which the fetal shoulders cannot easily pass through the vagina. In this maneuver the anterior shoulder is pushed towards the baby's chest, and the posterior shoulder is pushed towards the baby's back, making the baby's head somewhat face the mother's rectum.
Anterior shoulder in obstetrics refers to that shoulder of the fetus that faces the pubic symphysis of the mother during delivery. Depending upon the original position of the fetus, either the left or the right shoulder can be the anterior shoulder. It is known as the anterior shoulder as it faces the anterior of the mother. This distinction between the anterior and the posterior shoulder is important as the anterior shoulder is delivered first.
Posterior shoulder in obstetrics refers to the shoulder of the fetus other than the anterior shoulder. Thus, the posterior shoulder faces the rectum of the mother during delivery. Whether left or the right shoulder becomes the posterior shoulder is dependent upon the original position of the fetus. It is known as the posterior shoulder as it faces the posterior of the mother. This distinction between the anterior and the posterior shoulder is important as the anterior shoulder is delivered first.

A shoulder presentation refers to a malpresentation at childbirth where the baby is in a transverse lie, thus the leading part is an arm, a shoulder, or the trunk. While a baby can be delivered vaginally when either the head or the feet/buttocks are the leading part, it usually cannot be expected to be delivered successfully with a shoulder presentation unless a cesarean section (C/S) is performed.
An obstetric labor complication is a difficulty or abnormality that arises during the process of labor or delivery.

Prolonged labor is the inability of a woman to proceed with childbirth upon going into labor. Prolonged labor typically lasts over 20 hours for first time mothers, and over 14 hours for women that have already had children. Failure to progress can take place during two different phases; the latent phase and active phase of labor. The latent phase of labor can be emotionally tiring and cause fatigue, but it typically does not result in further problems. The active phase of labor, on the other hand, if prolonged, can result in long term complications.
Rubin maneuver, also known as reverse Wood's screw maneuver, is a secondary, rotational maneuver to deliver the baby in case of shoulder dystocia. The first Rubin maneuver is the rotation of anterior shoulder under pubic symphysis by giving suprapubic pressure. As a result, the bisacromial diameter is rotated from anteroposterior to oblique lie. The obstetrician uses the right hand for performing this maneuver if the foetus is facing mother's right side, and vice versa. During first Rubin maneuver, fundal pressure should not be applied because it may cause uterine rupture or further impaction of the shoulder. If the first Rubin maneuver does not disengage the shoulder, second Rubin maneuver is performed.
Emergency childbirth is the birth of an infant in places or situations other than what was planned. In most cases the location of childbirth is planned ahead of time and may be at home, a hospital, a medical facility or a birthing center. In other situations, the birth occurs on the way to these facilities. Oftentimes, no trained medical personnel are present, other times there may be police or other first responders. Emergency measures for delivery are indicated when childbirth is imminent.
References
- ↑ Baxley EG, Gobbo RW (April 2004). "Shoulder dystocia". Am Fam Physician. 69 (7): 1707–14. PMID 15086043.
- 1 2 Sandberg, EC (June 15, 1985). "The Zavanelli maneuver: a potentially revolutionary method for the resolution of shoulder dystocia". American Journal of Obstetrics and Gynecology. 152 (4): 479–84. doi:10.1016/s0002-9378(85)80161-7. PMID 4014342.
- ↑ Kish, Karen; Joseph V. Collea (2003). "Malpresentation & Cord Prolapse (Chapter 21)". In Alan H. DeCherney (ed.). Current Obstetric & Gynecologic Diagnosis & Treatment. Lauren Nathan (Ninth ed.). Lange/McGraw-Hill. p. 382. ISBN 0-07-118207-1.
- 1 2 Gabbe, Steven G. (January 2012). Obstetrics : normal and problem pregnancies (6th ed.). Philadelphia: Elsevier/Saunders. p. 412. ISBN 9781437719352.
- ↑ Baskett, Thomas F. (2019). "Zavanelli, William Angelo (b. 1926)". Eponyms and Names in Obstetrics and Gynaecology. Cambridge University Press. pp. 461–2. doi:10.1017/9781108421706.369. ISBN 9781108336710.