
Otorhinolaryngology is a surgical subspeciality within medicine that deals with the surgical and medical management of conditions of the head and neck. Doctors who specialize in this area are called otorhinolaryngologists, otolaryngologists, head and neck surgeons, or ENT surgeons or physicians. Patients seek treatment from an otorhinolaryngologist for diseases of the ear, nose, throat, base of the skull, head, and neck. These commonly include functional diseases that affect the senses and activities of eating, drinking, speaking, breathing, swallowing, and hearing. In addition, ENT surgery encompasses the surgical management of cancers and benign tumors and reconstruction of the head and neck as well as plastic surgery of the face, scalp, and neck.

Plastic surgery is a surgical specialty involving the restoration, reconstruction, or alteration of the human body. It can be divided into two main categories: reconstructive surgery and cosmetic surgery. Reconstructive surgery includes craniofacial surgery, hand surgery, microsurgery, and the treatment of burns. While reconstructive surgery aims to reconstruct a part of the body or improve its functioning, cosmetic surgery aims to improve the appearance of it. A comprehensive definition of plastic surgery has never been established, because it has no distinct anatomical object and thus overlaps with practically all other surgical specialties. An essential feature of plastic surgery is that it involves the treatment of conditions that require or may require tissue relocation skills.

The brachial plexus is a network of nerves formed by the anterior rami of the lower four cervical nerves and first thoracic nerve. This plexus extends from the spinal cord, through the cervicoaxillary canal in the neck, over the first rib, and into the armpit, it supplies afferent and efferent nerve fibers to the chest, shoulder, arm, forearm, and hand.
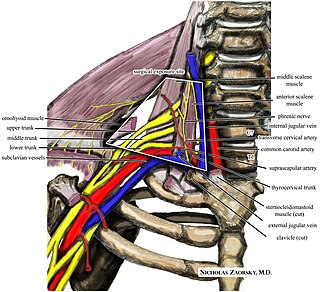
Thoracic outlet syndrome (TOS) is a condition in which there is compression of the nerves, arteries, or veins in the superior thoracic aperture, the passageway from the lower neck to the armpit, also known as the thoracic outlet. There are three main types: neurogenic, venous, and arterial. The neurogenic type is the most common and presents with pain, weakness, paraesthesia, and occasionally loss of muscle at the base of the thumb. The venous type results in swelling, pain, and possibly a bluish coloration of the arm. The arterial type results in pain, coldness, and pallor of the arm.

An eyelid is a thin fold of skin that covers and protects an eye. The levator palpebrae superioris muscle retracts the eyelid, exposing the cornea to the outside, giving vision. This can be either voluntarily or involuntarily. "Palpebral" means relating to the eyelids. Its key function is to regularly spread the tears and other secretions on the eye surface to keep it moist, since the cornea must be continuously moist. They keep the eyes from drying out when asleep. Moreover, the blink reflex protects the eye from foreign bodies. A set of specialized hairs known as lashes grow from the upper and lower eyelid margins to further protect the eye from dust and debris.

The musculocutaneous nerve is a mixed branch of the lateral cord of the brachial plexus derived from cervical spinal nerves C5-C7. It arises opposite the lower border of the pectoralis major. It provides motor innervation to the muscles of the anterior compartment of the arm: the coracobrachialis, biceps brachii, and brachialis. It provides sensory innervation to the lateral forearm. It courses through the anterior part of the arm, terminating 2 cm above elbow; after passing the lateral edge of the tendon of biceps brachii it is becomes known as the lateral cutaneous nerve of the forearm.

Microsurgery is a general term for surgery requiring an operating microscope. The most obvious developments have been procedures developed to allow anastomosis of successively smaller blood vessels and nerves which have allowed transfer of tissue from one part of the body to another and re-attachment of severed parts. Microsurgical techniques are utilized by several specialties today, such as general surgery, ophthalmology, orthopedic surgery, gynecological surgery, otolaryngology, neurosurgery, oral and maxillofacial surgery, endodontic microsurgery, plastic surgery, podiatric surgery and pediatric surgery.

A facelift, technically known as a rhytidectomy, is a type of cosmetic surgery procedure intended to give a more youthful facial appearance. There are multiple surgical techniques and exercise routines. Surgery usually involves the removal of excess facial skin, with or without the tightening of underlying tissues, and the redraping of the skin on the patient's face and neck. Exercise routines tone underlying facial muscles without surgery. Surgical facelifts are effectively combined with eyelid surgery (blepharoplasty) and other facial procedures and are typically performed under general anesthesia or deep twilight sleep.
A brachial plexus injury (BPI), also known as brachial plexus lesion, is an injury to the brachial plexus, the network of nerves that conducts signals from the spinal cord to the shoulder, arm and hand. These nerves originate in the fifth, sixth, seventh and eighth cervical (C5–C8), and first thoracic (T1) spinal nerves, and innervate the muscles and skin of the chest, shoulder, arm and hand.
The terms free flap, free autologous tissue transfer and microvascular free tissue transfer are synonymous terms used to describe the "transplantation" of tissue from one site of the body to another, in order to reconstruct an existing defect. "Free" implies that the tissue is completely detached from its blood supply at the original location and then transferred to another location and the circulation in the tissue re-established by anastomosis of artery(s) and vein(s). This is in contrast to a "pedicled" flap in which the tissue is left partly attached to the donor site ("pedicle") and simply transposed to a new location; keeping the "pedicle" intact as a conduit to supply the tissue with blood.
The lateral pectoral nerve arises from the lateral cord of the brachial plexus, and through it from the C5-7.
Harry J. Buncke was an American plastic surgeon who has been called "The Father of Microsurgery" for his contributions in the history and development of reconstructive microsurgical procedures. He is a past president of the American Society for Surgery of the Hand, the International Society of Reconstructive Microsurgery, and the American Association of Plastic Surgery. He served as a clinical professor of surgery at both Stanford University and the University of California - San Francisco. He was the author of 15 movies and television tapes, four surgical textbooks, and more than 400 peer-reviewed publications.

Replantation or reattachment is defined as the surgical reattachment of a body part that has been completely cut from the body.
Degloving occurs when skin and the fat below it, the subcutaneous tissue, are torn away from the underlying anatomical structures they are normally attached to. Normally the subcutaneous tissue layer is attached to the fibrous layer that covers muscles known as deep fascia.
Jersey finger, also known as rugby finger, is a finger-related tendon injury that is common in sport and can result in permanent loss of flexion of the end of the finger if not surgically repaired. The injury is common when one player grabs another's jersey with the tips of one or more fingers while that player is pulling or running away. It is the most common closed flexor tendon injury and occurs in the ring finger in 75% of cases.
Flap surgery is a technique in plastic and reconstructive surgery where tissue with an intact blood supply is lifted from a donor site and moved to a recipient site. Flaps are distinct from grafts, which do not have an intact blood supply and relies on the growth of new blood vessels. Flaps are done to fill a defect such as a wound resulting from injury or surgery when the remaining tissue is unable to support a graft, or to rebuild more complex anatomic structures like breasts or jaws.

Dental avulsion is the complete displacement of a tooth from its socket in alveolar bone owing to trauma which can be caused by a fall, road traffic accident, assault, sports, or occupational injury. Typically, a tooth is held in place by the periodontal ligament, which becomes torn when the tooth is knocked out.
The cheek constitutes the facial periphery and plays a key role in the maintenance of oral competence and mastication. It is also involved in the facial manifestation of human emotion and supports neighboring primary structures.
A penile injury is a medical emergency that afflicts the penis. Common injuries include fracture, avulsion injury, strangulation, entrapment, and amputation.
Tooth replantation is a form of restorative dentistry in which an avulsed or luxated tooth is reinserted and secured into its socket through a combination of dental procedures. The purposes of tooth replantation is to resolve tooth loss and preserve the natural landscape of the teeth. Whilst variations of the procedure exist including, Allotransplantation, where a tooth is transferred from one individual to another individual of the same species. It is a largely defunct practice due to the improvements made within the field of dentistry and due to the risks and complications involved including the transmission of diseases such as syphilis, histocompatibility, as well as the low success rate of the procedure, has resulted in its practice being largely abandoned. Autotransplantation, otherwise known as intentional replantation in dentistry, is defined as the surgical movement of a tooth from one site on an individual to another location in the same individual. While rare, modern dentistry uses replantation as a form of proactive care to prevent future complications and protect the natural dentition in cases where root canal and surgical endodontic treatments are problematic. In the modern context, tooth replantation most often refers to reattachment of an avulsed or luxated permanent tooth into its original socket.
